

Year: 2003 Vol. 69 Ed. 2 - (13º)
Artigo Original
Pages: 227 to 223
 PDF PT
PDF PT Speech perception optimization in deaf with multichannel cochlear implant
Author(s):
Natália B. Frederigue[1],
Maria C. Bevilacqua[2]
Keywords: deafness, cochlear implantation, speech perception
Abstract:
Aim: Accomplish an intra-subject study, evaluating the speech perception and preferences in deaf implanted with the Nucleus 24 device fitted with SPEAK, CIS and ACE strategies (Spectral Peak - SPEAK, Continuous Interleaved Sampler - CIS e Advanced Combination Encoders - ACE). Material and Methods: Seven adults with post-lingual deafness were distributed randomly in groups entitled A and B for the application of the evaluation protocol. The CIS strategy was fitted to the group A and the ACE strategy to the group B. The SPEAK strategy was the basis for all aspects. Evaluations of sentences, recognition in silence and noisy situations (cocktail party, S/N +10 dB) and adjustments of the codification strategies were carried out. Self-assessment questionnaires were applied as well. Results: The results indicated that high levels of speech recognition were observed, in silence and in noise, for all encoding strategies. The average scores obtained for the recognition of sentences in silence were 76,2%, 69,1%, and 80,2% for the SPEAK, CIS, and ACE strategies, respectively. For the recognition of sentences in noise the average scores obtained were 38,0%, 40,8% and 53,1% for the SPEAK, CIS and ACE strategies, respectively. There was no difference statistically significant between the encoding strategies. High speech recognition scores were obtained for each subject with the optimization of the strategy. Conclusion: The use of multiple speech encoding strategies as well as the choices of the various parameters allow for the clinician to fit an individual program, resulting in greater benefits for the cochlear implant users.
![]()
INTRODUCTION
The development of speech perception skills by subjects who have sensorineural hearing loss is a challenge for all professionals involved in the areas of clinical and educational audiology, since speech is present in our daily lives, taking an extremely important role in human relationships.
A number of studies focused on speech perception assessment have been developed. The studies showed concerns about improving the quality of speech perception of people with sensorineural hearing loss.
In order to minimize the consequences brought by the hearing loss, researchers have centered their efforts in improving hearing aids, collective aids (FM system), and other devices that can help the use of residual hearing and sound perception, such as cochlear implant (CI) and tactile oscillator.
Various degrees of benefits in speech perception are obtained by users of multi-channel CI. Much of the performance variability can be attributed to the coding strategies of each system for each subject1. Technology advances have allowed improvement of signal processing strategies in multi-channel CI, which allows better performance in speech comprehension. However, the most frequent complaint of users of such devices has been to recognize and understand the speech signal in noise2.
The interest in maximizing speech recognition for users of multi-channel CI represents a common characteristics for most CI centers in the world. Many issues have been discussed in the development of signal processing strategies and comparative studies, using different strategies, have been conducted. One of the most important points for the speech perception of implantable system users is the unfavorable conditions, such as the presence of reverberation and competitive noise. The speech processor codifies the acoustically processed signal for an electrode stimulation pattern. In this case, the integrity of the processor and its algorithms is a determining factor in the users' skills to separate the target signals from other signals3.
The purpose of the present study was to conduct a clinical analysis of speech perception in users of multi-channel CI Nucleus 24 using different coding strategies available in the device (SPEAK, CIS and ACE), in different hearing situations (silence and noise) in order to check the benefits resulting from the current technology for each user and to determine which strategies and which combinations of parameters can be more appropriate to patients.
MATERIAL AND METHODS
The present study was approved by the Ethics Committee of Hospital de Reabilitação de Anomalias Craniofaciais (HRAC) - University of São Paulo (USP), Campus Bauru, Opinion N. 010/2001-UEP-CEP, and was conducted at the Center for Audiological Research (CPA), HRAC/USP.
Subjects
The inclusion criteria for the studied subjects were: adult subjects, post-lingual bilateral profound sensorineural loss, users of CI multi-channel Nucleus 24 system at least for 3 months with experience with CI and open-set speech recognition. The samples comprised seven subjects (S1, S2, S3, S4, S5, S6 and S7), being five female and two male subjects, aged between 36 and 59 years. The average time of deafness was 97 months (ranging from 15 to 300 months) and the mean time of use of CI was 12 months (ranging from 4 to 19 months). Of the seven studied subjects, only one presented partial insertion of electrodes.
Procedures
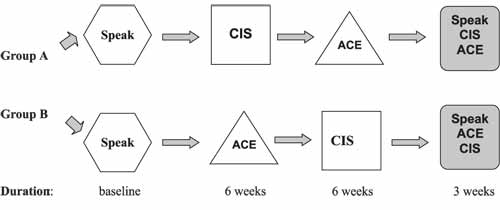
Procedures followed the protocol4 presented in Figure 1.
All subjects completed the baseline assessment using speech processor Sprint and coding strategy SPEAK so that later they could experience the other two strategies CIS and ACE. The SPEAK strategy was the basis of the study, since it was the first one used by subjects since the initial moment of CI use. This baseline assessment included a battery of open-set speech recognition tests in silence and in competitive noise (party noise - S/N ratio + 10dB). We used lists for monosyllable word recognition5, senseless syllable recognition6, CPA sentence lists7 and Self-Assessment Questionnaires.
The subjects were randomly divided into two groups, named A and B. Subjects in group A were initially adapted with strategy CIS and group B with strategy ACE. Maps with strategies CIS and ACE were created and optimized based on the necessary changes for each subject concerning stimulation speed, maximum number, channel selection, frequency gain changes, among others. After six weeks of use of such strategies, an assessment of speech perception in silence and in noise was made, followed by the application of the subjective questionnaire. The subjects were then adapted with the opposite strategy (ACE for group A and CIS for group B) and again they were assessed after six weeks of optimization and use of such strategies. These steps referred to the Initial condition of the study, being that subjects accessed the strategies separately. In the Final condition, the three coding strategies were made available in the multiple memory speech processor (Sprint) for each subject and they were accessed simultaneously. The subjects were instructed to use the strategies in various hearing situations. After three weeks of experience with the three simultaneous strategies, a comparative analysis was conducted, in a test session, using lists of sentences in silence and in noise and the subjective questionnaire. At the end of the protocol, after 15 weeks, speech processors were programmed with subjects' preferential strategies, occupying one or more processor memories.
For the statistical analysis, we used Friedman and Wilcoxon non-parametric tests. In all cases, the level of rejection of the null hypothesis was defined as below 0.05 (%).
RESULTS
All subjects in the study completed the investigation protocol. The optimal number of channels/maximum and optimal stimulation speed for strategies CIS and ACE varied from subject to subject. The occurrence for ACE strategy ranged from 500Hz, 720 Hz to 1800 Hz for the maximum and for CIS strategy, it ranged between 900 Hz, 1200 Hz, 1800 Hz and 2400 Hz by channel. The optimal set of programming parameters extended the order of available channels (6 to 12) and the stimulation speed (from 500 to 2400 Hz by channel) for the Nucleus 24 system.
Initial study conditions. High levels of speech recognition were obtained for all coding strategies tested. Table 1 shows the means and standard deviations of the CPA sentence recognition scores in silence and in noise (S/N + 10dB) for each strategy. The mean CPA sentence recognition score in silence was 61.1% for SPEAK strategy, 66.5% for CIS and 84.5% for ACE. In noise (S/N ratio + 10 dB), the mean was 38% for CIS, 49.4% for SPEAK and 60.0% for ACE. The variance analysis (Friedman test) revealed that there were no statistically significant differences among mean scores obtained in speech recognition assessments, in the three coding strategies in the initial conditions.
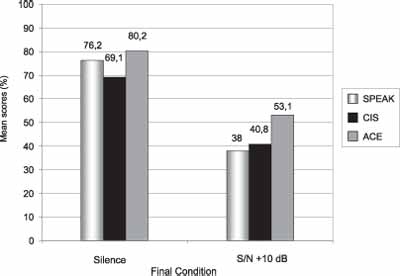
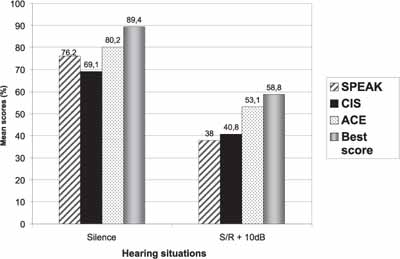
Final study conditions. In Graph 1, we can see the CPA sentence recognition scores in silence and in noise (S/N + 10dB). High levels of speech recognition have also been obtained. The men CPA sentence recognition score in silence was 69.1% with the strategy CIS. 76.2% with SPEAK and 80.2% with ACE. In noise, (S/N ratio + 10 dB), the men was 38.0% for SPEAK, 40.8% for CIS and 53.1% for ACE. The variance analysis (Friedman test) revealed that there were no statistically significant differences between mean scores obtained in speech recognition assessments among the three coding strategies. However, it was observed that in the two hearing situations (silence/noise), the strategy with the highest mean scores was ACE.
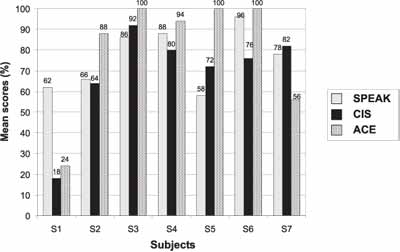
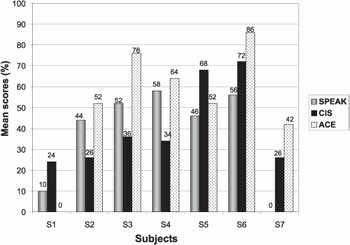
Individual differences between the strategies were noted, both for silence sentence recognition as in noise. In Graph 2, five subjects had the highest scores with ACE strategy for sentence recognition in silence, one subject with CIS and another with SPEAK. For sentence recognition in noise, the highest scores were also obtained for SPEAK. For sentence recognition in noise, the highest scores were also obtained with the ACE strategy for 5 subjects and two subjects had greater percentage of results with CIS strategy (Graph 3).
In order to estimate the collective advantage of selecting the best strategy for each subject, the group means of each strategy separately (both in silence and in noise) were compared to the best group means. To that end, the maximum individual scores obtained were calculated, regardless of the strategy, during the final condition (Graph 4). The best score group mean for sentence recognition in silence was 13.2%, 20.3% and 9.2% higher than means for SPEAK, CIS and ACE, respectively. Similarly, for sentences in noise (S/N ratio + 10dB), the best score group mean was 20.8%, 18.0% and 5.7% greater than the means for strategies SPEAK, CIS and ACE, respectively. The CPA sentence recognition best group score was 89.4% for sentence in silence and 58.8% for sentence in noise.
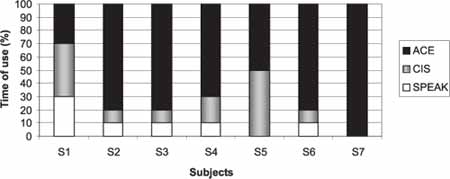
Results of the Self-Assessment Questionnaire. Graph 5 shows the results referring to time of use of each strategy in the past weeks of the protocol. Most subjects used the three strategies in the period. For three subjects, the use of strategies SPEAK and CIS occurred in 10% of the total period and CIS in 40%; one subject used strategies SPEAK, CIS and ACE in 10%, 20% and 70% of the time, respectively; one subject used strategies CIS and ACE in 50% of the time, and one subject used only the ACE strategy 100% of the time.
Find below testimonials of two subjects during the completion of the Questionnaire, showing the adaptation steps referring to changes of strategy.
Testimonial 1 (Subject 2 -group A):
From SPEAK to CIS: Based on my experience, I would not change it, since the former made everything sound more natural and understandable. I enjoyed much more the strategy I used before." From CIS to ACE: "All sounds, in generals, seem to be more authentic. Other people's voices are more pleasant and easy to understand." In the final condition: "SPEAK has now a metallic sound, CIS is muffled and ACE is very natural."
Testimonial 2 (Subject 3 - group B):
From SPEAK to ACE: "Generally speaking, ACE proved to be better than SPEAK. The adaptation was relatively easy. I managed to talk and understand people easily." From ACE to CIS: "It seems that CIS distorts high sounds, and the speech is almost incomprehensible." In the Final Condition: "SPEAK distorts the speech a lot. The speech is very unpleasant, even though it is possible to understand it. In the CIS strategy, speech seems to come out of a metallic cylinder. ACE proved to be the best strategy, in terms of quality and easy comprehension."Table 1. Man and standard deviation of speech recognition scores obtained in the initial condition of the study for the three strategies.
Figure 1. Representation of the assessment protocol. Source 4.
Graph 1. Mean speech recognition scores obtained in the Final Condition.
Graph 2. Individual scores for CPA sentences in silence among strategies SPEAK, CIS and ACE.
Graph 3. Individual scores for CPA sentences in noise (S/N ratio +10dB) among strategies SPEAK, CIS and ACE.
Graph 4. Group mean for each strategy separately compared to the maximum scores for each subject considering the strategies.
Graph 5. Results of the Self-Assessment Questionnaire referring to time of use of each strategy in the last three weeks of the protocol.
DISCUSSION
The variability found concerning the optimal set of parameters to program CIS and ACE strategies suggests that in part, this set has been the recommended algorithm of adaptation, in which such orders are initially explored before looking for other alternatives. Despite that, there is a large series of configurations available in this CI system.
The result of Table 1 demonstrates that even after wide experience with a certain speech coding strategy (in such case, SPEAK, mean use of 12 months), CI users can access additional speech characteristics through advances in strategies and development of better speech perception skills in a reasonably short period of time. Many studies have demonstrated that advanced strategies of signal processing produce immediate effects in hearing impaired people users of the multi-channel CI system, related to open-set speech perception. Some authors described that subjects developed auditory skills right after two weeks of use of the device8. Data from some studies showed that patients users of CI Nucleus 24 demonstrated immediate benefits in speech understanding when SPEAK strategy (already implemented in the system) was used, after three days of CI use9.
The data presented in Graph 1 reveal that, both in silence and in noise, the mean speech recognition scores obtained with ACE strategy were respectively 4.00% and 15.1% better than the comparison with SPEAK strategies, and 11.1% and 12.3% better when compared to CIS. Such findings can be related to the superiority of ACE strategy. Such results support the advantage to combine the spectral characteristics of SPEAK to high speed of CIS 4.
Studies have reported reduction of speech recognition skills with the introduction of competitive noise10. The comparison between Graphs 2 and 3 shows that the best performance was obtained in silence and the worst in noise (S/N ratio + 10dB). Such results emphasized the literature data.
The results of Graph 4 demonstrate that the sentence recognition mean score in silence increased from 76.2% when the subjects accessed strategies separately (in such case, the lowest score was for SPEAK) to 89.4% when the maximum score for the subject was calculated, regardless of the strategy. For sentences in noise, the mean increased from 38.0% to 58.8% and such data support the hypothesis that accessing multiple coding strategies results in better performance of CI users4.
According to the results in Graph 5, we can observe that despite the strong experience with the SPEAK strategy, ACE was more used in the final weeks of the protocol by most subjects. The total time of use of the strategy in the final conditions could have been influenced by the preference of subjects for strategy ACE and by facilities that it provided in the initial condition of the study, compared to CIS (testimonials 1 and 2). Other authors have also mentioned such preference by ACE strategy, when the final questionnaire was administered4. The testimonials of the two subjects clearly showed differences in speech signal coding strategies for each specific strategy, which were referred in details by them and corresponded directly to the concepts of different strategies for the CI Nucleus 24 system described by various authors11, 12. The difficulties in adaptation of the CIS strategy after use of SPEAK could be justified by the clear differences among them, since SPEAK promotes the stimulation of various electrodes at low speed (250 Hz by channel), with great representation of frequencies, whereas in CIS, frequency spectrum is divided into a limited number of filters and it uses four, six, eight or 12 stimulation channels at moderately high speed (500 to 2,400 Hz by channel), providing detailed temporal information4.
The data obtained in the assessment of speech perception agree with the results referred in the application of the Self-Assessment questionnaire, being that the mean scores for CPA sentence recognition both in silence and in noise (S/N ratio + 10dB) were the highest for strategy ACE (Graph 1). From a clinical perspective, it would be useful to consider the preference of strategy as a guide in adaptation, however, it is not known whether the initial adaptation would predict the performance during the whole time.
The advantages of testing multiple strategies include the skill to find a better adaptation to a given subject for both strategies and for a set of parameters (number of channels/maximum stimulation speed, among others) and maybe the skill to choose the strategy for one or more environment.
Based on the results obtained in the assessments, it is noted that the balance of choice of the coding strategy for subjects was divided into speech comprehension and sound quality provided for each strategy. Even though the CIS strategy has provided high scores of speech recognition, the subjects reported sudden chance noticed with the strategy (testimonials 1 and 2), which was based on the vocal quality provided by it, which produced worse comprehension.
Many studies have shown the importance of providing digital speech sound processing innovations to users of multi-channel CI system and the findings of this study agree with such data4, 10, 13-17.
After the completion of the protocol, two subject decided to use exclusively strategy ACE, two strategy CIS and ACE and three, SPEAK, ACE and CIS, having them available in the Sprint speech processor programming memory. It shows, once again, the great individual variability related to strategy preferences, which suggests that when isolated or combined, they are useful in one or various hearing situations. Analyzing such data, it became possible to state that the participants of the present study reached a high level of performance concerning the flexibility to use various strategies.
Cochlear implant advances have been offered to users whenever possible, so that they can be exposed to and experiment new innovations, adapting to those compatible with their needs.
CLOSING REMARKS
We have experienced CI innovations and the onset of flexible devices has allowed the use of multiple strategies in speech sound digital processing. It enables the clinician to select different algorithms allowing greater refinement and customization of the fitting process and results in higher scores when the level of speech recognition is assessed in each user.
High level of speech recognition scores were demonstrated by subjects with the three coding strategies available in model CI Nucleus 24. There were no statistically significant differences among the three strategies in all studied conditions, but the greatest scores were obtained for strategy ACE, assessed in silence and in noise. Differences in speech recognition score were noticed in each subject with the optimized strategy, using the flexible parameters according to individual needs considering the series of available options in the CI model.
CONCLUSION
The use of multiple speech coding strategies allows clinicians to customize the fitting program and results in high scores when subjects are assessed individually.
It is expected that future studies with CI progress to a level that enables all users of CI to obtain a satisfactory performance, meeting the needs of specific hearing benefits.
The clinician is then responsible for having skills, competence and critical ability to provide to the CI users the strategies and the most appropriate combination of parameters in order to improve their quality of communication.
REFERENCES
1. Fishman KE, Shannon RV, Slattery WH. Speech recognition as a function of the number of electrodes used in the SPEAK cochlear implant speech processor. J Speech Lang Hear Res 1997;40:1201-15.
2. Zhao F, Stephens SD, Sim SW, Meredith R. The use of qualitative questionnaires in patients having and being considered for cochlear implants. Clin Otolaryngol 1997;22:254-9.
3. Margo V, Schweitzer C, Gail F. Comparisons of Spectra 22 performance with and without an additional noise reduction processor. Sem Hear 1997;18:405-15.
4. Arndt P, Sttaler S, Arcaroli J, Hines A, Ebinger K. Within-subject comparison of advanced coding strategies in the Nucleus 24 cochlear implant. [s.l.]: Cochlear Corporation, 1-7; 1999.
5. Lacerda AP. Logoaudiometria. In: Lacerda AP. Audiologia clínica. Rio de Janeiro: Guanabara Koogan; 1976.
6. "Consonat Confusion Study - Confusion program" apresentado no software de sistema de implante coclear Nucleus, na sua unidade de programação - versão 6.90.
7. Valente SLOL. Elaboração de listas de sentenças. [Dissertação]. São Paulo: Pontifícia Universidade Católica de São Paulo; 1998.
8. Staller A, Menapace C, Domico E, Mills D, Dowell RC, Geers A, Pijl S, Hasenstabe S, Justus M, Brunelli T, Adam A, Borton T, Lemay M. Speech perception abilities of adult and pediatric Nucleus implant recipients using the Spectral Peak (SPEAK) coding strategy. Otolaryngol Head Neck Surg 1997;117:236-42.
9. Bevilacqua MC, Costa Filho AO, Nascimento LT, Frederigue NB, Silveira. Relato de casos: pacientes adultos com implante coclear Nucleus 24. Audiologia Atual. Collectanea Symposium, Medicina e Saúde 1998;1:121-6.
10. Kiefer J, Muller J, Pfenningdorff T, Schon F, Helms J, von Ilberg C, Baumgartner WD, Gstoettner W, Ehrenberger K, Arnold W, Stephan K, Thumfart W, Baur S. Speech understanding in quiet and in noise with the CIS speech coding strategy (MED EL Combi-40) compared to the MPEAK and SPEAK strategies (Nucleus). Adv Otorhinolaryngol 1997;52:286-90.
11. Loizou PC. Signal-procesing techniques for cochlear implants. IEEE Eng Med Biol Mag 1999;18:34-46.
12. Waltzman SB, Cohen NL, Roland Junior T. A comparison of the growth of open-set speech perception between the nucleus 22 and nucleus 24 cochlear implant systems. Am J Otol 1999;20:435-41.
13. Bevilacqua MC, Costa Filho AO, Moret ALM, Barreira CSC, Nascimento LT, Silveira TS et al. Implante coclear em criança: novas estratégias de codificação. In: Anais do 4º Congresso Internacional de Fonoaudiologia, 4º Encontro Ibero-Americano de Fonoaudiologia; 1999, São Paulo: Sociedade Brasileira de Fonoaudiologia; 1999. p. 383.
14. Cohen NL, Waltzman SB, Roland Jr JT, Bromberg B, Cambron N.. Results of speech processor upgrade in a population of Veterans Affairs cochlear implant recipients. Am J Otol 1997;18:462-5.
15. Holden LK, Skinner MW, Holden TA. Speech recognition with the MPEAK and SPEAK speech-coding strategies of the Nucleus Cochlear implant. Otolaryngol Head Neck Surg 1997;116:163-7.
16. Parkinson AJ, Parkinson WS, Tyler RS, Lowder MW, Gantz BJ. Speech perception performance in experienced cochlear-implant patients receiving the SPEAK processing strategy in the Nucleus Spectra-22 cochlear implant. J Speech Lang Hear Res 1998;41:1037-87.
17. Skinner MW, Clark GM, Whitford LA, Seligman PM, Staller SJ, Shipp DB, Shallop JK, Everingham C, Menapace CM, Arndt PL. Evaluation of a new spectral peak coding strategy for the Nucleus 22 Channel Cochlear Implant System. Am J Otol [Suppl] 1994;15:15-27.
1 Master in Education, Pontifical Catholic University of São Paulo, Doctorate studies in Psychology under course, Program of Neuroscience and Behavior,
University of São Paulo/SP, Speech and Hearing Therapist, Centro de Atendimento aos Distúrbios da Audição, Linguagem e
Visão (Cedalvi), Hospital de Reabilitação das Anomalias Craniofaciais (HRAC), University of São Paulo.
2 Full Professor, Head of the Department of Speech Therapy and Audiology, Dental School, University of São Paulo, Speech Therapist and Audiologist, HRAC-USP, responsible for the Program of Cochlear Implant, Centro de Pesquisas Audiológicas (CPA), HRAC-USP.
Center for Audiological Research, Hospital de Reabilitação de Anomalias Craniofaciais, University of São Paulo - Financially supported by CAPES.
Address correspondence to: Hospital de Reabilitação de Anomalias Craniofaciais - Centro de Pesquisas Audiológicas (CPA) -
Rua Silvio Marchione 3-20 São Paulo SP 17.043-900
Tel (55 14)235-8433 - Fax (55 14)234-2280 - E-mail: natifrederigue@yahoo.com
Presented as Post-Graduation Oral Communication, XVI Encontro Internacional de Audiologia, Rio de Janeiro/RJ,
Article submitted on January 31, 2003. Article accepted on March 20, 2003.
Print: ![]()