

Year: 2002 Vol. 68 Ed. 6 - (13º)
Artigos Originais
Pages: 861 to 868
Correlation between craniofacial morphology and mliddle ear diseases in adults
Author(s):
Renata Cantisani Lei Francesco 1,
Perboyre Lacerda Sampaio 2,
Ricardo Ferreira Bento 3
Keywords: dysphonia, vocal fold, vocal nodule
Abstract:
There are thousand types of faces. The face proportions, in children, are distinct of adult ones. Diseases of middle ear are more frequent in children. The type of cranial base and the displacement of the maxilla during craniofacial growth influence the growth of the auditory tube. So, there should be a correlation between craniofacial morphology and otitis media. Aim: The aim of this study are to correlate facial types and cephalometric measurement morphology to otitis media and suggest which measurements can be used as a prediction of the evolution of otitis media. Study design: Clinical prospective. Material and Methods: We studied 64 patients, 18 to 40 years old, from Department of Otolaryngology of the University of São Paulo Medical School. They were divided into two groups: 32 with otitis media and 34 controls. We excluded patients with personal or familiar history of cleft palate, previous bucal, maxillar, pharyngeal, facial or nasal surgery, orthodontic treatment or obstructive process of the auditory tube ostia. All subjects underwent to complete ENT physical examination, videotoscopy, fibernasalendoscopy and lateral cephalograms. Results: Statistical analysis of the cephalometric measurements showed significant differences of cranial base; projection of maxilla and facial height, in patients with otitis media when compared to the control group or to the ideal measures of the harmonic face. There was no predominance of any facial type. Conclusion: The following measures were found to be predictive of the evolution of otitis media: N-S (anterior cranial base), N-S.Ba (angle between anterior and medial cranial base), PMax (projection of the maxilla) and N-ANS (superior anterior facial height).
![]()
Introduction
Every day, we come across the face of thousands of people and recognize each of them because of different characteristics. There are oval, triangular and round faces. Each type is unique, a consequence of the combination between different mandibles, orbits, mouths, maxillas, etc.1
Hippocrates, in his 6th book about epidemics, wrote that: Among the subjects whose heads are elongated, some have wide necks and strong limbs, others have high palate, irregularly aligned teeth, one on top of the other, and they are frequently affected by headaches and otorrhea. 2
Politzer, since 1862, had already suggested that poor functioning of the auditory tube could be the most important factor in the genesis of middle ear infectious diseases3.
It is known that otitis media episodes are more frequent in childhood4 and its incidence reduces as the person matures. Auditory tube dysfunction is more common in this age range owing to its more horizontal position in relation to the skull base. It is during cranial growth and development processes that the auditory tube gets its more vertical position, characteristic of the adults4, 5, 6.
In 1925, Pautow7 suggested that there could be a correlation between format of the head and auditory tube anatomy. Subjects with facial malformations such as cleft palate, Pierre-Robin, Crouzon and Down syndrome have higher incidences of middle ear infections caused by morphological abnormalities in the cranial-basal region and the dysmorphic relation of the auditory tube8.
Cephalometry is a technique that enables dental-cranial-facial assessment through head frontal and lateral x-rays taken in a constant pattern, through linear and angular values. Widely used in orthodontics, it has extrapolated the limits of the specialty, and became a complementary technique for the diagnosis of skeletal facial architecture. The cephalometric analysis enables visualization of the various positions of the maxillary and mandibular complex in addition to the relations of the other adjacent structures9.
It is very common in our clinical practice to observe patients that present otitis media in the adult age, be it by middle ear effusion or suppurative otitis media. In many occasions, these patients are submitted to unsuccessful tympanoplasty even when they were treated for factors that normally lead to tube dysfunction, such as nasal obstruction, allergy and obstruction of the auditory tube pharyngeal ostium, at the level of the nasopharynx, whereas others were not.
If the development of the auditory tube is related to craniofacial growth, it is probable that its anatomy and physiology are strictly correlated with the facial and cranial structures of adult subjects. By knowing this correlation it would be easier to understand the reasons for failure in some cases of clinical and surgical treatment of middle ear infectious disease, whose good result would have been related to normal tube functioning. Thus, the objectives of this study were:
1. To study the correlation between middle ear diseases influenced by auditory tube dysfunction and morphology (cephalometric measurements) and craniofacial typology.
2. To determine which cephalometric values are the most important ones and to suggest cephalometric tracings with predictive value for middle ear diseases influenced by auditory tube dysfunction.
material and method
The studied group consisted of 32 volunteer patients aged 18 to 40 years, seen at the Division of Clinical Otorhinolaryngology, Hospital das Clinicas, University of São Paulo (20 men and 12 women). The subjects presented middle ear diseases or sequels, such as: serous otitis media (SOM), simple chronic otitis media (Simple COM), or suppurative chronic otitis media (suppurative COM). We considered as sequels retraction and thickness of tympanic membrane and tympanosclerosis plaques. All subjects presented bilateral affection.
Thirteen patients presented previous or current history of nasal obstruction or nasal abnormalities as physical finding, such as controlled rhinitis - 6, septal deviation - 4, turbinate hypertrophy - 3.
The subjects that were excluded had: personal or family history of cleft palate; oral, maxillary, pharyngeal, nasal or facial previous surgeries; obstructive processes of the pharyngeal ostia of the auditory tube at nasofibropharyngoscopy; cholesteatomatous chronic otitis media, or those who had been submitted to orthodontic treatment.
The control group consisted of 34 volunteer patients (16 men and 18 women) seen at the Division of Clinical Otorhinolaryngology, Hospital das Clinicas, University of São Paulo, who did not present middle ear diseases nor met the exclusion criteria. Among the 13 who reported nasal obstruction, the causes were allergic rhinitis - 7; septal deviation - 4, turbinate hypertrophy - 3. All subjects underwent anamnesis and complete ENT examination. Patients were submitted to ear telescopy with the device Hopkins Optics 4mm, otological use, and fibronasopharyngoscopy with flexible endoscope Machida ENT of 3.2 mm, and halogen 250 Watts light source. The exam was conducted under mild topical anesthesia of the nasal fossa with stovaine or tetracaine 4% with 0.5% solution of phenylephrine. The device was introduced through one of the fossa, along the inferior turbinate or middle meatus, up to visualization of the nasopharynx, paying special attention to the auditory tube ostia, which should be unobstructed.
Both the middle ear telescopy and nasofibropharyngoscopy were videotaped.
Cephalometry
Subjects were submitted to teleradiography at profile. Radiographs were conducted in a x-ray device, brand Dentoramix, with variations from 30 to 100mA and 0 to 120 kV; regulated to 100mA, 90 kV and exposure time of 0.30 seconds (30 mA).
In order to standardize the radiographic exam in profile we used a cephalostat adapted at a fixed distance between the focal area of the x-ray device and the median sagittal plan (for normal lateral one) approaching it as much as possible from the head of the patient, enabling greater contact with the film, pressing the meeting point between the left tip of the cephalostat in order to have an enlargement of the image below 4% in relation to the median sagittal plan. The patient was positioned at the cephalostat so as to have the median sagittal plan perpendicular to the central x-ray of the device and the Frankfurt plan parallel to the floor.
The exams were processed in radiographic film Kodak®, 24x30 cm, by automatic method.
Cephalometric Analysis
The cephalometric tracing was conducted using ultraphan paper and pencil HB 0.5mm, by drawing the contour of the head and the anatomical structures.
We identified cephalometric reference points from the x-rays. These points served as a guide for the determination of the lines and plans.
We decided to use the cephalometric analysis manually, despite the various commercially available software packets. This kind of software analysis has standardized measures of each specific analysis, and that hinders the association of measures made by different authors, which was done by the present study.
For cephalometric analysis, we used linear and angular measures (Figure 1).
Determination of facial type11
Facial type is determined by means of EF, PF, PM, AFAI and AM values. By defining the VERT index (arithmetic mean of the difference between the above mentioned measures, obtained from the cephalometric analysis, and the values considered ideal for a harmonic face, divided by the standard deviation). The value obtained was compared to the table, defining, thus, the facial axis.
The methodology of the present study was approved by the Research Ethics Committee of Hospital das Clinicas, Medical School, University of São Paulo. All patients participated voluntarily. They were informed about the procedures and signed the Informed Consent Term.
Statistical Analysis
The comparison between the groups was conducted based on parametric and non-parametric tests considering the data and variability of measures made.
We used the following statistical methods12:
To compare the group of subjects with middle ear disease and the controls and the value considered ideal for a harmonic face: t Student test;
To associate two variables: Chi-square test (by Pearson);
The statistical analysis considered level of significance as p< 0.05.
Figure 1. Cephalometric tracing.
Linear measurements for lateral analysis (Figure 1):
1.N-S: length of the skull base anterior fossa
2.S-Ba: length of the skull base medial fossa
3.Go-Me: length if the mandibular body
4.N-Me anterior facial height
5. Frankfurt Plan: the line that passes through points Po and Or (reference plan)
6.ENA-ENP: length of bone palate
Angular Measurements:
7.S-N.Go-Me: angle between the anterior skull base and the mandible
8. ENA-ENP.Po-Or: relation of the palatine plan and Frankfurt plan
9. Mandibular Plan PM (Go-Me.Po-Or): Measured by the angle formed by the mandibular plan Go-Me and the Frankfurt plan.
10. Facial Axis EF (Angle formed by line Ba-N, with line Pt-Gn): it informs the direction of growth of the mentalis and expresses facial height proportion).
11. Inferior Anterior Facial Height - AFAI: ENA-Xi.Pm: Angle formed by the nasal spine up to point Xi, and from this point to Pm point.
12. Mandibular Arch (AM): Angle formed by the mandibular body axis (Xi-Pm, by its prolongation and the condyle axis Xi-Dc.
13. Facial Depth PF: Angle formed by Frankfurt plan (Po-Or) and facial plan (Na-Pog). Locates the mentalis horizontally on the face.
14. Facial Cone (Go-Me.Gn-N): facial convexity.
15.N-S.Ba: angle between the anterior and middle cranial basis.
16. Maxillary depth PMax: angle between Frankfurt plan and N-A.
17.Po-Or. Ba-N: cranial deflection
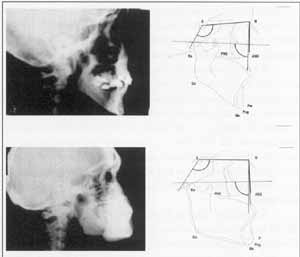
Figure 2. Comparison of cephalometric tracings.
A- subject with middle ear disease
B- subject without middle ear disease
Figure 3. Growth of maxilla and redirecting of auditory tube.
Figure 4. Cephalometric tracing proposed for predictive assessment of the evolution of the disease.
Results
We studied 66 patients, mean age of 18-40 years. Among them, 32 presented middle ear disease and were aged 26.69 years (SD of 7.94years) and 34 did not present it (control group) and were aged 27.74 years (SD of 5.81 years). As to gender, there were 36 male and 30 female patients, distributed in both groups, with no statistically significant difference. There was predominance of Caucasian subjects. Among the patients with middle ear affection, there were 24 Caucasian, 2 mixed races and 6 black people, and among those without the affection, there were 28, 2 and 4, respectively.
A. PRESENCE OF NASAL OBSTRUCTION
By analyzing the incidence of obstruction in the studied groups, we observed a value of chi-square = 0.04 and a value of P = 0.084, showing that nasal obstruction has no influence on the samples (Table 2).
B. RESULTS OF CEPHALOMETRIC STUDIES
Cephalometric measurements were compared between the two groups and some were measured and compared between the group with middle ear disease and the normal values described in the literature. The results can be seen in Table 3.
C. FACIAL TYPE
There was no correlation between facial type and middle ear disease (Table 4).Table 1. Comparison of values for facial type.
Note: Chi-square: 0.04
Value P: 0.84
Table 2. Frequency of nasal obstruction.
Note: Chi-square: 0.04
Value P: 0.84
Table 3. Comparison of Cephalometric Measurements.
NOTE: C/S: tests comparing the group with middle ear disease and the group without it.
C/N: test comparing the group with disease and the normal range by the literature.
* normal range values according to JARABAK (1965)15
** normal range values according to RICKETTS (1982)25
TABLE 4. Association between facial type and middle ear infectious diseases.
OTE: Chi-square = 9.40
Degree of freedom = 5
p value = 0.094
Discussion
ENT physical examination starts from the face and there lies most of the structures that we treat in our specialty. The knowledge of craniofacial type and characteristics of each one, as well as development and growth, favors the understanding of many abnormalities or variations in the region, contributing to better understand the occurrence and pathophysiology of the diseases.
We decided to restrict the sample from 18 to 40 years of age since craniofacial growth is stabilized at the age of 17 or 18 years in both genders1. There are no significant differences among the genders13, 14.
We studied patients with secretory and chronic otitis media except for cholesteatomatous, which may not be associated to auditory tube dysfunction15.
Nasal Obstruction
The analysis of the incidence of nasal obstruction in the study group showed that there is no association between nasal obstruction and middle ear disease in our sample. It is known that mouth breathing brings abnormalities to facial conformation. However, the main consequences are seen in the inferior third of the face, such as retrognatia, cross or open bite, obtuse gonic angle16, and as we are going to show next, they are different from those identified in the present study. It is suggested, thus, that nasal obstruction is part of etiopathogenic factors of tube dysfunction. They participate in the nasal process of the auditory tube pharyngeal ostium, such as pharyngeal tonsil hypertrophy and allergic process of the nasal mucosa, but apparently they are not responsible by deformity of the auditory tube during its growth.
Few authors have studied craniofacial morphology and middle ear infectious diseases. The cephalometric analysis used in our sample was based on anatomic location of the auditory tube and the measurements referring to the skull base and maxilla, as well as those determining facial type. The measures considered normal in the literature were defined in American subjects, but according to CERCI17, there is no difference when comparing them to Brazilian subjects in regards to skull base and maxilla.
Skull base measures
To analyze the skull base, we used the measures N-S, S-Ba; N-S.Ba e Ba-Na.Po-Or. We observed that the linear measure N-S, which represents the anterior fossa of the skull base, was smaller in the group of subjects with middle ear disease compared to the control group, however, this difference was not statistically significant, probably because our sample was small. Upon the comparison of mean and standard deviation of the middle ear disease group with the value reported by the literature as ideal for a proportional and harmonious face11, we observed that the subjects with middle ear disease presented a statistically significant smaller face. These data are in accordance with those by Jonas et al.18 Kemaloglu et al.6,8 and Mann et al.4 - in cephalometric analyses of children with tube dysfunction they found smaller skull base anterior fossa. Worley et al.7 and Stolovitzky; Todd19 found greater incidence of abnormalities in the tympanic membrane of brachycephalic subjects, that is, the ones with shorter anterior cranial base.
By analyzing the measures S-Ba, which represents the medial fossa of the skull base, we observed that subjects with middle ear disease present lower mean compared to the control group, but there was no statistically significant difference.
The measure N-S.Ba, which represents the angle between the anterior and medial fossae of the skull base, showed statistically significant difference with smaller values in the middle ear group compared to the control group. These data confirm the findings by Vidal 20, which found an association between abnormal tympanograms and reduced clivus angle.
The bone portion of the auditory tube is located in the temporal bone at the petrous-squamous suture that presents a close relation with the sphenoid and occipital bones21. The spheno-occipital synchondrosis is one of the most important in the skull base growth1. Its abnormal growth can result both in reduction of medial fossa dimension and angle of the anterior fossa, leading to abnormalities of the conformation of the bone portion of the auditory tube, which could influence its function.
The measurement Ba-Na.Po-Or (inclination of the skull base in relation to Frankfurt plan) did not present statistical difference in relation to the control, but rather in relation to the normal values in the population. We noticed that the measures of subjects with and without the middle ear disease are very similar and both present statistically significant differences compared to the measures in the literature11. This is the characteristic of our population that is in accordance with the data showed next. This angular measures does not provide the skull base dimensions, but rather the angle that is formed by the reference plan of Frankfurt. It shows that there are no differences in direction of growth, but in dimensions and in the relation of the anterior and posterior bases.
Maxilla-related measures
The anterior-posterior length of the maxilla, represented by ENA-ENP did not present statistically significant difference among the studied groups, meaning that there is no difference in size of palate/maxilla. This parameter has not been studied by other authors.
Considering the angular values, we observed that the comparison of the ENA-ENP.Po-Or measure (palatine plan in relation to Frankfurt plan) among the groups did not show statistically significant differences, not even when compared to the literature. This measurement relates the depth of the hard palate and the tendency to dental malocclusion, such as open bite. The high palate is associated with nasal obstruction and oral breathing, since nasal cavity expansion and palate migration depend on nasal function1. There was no influence of nasal obstruction in the samples and it apparently does not influence the auditory tube configuration.
By analyzing the cephalometric value P-Max - maxillary depth, it proved to be smaller in the group of middle ear diseases than in the control group, however there was no statistically significant difference. The great variation of measures in our sample, leading to large standard deviations, required large samples, which was not available in our study. Upon the comparison of values of subject with middle ear disease and ideal values for the population11, we obtained the value of p>0.5, showing that the studied group had smaller maxilla projection than the general population. Smaller maxilla projection contributes to the underdevelopment of length and/or different angle of the auditory tube, and it may lead to its dysfunction, since the anterior-inferior portion of the maxilla contributes to its more vertical position in the adults4, 6, 8.
The position of the auditory tube and its muscles in relation to the maxilla is the explanation for the tube dysfunction during childhood4, 5. The smaller projection of maxilla can be related with abnormal attachment of auditory tube muscles, since the attachment angle of tube muscles can affect the traction vector, interfering in the active opening of the auditory tube. This is one of the main reasons for auditory tube dysfunction in children4, 5.
Based on the findings referred above, we observed that auditory tube dysfunction is related to the relative position of the maxilla in relation to skull base (Figure 3).
Mandible-related measures
Linear measurements of mandible did not show differences in body size. As to angular measures, we observed that in relation to the harmonic ideal face, there were differences for the measures Mandibular plan, facial depth and Go-Me.Po-Or, which were larger in both studied groups. Such findings are probably characteristics of the studied population.
Facial height measures
We analyzed the linear measurements concerning facial height and observed that in our study, N-Me (total facial height) was smaller for the group with auditory tube dysfunction than the control group. The measure N-ENA referring to height of the middle third of the face has also proved to be smaller in the group of subjects with middle ear affection. Maxilla was anterior-inferiorly projected1 and, therefore, we could expect that a limited growth in the vertical direction of the middle third would influence the auditory tube function, and thus, would be correlated with greater incidence of otitis media.
Other measurements
The facial axis (EF) represents the direction of growth. Upon the analysis of craniofacial measures in relation to growth, we should consider the direction of the face as a whole and not only the isolated structures. In our study, we observed that there was no difference concerning the facial axis. Subjects with middle ear affection should not present abnormal growth, but maybe they could have incomplete growth, which leads to persistence of some childhood characteristics (determined by proneness to dysfunction) in the adult auditory tube. Maw22 suggested that the abnormalities of craniofacial morphology in children with serous otitis media would be resultant from delayed craniofacial growth.
Facial Types
In the analysis of frequency of facial types, we could observe that there was a predominance of dolichocephalic types. The VERT index uses measures mainly related to the mandible11. Therefore, we observed that this findings can be related to the characteristics of the studied population, which is in accordance with the studies by Atherino 24, who, upon analyzing the cephalometric measures in dry skulls of Brazilian subjects, a population similar to that of our study, found a predominance of dolichocephalic subjects, that is, long and narrow skull base and elongated face.
Comparing the cephalometric findings and the incidence of otitis in different races, we observed that Native Americans, which have brachycephalic characteristics23, are those that present the highest incidence of otitis media25, 26 among Caucasian subjects.
There are skull base differences among the various ethnic groups, especially concerning the main angle between the anterior and middle base in Black people14, and greater maxilla protrusion11, which can be related to Griffith findings (1979)28 of smaller incidence of otitis media in Black people. The different incidences of otitis in each race are not related to environmental factors or social-economic issues29.
It is known that subjects with cleft palate present a greater frequency of middle ear infections. In such subjects, there are skull base anomalies that probably influence the opening of the auditory tube. Children with cleft palate present a reduced N-S.Ba angle and reduced maxilla projection, associated with abnormalities of course and attachment of paratubary muscles30.
The analysis of data collected from the study has shown that there are similarities among the findings concerning the skull base and the maxilla of cleft palate people. There is probably an association between morphological and/or craniofacial growth micro-abnormalities with cleft palate in subjects prone to otitis that has not been studied yet. Todd26, upon studying the incidence of otitis in Apache Indians, found 20% of the subjects with microforms of uvula bifida, a percentage superior to that of American Caucasians. Thus, he concluded that Apache Indians could present genetically determined anatomical variations of the auditory tube, which could be associated with microforms of cleft palate.
Thus, we can conclude that there is in fact a correlation between craniofacial morphology and greater proneness to otitis.
The data from the present study showed us a correlation between craniofacial morphology and middle ear diseases.
We know how difficult it is to define predictive measures concerning the prognosis of middle ear diseases. The available techniques to assess auditory tube function are still considered insufficient to predict individually each case of secretory or chronic otitis media31.
Therefore, we suggest the cephalometric study in the assessment of middle ear disease evolution and to prevent craniofacial growth disorders that can contribute to the auditory tube dysfunction.
Conclusion
The group of subjects with middle ear diseases influenced by auditory tube dysfunction presented differences in craniofacial morphology as follows:
anterior fossa of the skull base was shorter;
smaller angle between the anterior and medial fossae of the skull base;
smaller anterior projection of the maxilla;
shorter facial superior anterior height;
shorter total facial height.
There was no predominant facial type.
Cephalometric values that had predictive value for middle ear disease influenced by auditory tube dysfunction were:
N-S (measure of the cranial anterior base)
N-S.Ba (angle between the anterior and medial base of the skull)
PMax (maxilla depth)
N-Me (facial height)
N-ENA (superior facial height)
Therefore, we proposed the cephalometric tracing that follows (Figure 4).
References
1. Enlow DH, Hans MG. Essentials of facial growth. Philadelphia: Saunders; 1996. 303p.
2. Mew JRC, Meredith GH. Middle ear effusion: an orthodontic perspective. J Laryngol Otol 1992;106:71-77.
3. Politzer A. Traité de maladie de loreille. Paris: Octave Doin Editeur; 1884. p.48-53.
4. Mann W, Jonas I, Munker G. Growth influence on tubal function. Acta Otolaryngol 1979;87: 451-57.
5. Holborow C. Eustachian tubal function. Arch Otolaryngol 1970;92: 624-6.
6. Kemaloglu YK, Göksu N, Köybasioglu A, Inal E, Özbilen, S. Prognostic value of craniofacial growth and development in children with secretory otitis media. In: Tos M, Thonsen J, Balle V. Otitis media today. Netherlands: Kyler Publications; 1999b. p. 81-91.
7. Worley G, Frothingham TE, Stuner RS. Head shape and middle ear effusion in children. AJDC 1987;141.
8. Kemaloglu YK, Kobayashi T, Nakajima T. Analysis of craniofacial skeleton in cleft children with otitis media with effusion. Int J Ped Otorhinolaryngol 1999;47: 57-69.
9. Vilella OV. Manual de Cefalometria. Rio de Janeiro: Guanabara Koogan; 1998.
10. Jarabak JR, Fizell JA. Technique and treatment with light-wire ederwise appliances. 2nd ed. Saint Louis: CV Mosby Co.; 1972. 1224p.
11. Ricketts RM, Roth RH, Chaconas SJ, Schullof RJ, Engel GA. Orthodontic diagnosis and planning. Rocky Mountain: Rocky Mountain Data Systems; 1982, 53-118, v.1.
12. Rosner B. Fundamental of biostatistics. 4th ed. EUA: ITP; 1995.
13. Costaras M, Pruzansky S, Broadbent Jr BH. Bony interorbital distance (BIOD), head size, and level of cribiform plate relative to orbital height. Normal standards for age and sex. J Craniofac Gent Dev Biol 1982;2:2-5.
14. DAloisio D, Pangrazio-Kulbersh V. A comparative and correlational study of the cranial base in North American Blacks. Am J Orthod Dentofac Orthop 1992;102: 449-55.
15. Bento RF, Marone S, Miniti, A. Tratado de Otologia. EDUSP; 1998. 488p.
16. Principato JJ. Upper airway obstruction and craniofacial morphology. Otolaryngol Head Neck Surg 1991;104: 81-90.
17. Cerci W, Martins JES, Oliveira MA. Cephalometric standars for white brazilians. Int Adult Orthod Orthognath Surg 1993;8: 287-92.
18. Jonas J, Mann W, Munker G, Junker W, Schumann K. Relationship between tubal function, craniofacial morphology and disorder of deglutition. Arch Oto-rhino-laryngol 1978;218:151-62.
19. Stolovitzky JP, Todd NW. Head shape and abnormal appearance of tympanic membranes. Otolaryngol Head Neck Surg 1990;102: 322-5.
20. Vidal SR, Sprekelsen C, Aranda MC, Estaca A. Disfunción tubárica, ángulo del clívus y ángulo de la base: uma posible relacion antropométrica. Acta Otorrinolaringol Esp 1988;39: 247-9.
21. Testut L; Latarjet A. Anatomía Humana. Barcelona: Salvat; 1976. p. 791-813.
22. Maw AR, Smith IM, Lance GN. Lateral cephalometric analysis of children with otitis media with effusion: a comparison with age and sex matched controls. J Laryngol Otolol 1991;10: 71-77.
23. Olivier G. Anatomie Antropologique. Paris: Vigot Frères Éditeurs; 1965. p.110-30.
24. Atherino CCT. Anatomia da parede medial da órbita: profundidade dos forames etmoidais e canal óptico e suas relações com as dimensões cranianas e orbitária no Brasil. 2000. Doutorado, Faculdade de Medicina da Universidade de São Paulo, São Paulo, 50p.
25. Spivey GH, Hirschhorn N. A migrant study of adopted apache children. Johns Hopkins Med J 1977;140:43-6.
26. Todd Jr NW. Otitis media at Canyon Day, Arizona: a 16 year follow-up in Apache indians. Arch Otolaryngol 1985;111:606-8.
27. Farrow L, Zarrinnia K, Azizi K. Bimaxillary protusion in black Americans an esthetic evaluation and the treatment considerations. Am J Orthod Craniofac Orthop 1993;104:240-50.
28. Griffth TE. Epidemiology of otitis media an interracial study. Laryngoscope 1979;89:22-30.
29. Shaw JR, Todd NW. Observations on the relation of environmental and behavioral factors to the occurrence of otitis media among indian children. Public Health Rep 1981;96:342-49.
30. Bishara SE, Sierk DL, Huang AS. A longitudinal cephalometric study on unilateral cleft lip and palate subjects. Cleft Palate J 1979;16:59-71.
31. Bylander-Groth A, Stenströn C. Eustachian tube function and otitis media in children. ENT J 1998;77:762-9.
1 Assistant Physician, Division of Otorhinolaryngology, FMUSP.
2 Assistant Physician, Ph.D., Division of Otorhinolaryngology, FMUSP, Head of the Facial Surgery Group.
3 Associated Professor, Discipline of Otorhinolaryngology, FMUSP.
Study awarded a Citation at II Congresso Triológico de Otorrinolaringologia, Goiânia, GO, 2001.
Part of the Doctorate Dissertation submitted to the Medical School, University of São Paulo, on March 28, 2001.
Address correspondence to: Rua Guarará 529 cj. 121 São Paulo SP 01425-001
E-mail: difran@attglobal.net
Article submitted on August 19, 2002. Article accepted on September 05, 2002


Print: ![]()