

Year: 2012 Vol. 78 Ed. 5 - (5º)
Artigo Original
Pages: 27 to 37
 PDF PT
PDF PT  PDF EN
PDF ENAre parents aware of their children's hearing complaints?
Author(s): Keila Alessandra Baraldi Knobel1; Maria Cecília Marconi Pinheiro Lima2
DOI: 10.5935/1808-8694.20120005
Keywords: child, hearing, hyperacusis, parents, tinnitus.
Abstract:
The accuracy of parents' impressions about their child's hearing status is variable and may not correspond to the child's complaints.
AIM: To investigate children's self-reported hearing symptoms and parents' impressions about it.
METHODS: 477 children (2nd to 5th grades of elementary schools) were interviewed and parents answered a survey at home. There were 393 matches between the children's interview and the parent's survey.
RESULTS: 29% of the children reported trouble in understanding what people said, 36.1% had history of 1-3 ear infections, 12.7% had four or more ear infections, 21.7% had continuous tinnitus (positive association with history of exposure to loud sounds, p = 0.0007), 3.8% had pulsatile tinnitus and 2.9% had auditory hallucinations. 28.5% of the children were annoyed by loud sounds (associated with tinnitus, p = 0.0142, and gender, p = 0.0029) 10.4% had had audiological tests, and the determinant factors were history of ear infections (p < 0.001) and parents' concern about their child's hearing (p = 0.043). Parents and their own child's responses were significantly different.
CONCLUSIONS: Children's auditory complaints were prevalent and relevant, but most of them had never had an audiological evaluation and most parents were not aware of their child's complaints. Sound intolerances and auditory hallucinations should be considered in clinical and audiological examinations.
![]()
INTRODUCTION
Communication occurs in many ways, but oral communication is the main mode of the educational system. For this reason, early identification of any type or level of hearing loss gives students the opportunity of an early intervention to prevent negative effects of the hearing loss on the child's speech, language, learning, and academic outcomes1,2.
The prevalence of hearing impairment in children depends on how rigorous the criteria are to define it1,3,4 and on living conditions and access to health care2,5. According to the World Health Organization3, the prevalence of hearing impairment among school aged children ranges from 0.05% to 7.7%, but more recent studies found prevalence of 14%6, 14.9%7, 18.4%8, 19.5%9 and 24%10. In summary, a considerable number of children face hearing difficulties and need to be identified and receive proper assistance. In countries where hearing screening for school-aged children is not a routine, children can only count on adults' attention. However, studies have shown that parental concern for their child's hearing has low sensitivity and very low positive predictive values for detecting hearing loss, especially minimal or mild ones4,11,12.
Another auditory symptom that is common among children is tinnitus13. Tinnitus is a phantom auditory perception, since it is a perception that is not related to an external source14-16. The prevalence of tinnitus among children varies from 6% to 59%6. Despite the disclosed prevalence data, attributed to important differences in methods of data collection, diagnostic criteria, and age groups6, there is a consensus that it is higher among children with otological disorders or history of exposures to loud sounds4,6,17-20. Children seem to be less distressed by tinnitus than adults, but children who complain of tinnitus should be taken seriously, since it may be a sign of an otological condition and can affect children's lives as it is reported to have on adults18.
Auditory hallucination (AH) is a different kind of phantom auditory perception. When the perception has the same qualities as a real one, meaning that the person does not recognize it as a distorted perception, it is called auditory hallucination (AH)21. The prevalence of AH in population based studies with adolescents from the general population is around 6%22,23, although the number of parents who reported hallucinations in their children was less than 1%22. In a follow-up research, Dhossche et al.22 reported that, eight years after they found 6% of adolescents (out of 914) from the general population with self-reported hallucination, no subject was diagnosed with schizophrenia. However, AH were associated with non-psychotic psychiatric problems, such as specific phobias, depressive disorders, substance use disorders, post-traumatic stress disorder and social phobia. Similar development was found in 16 (out of 90) non-psychotic children (5-12 years old) that reported AH in psychiatric clinics24.
Hyperacusis is defined as a decreased sound tolerance to ordinary sounds, even in low intensities25. Annoyance or feeling of displeasure with specific sounds can be called phonophobia (fear of sound) or misophonia (dislike of sound)26. There is scarce published information on the prevalence, possible associated causes and prognosis of decreased sound tolerance in childhood. A link between hyperacusis and tinnitus has been described in adults25-27 and in children28. According to Coelho et al.28 50% of the children who had hyperacusis also reported tinnitus, and of those who did not have hyperacusis, 17.8% reported tinnitus.
In summary, population studies show that a significant number of children have at least one hearing complaint that can potentially cause negative effects on the child's communication, academic outcomes and emotional well-being. The aims of the present study were to evaluate the parents' impressions about their child's hearing, the prevalence of self-reported hearing impairment, tinnitus, AHs and decreased sound tolerance among children attending the 2nd to 5th grades of elementary school and to investigate possible risk factors for the complaints. The present study is part of a larger one that also sought information about children's knowledge, habits, preferences and protective behaviors regarding loud sound exposures29.
METHOD
Design
A prospective cross-sectional study was carried out in elementary schools in Campinas, a southeastern Brazilian town with 1.1 million inhabitants. Data were collected between April 2010 and November 2010.
The survey started after a pilot test with 60 children and their parents. We selected the questions of questionnaire with the children and the questions of the survey to the parents that were most suitable for the research.
Selection criteria
In Campinas there are 72,326 students from 2nd to 5th grades30. Sixty per cent of them are distributed in 98 State Public Schools, 25% in 42 Municipal Schools and 15% in approximately 180 Private Schools. It is important to explain that in Brazil there are free municipal and state public schools and private schools. With few exceptions, public schools have limited educational resources and, for this reason, families with higher incomes usually send their children to private school. Children go to school either during the morning or afternoon. Children from 2nd to 5th grades are 6 to 10 years-old.
The city is divided into five regions. The selection of the schools was made in alphabetical order for each region. After a telephone contact, many school directors refused to receive us. So, the next school in alphabetical order in the same region was contacted. Using these criteria we selected 13 schools: seven State public, three Municipal public schools and three private. In large schools, with more than one class per year, the class was chosen also by letter (2nd, 3rd, 4th and 5th years C, for example). In small schools students either from the morning or from the afternoon period were interviewed.
With these procedures we had a selected sample of 753 children. Children with medical records of mental or psychiatric disabilities were excluded. Parents (mother, father or caretaker) received the informed consent form and a survey (described in assessments) to be filled out at home. Teachers collected the returned forms and questionnaires and gave them to the researcher, who went to the school to make the assessments. The number of interviewed children was 477. Considering the number of the selected sample and the number of interviewed children, the drop-out range was 36.8%. Withdrawals were due to no returns of the informed consent form (71.4%), parental refusals (23.2%), and children's non attendances at school at the day of the interview (5.4%). Because some parents' surveys were returned in blank, there were 393 matches between child's interview and his/her own parent's survey.
Procedure
The interviews with the children were conducted during school-time. All children gave verbal consent and were individually and privately interviewed by the first author in the most silent room available in the school. Care was taken to ensure that children understood the questions and had plenty time to respond. The interviewer did not express either approval or disapproval to the child's answer at any time.
Assessments
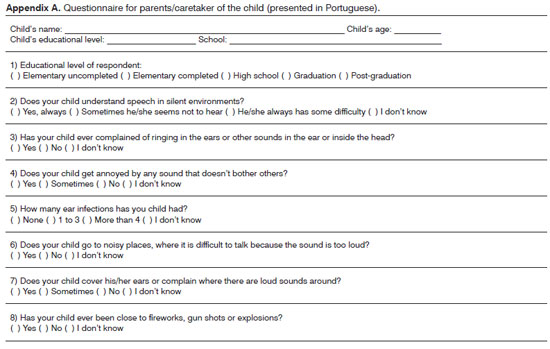
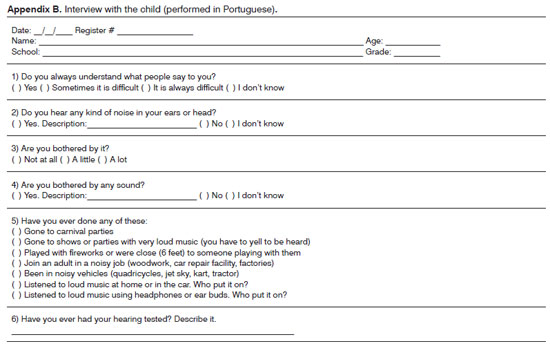
The parents' survey sought information on parental impressions of their child's auditory behavior and complaints, history of exposures to loud sounds, the number of episodes of otitis media and background information (8 items, Appendix A). The children's interview consisted of an open-ended questionnaire, with guideline questions presented orally by the interviewer about demographic information, self-reported trouble hearing in quiet, phantom auditory perceptions, sound annoyance and information about previous hearing tests (5 items, see Appendix B). Many children and adults described their tinnitus as sounds of insects, such as a bee or mosquito, tones and noises. But, to be considered tinnitus, these phantom auditory perceptions must be recognized by the person as "sounds" produced by their own ears or head. On the contrary, if the person does not recognize it as a distorted perception, it is called AHs21. For this reason, children that reported they hear insects, tones or noises around them, but could identify where it came from, believing it to come from somewhere outside themselves, were considered to have AHs. We had not planned a question about the level of annoyance with phantom auditory perceptions, but a discussion of partial results showed its importance. For this reason, only a sub-group of the participants (239 children from state public schools) were answered to this question.
Statistical analysis
There was a content analysis for the questions that included descriptions. Those responses were coded prior to statistical analysis. Statistical analysis was performed by using SAS (version 9.1) and the significance level was 5%.
Homogeneity and other exposure factors were analyzed by using Chi-square Test for percentage differences and Fischer's Exact Test for absolute frequencies (n < 5). Analysis of agreement in measurement comparing children's and parents' questionnaires was accomplished by using the Symmetric Test. It analyses how different the answers were.
Ethics
The present study was approved by the ethics committee of research (number 940/2009). Written consent was obtained from all parents and verbal consent from all children.
RESULTS
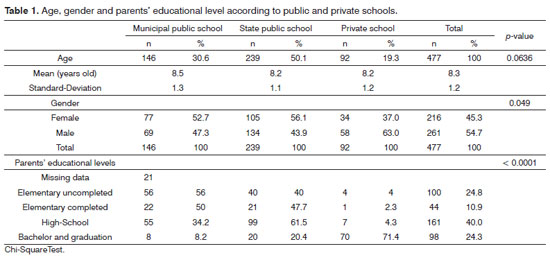
Samples from public and private schools were similar in gender and age, but Chi-Square Test showed a significant difference among schools with regard to parents' educational level (Table 1).
Twenty nine percent of the children reported some trouble understanding what people say, 0.6% said they always had some trouble. According to parents' information, 36.1% of the children had history of one to three ear infections, 12.7% had had four or more ear infections and 2.5% did not know. The number of previous ear infections was not associated with parent's educational level (p = 0.639, Chi Square Test).
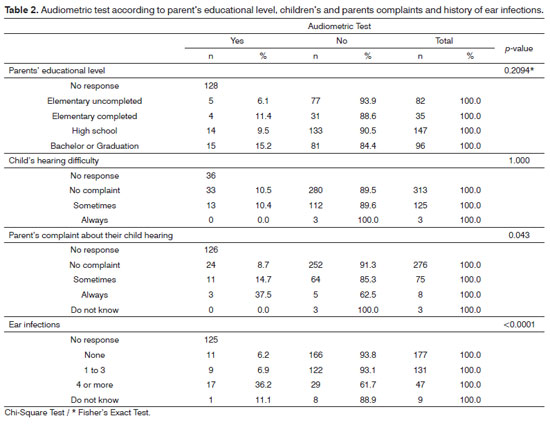
Despite the prevalence of self-reported hearing complaints and history of ear infections, only 10.4% had had an audiometric test, and almost 2/3 of them were from private schools. Table 2 displays the association of the audiometric test taken with parent's educational level, children's and parents' complaints and history of ear infections.
Excluding missing data from 13 children, the number of children with phantom auditory perception was 135 (28.4%). After classifying the perceptions, three categories were found: continuous tinnitus, such as a continuous ring or hum (n = 103/21.7%), pulsatile tinnitus (n = 18/3.8%) and AHs (n = 14/2.9%).
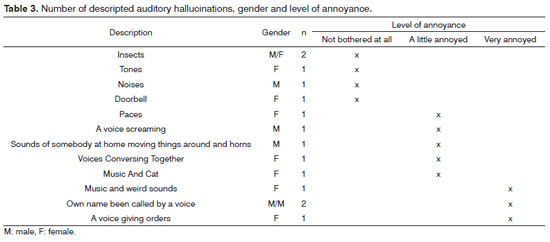
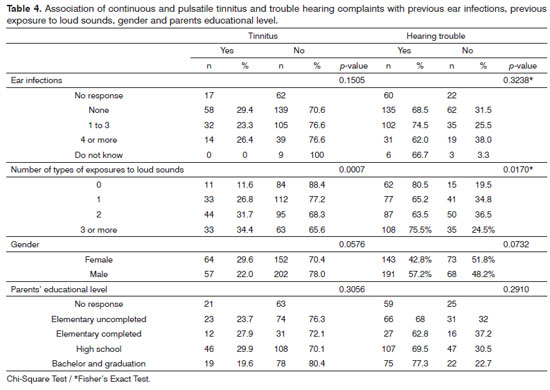
Table 3 provides the number and gender of children and the descriptions of their AHs. Owing to the small number of subjects with AHs, parametric tests were not performed. History of previous ear infections and previous exposure to loud sounds, gender and parents' educational level were examined with a view to investigating their association with complaints of trouble hearing and tinnitus (continuous and pulsatile) (Table 4).
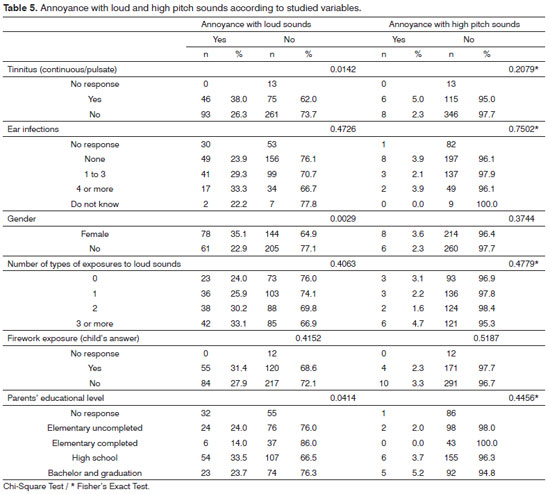
Regarding the question about sounds that bothered the child, 59.4% denied any annoyance with sounds, 28.5% were annoyed by loud sounds (noise or music), 2.9% high pitch sounds, 1.0% body sounds produced by others (snoring, cleaning accumulated mucus in the throat, swallowing), 3.5% scratching sounds (on iron, black-board, polystyrene...) and 4.7% referred to other sounds, such as a broom sweeping, a plastic cup being squeezed, a chair being dragged across the floor, sand-paper, etc.
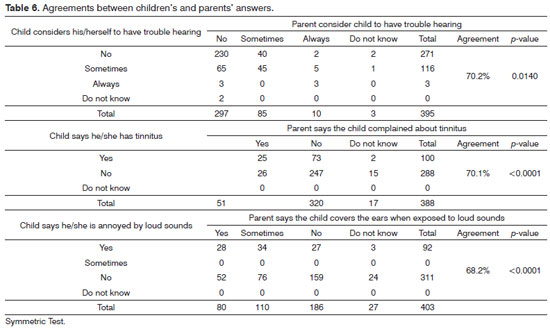
The study of the associations of previous ear infections, previous exposure to loud sounds, tinnitus, gender and parents' educational level with sound annoyance with loud and high pitch sounds is shown in Table 5. Agreements among children's and their own parents' answers are shown in Table 6. Dashed cells refer to agreement among parent and child answers. A symmetric test analyses how different they were.
DISCUSSION
The present study investigated self-reported hearing complaints among Brazilian children attending the 2nd, 3rd, 4th and 5th grades of elementary schools and parents' perceptions about this.
In Brazil, students do not pay to go to public schools. Family incomes were not analyzed, but the significant difference of parents' educational levels between municipal public, state public and private schools (p < 0.0001) seems to be influenced by other socioeconomic variables, such as access to adequate health care, housing, nutrition, etc. For this reason, we decided to analyze the variable parents' educational level across self-reported hearing complaints and not the school "type". Children's age was similar among schools, but there were more boys than girls (p = 0.049), which correspond to the gender distribution in the city for this age range30.
Hearing difficulties
Previous researches associated hearing difficulties to ear infections and lower incomes2,31. Although the majority of the Brazilian children who go to private schools are wealthier than the others, history of previous ear infections was not significantly different between public and private schools (p = 0.2000, Fisher's Exact Test). Contrary to other studies2,32, we did not find an association between children's hearing difficulties and history of ear infections, probably because of differences in methodology. In our study we investigated the self-reported hearing difficulty, not the hearing impairment, evaluated by both studies2,32 using pure-tone audiometry, tympanometry and otoscopy. Also, we gathered the total number of ear infections the child had in his/her life, while they looked for specific data, such as "otitis media treated with antibiotics", "more than three episodes of otitis media in a year"2 and "otorrhea"2,32. Holgers & Pettersson33 found that the risk of subjective hearing loss increases with increasing noise exposure. Although there was an association between hearing difficulties and history of loud sound exposure in our study, it seems that there is a confounding variable affecting the hearing difficulty, since any number of exposures to loud sounds (from none to more than four) resulted in a higher percentage of children with complaints of hearing trouble.
Despite the auditory symptoms, only 10.4% of the children had ever had an audiometric test, with no statistical association with parents' educational level (p = 0.2094) or child's self-reported hearing complaint (p = 1.000). Only if the child was able to describe the hearing test was she considered as ever been evaluated. A previous hearing test was associated with history of ear infection (p < 0.0001) and parent's complaint about their child's hearing (p = 0.043). We did not interrogate parents about why they did or did not take their child for a hearing evaluation. Thus, we cannot say if parents took their child to have a hearing test because they were really worried about their child's auditory behavior or if they expressed their concern with their child's hearing because the child (maybe) failed in a hearing test that was ordered by a health care professional.
The symmetric test pointed to a significant difference between the parents and their own child's answers. In Table 5 we verify that, among the 116 children who had trouble hearing in silence, only 45 (38.8%) had parents that were aware of their difficulty. Though we found 29.6% of children with some hearing complaints (0.6% with more evident trouble) we cannot directly transpose it into actual hearing losses, since we did not evaluate their hearing and predictive values of parental suspicion of hearing impairment are yet to be discussed4,34-36. Despite those weak points, we totally agree with Cone et al.4 that a caregiver's concern with regards a child's hearing development is enough reason to prompt a formal hearing assessment.
Tinnitus and AHs
Estimates of prevalence of tinnitus and decreased sound tolerance depend on the definitions adopted and on the way the questions are presented to the child. In order to have a better picture of those symptoms, we tried to identify all auditory phantom perceptions and sound annoyances and then we classified them. Tinnitus was reported by 28.4% of the children and was similar to the findings of Mills et al. (29%)19 and Raj-Koziak et al. (33%)37, but much higher than the findings of 9.2% from Holgers17 (12%) study and lower than Coelho et al. (37.5%)6 for the same age group.
We observed a significant association between tinnitus and the history of loud sound exposures6,17,38, which is worrying, since there is evidence that tinnitus may be an early warning sign of noise induced hearing loss20.
Only 51% of the parents reported that their child had tinnitus. So, despite the fact that half of the children did not talk to their parents about their tinnitus, we consider that our findings cast doubt on the assumption that it is rare for children to complain spontaneously of tinnitus to their parents19,37,39.
In our sample, 13 children (2.7%) reported auditory phantom perceptions that were compatible with AHs (Table 3). It is less than reported by other studies22-24, but it still shows that the symptom is not uncommon in childhood. Only one child had verbal hostile AHs, in which she told that she heard "her dead uncle giving orders to her". Another child reported that she heard voices conversing together, but she said it was not possible to understand anything; it was more like a bubble noise. So, except for one child, the other AHs in this sample were predominantly non-threatening24,40.
Sound annoyance
We identified almost half of the children with some annoyance with sounds. Of course, our data is not enough to diagnose children with hyperacusis nor phonophobia, but our results are generally the same as those obtained by Coelho et al.28, who evaluated the Loudness Discomfort Level (LDL) of children within the same age group. Their study indicated that, among the children with LDL in the lowest 5th percentile (lower than 90 dB HL), 42% were bothered by sounds, 3.2% had hyperacusis and 9% had phonophobia. Our study also supports that there is an association between tinnitus and annoyance with sounds (p = 0.0142) and that there is a higher occurrence of the complaint among girls (p = 0.0029), both found previously in studies with children28 and adults41.
Limitations
One limitation of our study was the drop-out range of 36.8%, which decreases the epidemiological power of the study. Nevertheless, drop-out was similar in private and public schools and did not change the general age and gender distribution.
The attempt to find possible relations between hearing complaints and the number of types of noise exposures may have been limited because children self-reported noise exposures and we have no data about how frequent or infrequent those exposures were. It is also possible that some children did not remember taking an audiometric test.
Future directions
Parental and teacher vigilance over children's hearing behavior and sensitive hearing screening programs are essential to identify children that should take a complete ear and hearing evaluation. Besides, we need to encourage children to talk about themselves or, at least, we have to start listening to their complaints and it follows that if the child has a hearing complaint, tinnitus, AHs or annoyance with sounds, something has to be done.
We also support the urgent need of hearing screening programs and pediatric ear health assistance for school-aged children. Ideally, hearing and audiological examinations should be incorporated into routine pediatric visits, especially for children of literacy age.
CONCLUSION
Difficulties in understanding what people say, decreased sound tolerance, tinnitus and hearing hallucinations are common complaints among children. Despite the relevance of those auditory complaints, the majority of the parents were not aware of their child's complaint, and even when they were, most of the children did not take an audiological evaluation. Sound intolerances and AHs should be considered in clinical and audiological examinations.
ACKNOWLEDGEMENTS
This work was supported by the Fundação de Amparo à Pesquisa de São Paulo (Fapesp 2009/15825-0). The funding organization had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript. Statistical analysis performed by Sirlei Moraes was much appreciated.
REFERENCES
1. Bess FH, Dodd-Murphy J, Parker RA. Children with minimal sensorineural hearing loss: prevalence, educational performance, and functional status. Ear Hear. 1998;19(5):339-54.
2. Czechowicz JA, Messner AH, Alarcon-Matutti E, Alarcon J, Quinones-Calderon G, Montano S, et al. Hearing impairment and poverty: the epidemiology of ear disease in Peruvian schoolchildren. Otolaryngol Head Neck Surg J. 2010;142(2):272-7.
3. Mathers C, Smith A, Concha M. Global burden of hearing loss in the year 20002003: Available from: http://www.who.int/healthinfo/statistics/bod_hearingloss.pdf
4. Cone BK, Wake M, Tobin S, Poulakis Z, Rickards FW. Slight-mild sensorineural hearing loss in children: audiometric, clinical, and risk factor profiles. Ear Hear J. 2010;31(2):202-12.
5. Evans GW, Marcynyszyn LA. Environmental justice, cumulative environmental risk, and health among low- and middle-income children in upstate New York. Am J Public Health. 2004;94(11):1942-4.
6. Coelho CB, Sanchez TG, Tyler R. Tinnitus in children and associated risk factors. Progr Brain Res. 2007;166:179-91.
7. Niskar AS, Kieszak SM, Holmes AE, Esteban E, Rubin C, Brody DJ. Estimated prevalence of noise-induced hearing threshold shifts among children 6 to 19 years of age: the Third National Health and Nutrition Examination Survey, 1988-1994, United States. Pediatrics. 2001;108(1):40-3.
8. Olusanya BO, Okolo AA, Aderami AA. Predictors of hearing loss in school entrants in a developing country. J Postgrad Med. 2004;50(3):173-8.
9. Shargorodsky J, Curhan SG, Curhan GC, Eavey R. Change in prevalence of hearing loss in US adolescents. JAMA. 2010;304(7):772-8.
10. Araújo SA, Moura JR, Camargo LA, Alves W. Avaliação auditiva em escolares. Rev Bras Otorrinolaringol. 2002;68(2):263-6.
11. Marini ALS, Halpern R, Aerts D. Sensibilidade, especificidade e valor preditivo da queixa auditiva. Rev Saúde Pública. 2005;39(6):982-4.
12. Watkin PM, Baldwin M, Laoide S. Parental suspicion and identification of hearing impairment. Arch Dis Child. 1990;65(8):846-50.
13. Bartnik G, Stepień A, Raj-Koziak D, Fabijańska A, Niedzialek I, Skarżyński H. Troublesome tinnitus in children: epidemiology, audiological profile, and preliminary results of treatment. Int J Pediatr. 2012. Epub 2011 Jul 19.
14. Weisz N, Müller S, Schlee W, Dohrmann K, Hartmann T, Elbert T. The neural code of auditory phantom perception. J Neurosci. 2007;27(6):1479-84.
15. Harris KD. Hallucinations and nonsensory correlates of neural activity. Behav Brain Sci. 2004;27(6):796.
16. Nam EC. Is it necessary to differentiate tinnitus from auditory hallucination in schizophrenic patients? J Laryngol Otol. 2005;119(5):352-5.
17. Holgers KM. Tinnitus in 7-year-old children. Eur J Pediatr. 2003;162(4):276-8.
18. Kenitsh RC, Crocker SR, McKenna L. Children's experience of tinnitus: a preliminary survey of children presenting to a psychology department. Br J Audiol. 2000;34(6):335-40.
19. Mills RP, Albert DM, Brain CE. Tinnitus in childhood. Clin Otolaryngol Allied Sci. 1986;11(6):431-4.
20. Griest SE, Bishop PM. Tinnitus as an early indicator of permanent hearing loss. A 15 year longitudinal study of noise exposed workers. AAOHN J. 1998;46(7):325-9.
21. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM IV). 4th ed. Washington: American Psychiatric Pub; 1994.
22. Dhossche D, Ferdinand R, Van Der Ende J, Hofstra MB, Verhulst F. Diagnostic outcome of self-reported hallucinations in a community sample of adolescents. Psychol Med. 2002;32(4):619-27.
23. Kelleher I, Harley M, Lynch F, Arseneault L, Fitzpatrick C, Cannon M. Associations between childhood trauma, bullying and psychotic symptoms among a school-based adolescent sample. Br J Psychiatry. 2008;193(5):378-82.
24. Askenazy FL, Lestideau K, Meynadier A, Dor E, Myquel M, Lecrubier Y. Auditory hallucinations in pre-pubertal children. A one-year follow-up, preliminary findings. Eur Child Adolesc Psychiatry. 2007;16(6):411-5.
25. Baguley DM. Hyperacusis. J R Soc Med. 2003;96(12):582-5.
26. Jastreboff PJ, Jastreboff MM. Decreased sound tolerance. In: Snow JB, editor. Tinnitus: theory and management. Hamilton: BC Decker; 2004. p.8-15.
27. Anari M, Axelsson A, Eliasson A, Magnusson L. Hypersensitivity to sound--questionnaire data, audiometry and classification. Scand Audiol. 1999;28(4):219-30.
28. Coelho CB, Sanchez TG, Tyler RS. Hyperacusis, sound annoyance, and loudness hypersensitivity in children. Prog Brain Res. 2007;166:169-78.
29. Knobel KA, Lima MC. Knowledge, habits, preferences and protective behavior in relation to loud sound exposures among Brazilian children. Int J Audiol. 2012;51(Suppl 1):S12-9.
30. Anuário Estatístico do Estado de São Paulo. São Paulo: Fundação SEADE; 2003.
31. Béria JU, Raymann BC, Gigante LP, Figueiredo AC, Jotz G, Roithman R, et al. Hearing impairment and socioeconomic factors: a population-based survey of an urban locality in southern Brazil. Rev Panam Salud Publica. 2007;21(6):381-7.
32. Seely DR, Gloyds SS, Wright AD, Norton SJ. Hearing loss prevalence and risk factors among Sierra Leonean children. Arch Otolaryngol Head Neck Surg. 1995;121(8):853-8.
33. Holgers KM, Pettersson B. Noise exposure and subjective hearing symptoms among school children in Sweden. Noise Health. 2005;7(27):27-37.
34. Borgstein BM, Raglan E. Parental awareness and the detection of hearing loss. Pediatr Rehabil. 1998;2(4):165-72.
35. Lo PS, Tong MC, Wong EM, van Hasselt CA. Parental suspicion of hearing loss in children with otitis media with effusion. Eur J Pediatr. 2006;165(12):851-7.
36. Taha AA, Pratt SR, Farahat TM, Abdel-Rasoul GM, Albtanony MA, Elrashiedy AL, et al. Prevalence and risk factors of hearing impairment among primary-school children in Shebin El-kom District, Egypt. Am J Audiol. 2010;19(1):46-60.
37. Raj-Koziak D, Piłka A, Bartnik G, Fabijańska A, Kochanek K, Skarzyński H. The prevalence of tinnitus in 7-year-old children in the eastern of Poland. Otolaryngol Pol. 2011;65(2):106-9.
38. Hoffman HJ, Reed GW. Epidemiology of tinnitus. In: Snow JB, editor. Tinnitus Theory and Management. London: Decker; 2004. p.16-41.
39. Baguley DM, McFerran DJ. Tinnitus in childhood. Int J Pediatr Otorhinolaryngol. 1999;49(2):99-105.
40. Choong C, Hunter MD, Woodruff PW. Auditory hallucinations in those populations that do not suffer from schizophrenia. Curr Psychiatry Rep. 2007;9(3):206-12.
41. Nelson JJ, Chen K. The relationship of tinnitus, hyperacusis, and hearing loss. Ear Nose Throat J. 2004;83(7):472-6.
1. PhD; Researcher; Post-Doctoral Student - School of Medical Sciences - State University of Campinas.
2. PhD; Assistant Professor - Graduate Program in Speech and Hearing Therapy - Medical School of the State University of Campinas.
Send correspondence to:
Keila Alessandra Baraldi Knobel
Rua Tessália Vieira de Camargo, nº 126, Cidade Universitária "Zeferino Vaz"
Campinas - SP. Brazil. CEP: 13083-887
E-mail: keila.knobel@gmail.com
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on December 17, 2011.
And accepted on January 15, 2012. cod. 8938.
Fundação de Amparo à Pesquisa de São Paulo (Fapesp 2009/15825-0).
Print: ![]()