

Year: 2002 Vol. 68 Ed. 6 - (23º)
Relato de Casos
Pages: 920 to 925
Internal carotid artery in the middle ear: diferent forms of clinical presentation
Author(s):
Ricardo Gimenes Ferri 1,
Jurandy Marcelo da Silva Pessuto 2,
Ektor Tsuneo Onishi 3,
José Ricardo Gurgel Testa 4,
Norma de Oliveira Penido 5,
Yotaka Fukuda 6
Keywords: internal carotid artery, middle ear, tinnitus
Abstract:
Alterations on the normal internal carotid artery's (ICA) path on the petrous portion of the temporal bone are extremely rare. Normally the artery ascends vertically, medial and prior to the timpanic cavity and right bellow the hearing tube, prior and medially to the cochlea. In its path, the ICA can present from few anatomic variatious (micro-dehiscence, dehiscence, and so on) to great alterations in positioning and localization, but with similar clinical expression. The bone dehiscence of the ICA canal occurs in 1% of the cases, and the congenital bone deffect associated with the ICA anormality has an even smaller incidence. The deffective carotid artery is a vascular malformation of the middle ear which the main differential diagnostics are the aneurism of the internal carotid artery, the high julgular bulb and the timpanic or julgular glomus. The most found clinical patology is the conductive hearing loss associated with pulsatile tinnitus sincronyzed with heart bit and the presence of a retrotimpanic blue orpink mass located at hypotympani. The initial chosen radiologic exam is the computerized tomography of the temporal bones that can accuse an enlarged lower timpanic canal and an intra-timpanic mass in continuity with the ICA, associated with a dehiscence of the lateral bone wall of this artery. The arteriography or the magnetic resonance angiography are used on die cases of diagnostical uncertainties. The treatment is still controvertial. Here in describe a serie three cases, including the clinical findings, diagnostical investigation, and conduct as well as a review of the literature.
![]()
INTRODUCTION
Pulsatile tinnitus is a not very frequent in otological patients but many times it requires surgical intervention. Myoclonal symptoms caused by muscle contractions (stapedial, tympani tensor muscle, palatini veli muscle, etc.) and vascular abnormalities are the most common causes.
If it is synchronous with the heart beat, it means that the noise of the blood flow is being transmitted to the auditory organ, which can be present in patients with carotid artery aneurysm in the intra-temporal segment, hemagioma, tympanic or jugular paraganglioma 3 (glomus) and aberrant carotid artery4.
The detailed investigation of the symptom should be made by careful clinical history, general physical and otorhinolaryngological examination, auditory assessment and radiological study using computed tomography, for the correct diagnosis and appropriate therapeutic planning.
The authors present cases of abnormalities of the carotid artery tract that lead to otorhinolaryngological complaints and a literature review about the topic.
REVIEW OF LITERATURE
The course of aberrant internal carotid artery (ICA) in the middle ear was reported for the first time in 1899 by Max, who identified an artery pulsating in the tympanic cavity through a tympanic perforation5, 6. Hansen (1903) accidentally identified the ICA in the tympanic cavity in his collection of temporal bones6. Since Lapayowker et al. (1971), many authors have reported it, such as Poncet and Miller (1979), Cohen and Briant(1981), Damsma et al. (1984), Glasscock et al. (1980), Sinnreich et al. among others. Up to 1993, only 45 cases had been reported in the literature, most of them female patients aged on average 25 years, whose right side was the most affected one7. Many descriptions were made through intra-operative diagnoses, such as by Goodman (1981) who accidentally conducted a tympanotomy in a case of aberrant ICA intending to treat a secretory otitis media4.
The main theories about the etiology of aberrant ICA were based on Steffen, 1968, who described in details the embryology of the middle ear arterial system and defended that the stapedial-hyoid artery could fixate the ICA in a defective developmental position, modifying its normal path. Lasjaunias and Moret (1978) and later Poncet and Miller (1979) defended another theory in which the failure in developing the distal portion of ICA and its function would be suppressed by hypertrophy of anastomosis between the inferior tympanic and the caroticotympanic arteries, being the anastomosis the vessel we see in the tympanic cavity.
The main differential diagnoses are secretory otitis media, paraganglioma, intra-temporal carotid artery aneurysm, hemangioma 7, 9 and other middle ear vascular malformations.
CASE REPORT
CASE 1
M.F.L.A., 34 years old, female, Caucasian, married patient, cleaning woman and born and living in São Paulo. She came to the center complaining of noise in her ear for 3 years. According to the patient, she had had left ear progressive tinnitus, sometimes pulsatile, which worsened when she moved her head, but not constant. She did not refer otalgia, otorrhea, hearing loss, vertigo and other previous affections.
At the otorhinolaryngological examination, on the left otoscopy, we detected a slightly purple retro-tympanic mass, located on the anterior quadrant of the tympanic membrane, around the anterior process of malleus, over the promontorium. Right otoscopy and the remaining tests were normal. Pure tone audiometry showed conductive hearing loss with thresholds at 35dB in various frequencies, with bone-air gap of 10dB HL, and speech discrimination of 92%. Hearing thresholds on the right were normal, and there was only an isolated loss at 6kHz. Audiometry Weber test lateralized the response to the left (Figure 1). Tympanometry detected curve A (Jerger) in both ears, and it was not possible to detect stapedial reflex owing to pulsation of the impedanciometer needle (Figure 2). Computed tomography evidenced a vascular mass in the left tympanic cavity (Figure 3), leading us to the hypothesis of tympanic glomus. The patient was submitted to exploration tympanomastoidectomy by retro-auricular access with enlargement of external acoustic canal to improve the visualization of the tympanic cavity. The tumor process was in contact with the anterior process of malleus and the long ramus of the incus and they were purplish gray, pulsatile, recovered by thickened mucosa (Figure 4). We removed the malleus and incus and carefully dissected the tumor which was a well-delimited cylinder shape, both anterior-posterior and laterally, with no superior-inferior delimitation. We dissected as much as possible in the superior direction, towards the middle fossa, but it was not possible to identify the delimitation, similarly to the inferior portion. The cylinder mass was about 5mm in diameter, pulsatile and presented very thick and resistant walls that are normally found in tympanic glomus. Since we suspected it could be a vessel, we conducted a punch with a 30x7cm needle, and we obtained a spray 20mm away from the needle, confirming that it was a thick caliber vessel. We performed hemostasis with packing of the tympanic cavity with muscle fragments and replaced tympanomeatal flap. Postoperative CT scan control showed that there was a continuation of the tympanic cavity and the internal carotid artery, both inferiorly and superiorly, plus absence of the anterior-lateral bone wall of the carotid canal. We conducted an arteriography that confirmed the presence of the carotid in the tympanic cavity (Figure 5). The patient progressed well, with significant improvement of tinnitus and worsening of conductive hearing loss (Figure 6).
CASE 2
E.B.S., 31 years old, female Caucasian single patient, housewife, born and living in São Paulo. She reported history of progressive worsening of rotation dizziness throughout the past 8 years associated with pulsatile tinnitus on the left ear, which worsened with neck extension or flexion. She did not report hearing loss, ear pain or otorrhea. Upon the examination, we observed purple retro-tympanic tumor in the anterior and middle portions of the inferior hemitympanum of the left ear. Audiometry presented thresholds within the normal limits on the right and mild sensorineural loss (30dB HL) at 8kHz on the left, with 100% speech discrimination and normal vectoelectronystagmography. Temporal bone CT scan revealed internal carotid off the normal limits and dehiscent in the left middle ear. We conducted an angioresonance that confirmed the hypothesis of aberrant carotid. The patient was properly instructed and she has been followed up for 2 years now (Figure 7).
CASE 3
G.M., 40 years old, male Caucasian single patient, office clerk, born and living in São Paulo. He reported history of pulsatile tinnitus on the right for a long time, with no previous hearing loss; he came to the emergency room two year ago because of a sudden episode of right ear fullness, followed by sporadic whistling tinnitus, continuous pulsatile tinnitus especially in silent rooms and with mild rotations dizziness. He underwent ENT examination, interpreted as normal, and pure tone audiometry and serial speech discrimination, showing that he had profound sensorineural loss on the right and normal hearing on the left. Investigation for perilymphatic fistula (Tulio and Hennebert phenomena) were negative. We made the diagnostic hypothesis of sudden deafness and started clinical treatment with oral pentoxyphillin and cinarizine, resulting in stabilization of the vestibular disorder (improvement of rotation dizziness) and improvement of the whistling tinnitus, but he still presented pulsatile tinnitus and profound sensorineural loss on the right. After one year of follow-up, he was submitted to a new audiometry that showed profound sensorineural loss on the right and mild sensorineural loss on the left, with an inverted U pattern. At the same time, we noticed a slight asymmetry of the tympanic membrane at otoscopy, with pink-reddish retro-tympanic tumor on the right hypotympanum. Normal metabolic tests. By means of temporal bone CT scan we detected hypotympanum tumor that advanced into the right middle ear, continuing to the carotid canal (horizontal portion) through dehiscence of the canal lateral wall (Figures 8 and 9). Therefore, we diagnosed aberrant carotid artery and the patient has been followed up in our center.
Figure 1. Audiogram.
Figure 2. Immittanciometry.
Figure 3. Temporal bone CT scan of Case 1, showing temporal bone (arrow).
Figure 4. Intra-operative aspect of tympanic cavity in Case 1.
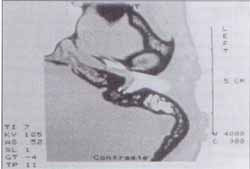
Figure 5. Arteriography of Case 1.
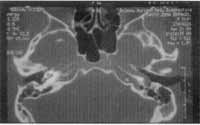
Figure 6. Temporal bone computed tomography of Case 2.
Figure 7. Audiogram of Case 3.
DISCUSSION
The abnormality detected in those cases is a rare condition, and there are few cases described in the literature4, 5, most of them are mistaken by glomus tumor. The carotid artery presentation in the tympanic cavity is the result of an anatomical abnormality in its path, leading to lateralization. Normally, the carotid artery penetrates into the carotid canal through the carotid foramen located in the skull base, more specifically in the inferior face of the temporal bone petrous portion, descending vertically. At the cochlear level, it takes a curve and goes towards the anterior-medial and horizontal direction, towards the lacerum foramen, on the floor of the cranial middle fossa. In the vertical portion, the carotid canal is located inferiorly to the cochlea, anterior to the jugular fossa and medially to the tympanic cavity. The horizontal portion of the carotid canal is presented posterior-medially to the auditory tube7, 10. In the curve, it is located between the auditory tube and the basal cochlear gyrus. At this position, the layer that separates the carotid from the tympanic cavity is a thin bone layer7. In some situations, this layer may be absent or present at different dehiscence degrees. According to Goldman4, there may be other abnormalities in the carotid system concomitant to the presence of the carotid artery in the tympanic cavity, which are normally related to congenital malformations. The etiology of aberrant ICA is controversial, and currently there are two theories based on the embryonic development of the dorsal portion of the carotid artery11. The pulsatile tinnitus synchronous with heartbeat is the main clinical symptom found in cases of aberrant carotid artery. In most of the cases, the patient comes to the otorhinolaryngologist with different complaints and diagnostic suspicion comes from the otoscopy, where we can seen on the anterior-inferior portion of the tympanic membrane a red or purple spot, normally on a normal and transparent posterior quadrant. Some patients also present hearing loss. Based on clinical suspicion, we should order complementary tests. Audiometry and immittanciometry can be normal or present conductive hearing loss associated with pulsating needle, synchronous to heart beat. Imaging exams are essential.
High resolution computed tomography scan (CT) of the temporal bones reveals the path of the ICA in the middle ear by well-defined axial sections of the carotid artery and their possible dehiscence. Corazza 12 in an analysis of the temporal bone using CT, found ICA dehiscence in the middle ear in 0.5% of the cases. Conversely, when the analysis is made in histology sections (Lion13), the percentage of micro-dehiscence increases to 38%. Differently from the cases of aberrant pathway, dehiscence and micro-dehiscence are less important from a surgical perspective, except in cases of hypotympanum approach and trans-cochlear access. They can clinically translate into pulsating tinnitus of vascular origin, whose investigation through imaging methods is not conclusive in most cases, owing to the sensitivity of the method. Thus, patients who have this type of anatomical variation can present tinnitus of vascular origin with normal CT scan.
Magnetic resonance has been of great importance in the differential diagnosis and angioresonance practically demonstrates the whole path of the carotid in the middle ear with details2, 9. Arteriography is a very useful test and it also helps the diagnosis of aberrant carotid artery, but it is more invasive, preferred to be used in cases of diagnostic doubts. Therefore, we can conclude that the diagnosis should be made based on accurate clinical study, including detailed clinical history in order to characterize the type of tinnitus and complete otoscopy. Other causes of pulsating tinnitus are: arterial-venous shunt, arterial-venous anastomosis, jugular bulb abnormalities, high intra-cranial pressure, jugular or tympanic glomus, meningiomas 8, carotid aneurysm and lateralization of the intra-temporal carotid artery.
The treatment of aberrant carotid artery is controversial. Some authors advocate surgery as the preferred treatment, using the projection of the abnormal path of the vessel with fascia or thin layers of silastic in order to try to prevent erosion of the vessel by the ossicle chain or the adjacent bone. Other authors contraindicate surgical treatment when there is suspicion or diagnosis of aberrant carotid artery. In Case 1, the initial diagnosis was glomus tumor and during the surgical act we identified it as an anatomical abnormality of the internal carotid artery. This case illustrates very well the need for a high index of suspicion of malformation of ICA in the petrous portion and the difficulty to differentiate it from tympanic glomus without specific radiological imaging (angiography or angioresonance). Other diagnoses can be made only intra-operatively, such as serous otitis referred to myringotomy, as described by Goodmann4.
During the procedure, if there is bleeding, it is recommended to use immediate packing of the external acoustic canal and use of nasopharyngeal tubes to block the auditory tube. In some cases, it is necessary to perform embolization or ICA ligature, despite the risks of sequels. Case 2 has a very typical presentation and intervention, with diagnosis and therapeutic instructions that resulted in no surprises. Case 3, however, had a very uncommon presentation. The history of acute sensorineural hearing loss is not part of the common picture. Pulsating tinnitus is the most frequent symptom in cases of aberrant carotid and dizziness, which can be less frequent, but sudden deafness has never been described. A literature review performed in studies since 1962 found no references. It is difficult to state that the etiology of the sudden deafness had been the presence of aberrant carotid; despite the normal results of other tests, we know that idiopathic cases in this condition are very common.
Despite being rare, the existence of carotid artery in the middle ear (aberrant) should be suspected whenever we have patients with pulsating tinnitus and the presence of retro-tympanic tumor. Careful history and physical examination can guide us to order complementary tests. Audiometry sometimes does not clarify the questions but immittanciometry can reveal synchronous beating of the needle with patients pulse and that is highly suggestive. The imaging tests, such as CT scan, magnetic resonance, angioresonance and arteriography can confirm the diagnosis.
The report of three cases showed us that diagnostic suspicion and comprehensive examination of the patient and the analysis of complementary tests is essential for the correct diagnosis and appropriate intervention, preventing surgical catastrophes.
REFERENCES
1. Saada A et al. Imagin Quis Case. Arch Otolaryngol Head Neck Surg 1996:122.
2. Caldas JGMP, Iffenecker C et al. Anomalous vessel in the middle ear: the role of CT and MR angiography. Neuroradiology 1998;40:748-751.
3. Fukuda Y, Penido NO, Munhoz MSL, Mota PHM, Oliveira HC. Internal Carotid Artery in the Middle Ear: differential diagnosis with glomus. Rev Laryngol 1991;112:75-8.
4. Goodman RS & Cohen NL. Aberrant Internal Carotid Artery in the Middle Ear. Ann Otol 1981:90.
5. Britton B.H. et al. Bruit Caused by Aberrant Carotid Artery in the Middle Ear. Surg Neurol 1988;30:71-2.
6. Jacobsson M et al. Aberrant intratympanic internal carotid artery: a potentially hazardous anomaly. The Journal of Laryngology and Otology 1989;103:1202-1205.
7. Glasscock M et al. Bilateral Aberrant Internal Carotid Artery: Case Presentation. Arch Otolaryngol Head Neck Surg 1993;119:335-339.
8. Cole RD. Aberrant Internal Carotid Artery. Southern Medical Journal 1994;87(12):1277-1280.
9. Bold et al. Magnetic Resonance Angiography of Vascular Anomalies of the Middle Ear. Laryngoscope 1994;104:1404-1411.
10. Swartz JD. Aberrant internal carotid artery lying within the middle ear. Neuroradiology 1985;27:322-326.
11. Cruz OLM e Costa SS. Otologia clínica e cirúrgica. 1ª edição, São Paulo: Revinter, 2000. p. 92-3.
12. Corazza RA. Variação no trajeto da Artéria Carótida Interna e Veia Jugular Interna no osso temporal avaliada pela Tomografia Computadorizada de Alta Resolução. Tese [Mestrado], 2000. Universidade Federal de São Paulo, Escola Paulista de Medicina, São Paulo.
13. Lion CSN. Deiscência do Canal Carótico na orelha média com exposição da Artéria Carótida Interna. Tese [Mestrado], 2000. Universidade Federal de São Paulo, Escola Paulista de Medicina, São Paulo.
14. Potter GD, Graham MD. The Carotid Canal. Radiologic Clinics of North America 1974;13(3):483-9.
1 Master studies under course, UNIFESP-EPM.
2 Otorhinolaryngologist, UNIFESP-EPM.
3 Doctorate studies under course, UNIFESP-EPM.
4 Ph.D. in Medicine, UNIFESP-EPM.
5 Ph.D. in Medicine UNIFESP-EPM.
6 Full Professor, Head of the Discipline of Otorhinolaryngology UNIFESP-EPM.
Study conducted at the Discipline of Otorhinolaryngology, Federal University of São Paulo -
Escola Paulista de Medicina
Address correspondence to: Rua Botucatu, 740 3º andar sala 23 Vila Clementino
São Paulo SP 04023-900
Article submitted on August 09, 2001. Article accepted on January 24, 2002.


Print: ![]()