

Year: 2001 Vol. 67 Ed. 4 - (20º)
Relato de Casos
Pages: 575 to 578
Carcinoid Tumor of Sphenoid Sinus: Case Report.
Author(s):
Elder Y. Goto*,
Luciana M. Nita*,
Fábio T. M. Lorenzetti*,
Marcus M. Lessa**,
Richard L. Yoegels***,
Ossamu Butugan****.
Keywords: carcinoid tumor, neuroendocrine, sphenoid sinus, computed tomography
Abstract:
Neuroendocrine tumors of the nasosinusal tract are extremely rare. Carcinoid tumors develop from the neuroendocrine cells of the whole body, but they are found mainly in the gastrointestinal tract, bronchia and pancreas. Other locations are extremely uncommon and there are only two cases of carcinoid tumor reported in the nasosinusal area, located in the maxillary sinus. The objective of the present study was to describe a case of carcinoid tumor located in the sphenoid sinus. It was a male 33-gear-old patient, presenting bitemporal headache for 10 years without improvement after use of analgesic or non-hormonal antiinflammatory. He did not present symptoms of nasal obstruction, rhinorrhea or epistaxis. He denied any other systemic symptomatology. During otorhinolaryngologic exam, we noticed bilateral retraction of the tympanic membrane. At computed tomography (CT) of paranasal sinus, a solid mass occupying the sphenoid sinus and sella turcica was detected. The pathology result was carcinoid tumor. The patient was submitted to radiotherapy treatment for two months and CT control evidenced a new mass occupying the sphenoid sinus. We decided to conduct a surgical intervention to remove the tumor, but due to intense intraoperative bleeding, we just partially removed it. Pathology result of the surgical specimen confirmed carcinoid tumor. The patient is currently undergoing radiotherapy and chemotherapy treatment, presenting good therapeutic responses. Nasosinusal tumors are rare and may present poor symptomatology. We described a case of an extremely uncommon tumor in the upper airways, whose diagnosis was only possible through CT and pathology.
![]()
INTRODUCTION
Neuroendocrine tumors of the nasosinusal tract are extremely rare, and various types have been described, such as classic neuroblastoma, esthesioneuroblastoma, carcinoid tumor, paraganglioma, neuroendocrine carcinoma and small-cell carcinoma2,5,7,8.
Carcinoid tumors develop from the neuroendocrine cells of the whole body, but they are found mainly in the gastrointestinal tract, pulmonary bronchia and pancreas3,4,6. About 90% of these tumors originate from enterochromaffin cells (or Kulchitsky's cells), inside the gastrointestinal tract. Other primary sites are extremely rare7,8. The literature presents case reports of carcinoid tumor in the maxillary sinus9,10. The objective of the present study was to describe a case of carcinoid tumor located in the sphenoid sinus.
CASE REPORT
Male 33-year-old patient, technician in safety, born in Bahia and living in São Paulo for 26 years. The patient reported history of headache for about 10 years. The headache was bitemporal, pulsatile or constant, with no improvement after use of analgesic or non-hormonal antiinflammatory. There was progressive increase of severity and frequency of pain episodes in the previous years. The patient did not report nasal obstruction, sneezes, nasal pruritus, epistaxis or rhinorrhea. He did not report weight loss, other ENT complaints or any other sort of body complaint, either.
He did not refer any previous systemic diseases. The patient used to smoke one pack of cigarettes a day, but had no history of exposure to possible carcinogenic substances. He did not report family history of neoplasia.
At physical examination, the patient presented good general status and normal exam. ENT examination showed bilateral retraction of tympanic membrane, more marked on the right.
The patient was submitted to paranasal sinuses CT scan, at 5 mm coronal and axial sections, with venous injection of iodine contrast (Figures 1 and 2). Based on the CT scan findings, we suspected of chordoma.
After imaging diagnosis, we conducted a biopsy of the sphenoidal mass via endonasal access, whose pathology revealed carcinoid tumor.
The patient was then treated with radiotherapy sessions for two months, at 5,400 cGy dose. Upon the analysis of the control CT scan, we noticed increase of the mass in the same site.
The patient was then submitted to a new sphenoid sinus intervention through transnasal endoscopic surgery to remove the tumor. However, owing to abundant bleeding, we decided to conduct a partial resection, whose pathology confirmed the previous diagnosis.
The patient has been submitted to radiotherapy and chemotherapy treatment for two months now, presenting good clinical conditions. He is currently being prepared to a new endoscopic surgical approach.
Pathology
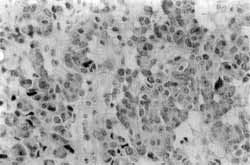
Histologically, the neoplasia from both samples presented blocks of small cells, with scarce basophilic cytoplasm, presenting finely granuled and rounded cytoplasm, with ovoid, regular, monomorphic nuclei and discreet mitotic activity (Figure 3).
Figures 1 and 2. CT scan of paranasal sinuses showing solid formation that compromises sella turcica and right sphenoid sinus, presenting erosion of clivus, sellar floor, and dorsum and lateral walls of sella turcica, characterizing a lesion closely in contact with the cavernous sinuses.
Figure 3. Pathology study: blocks of small cells, with scarce basophilic cytoplasm, presenting finely granuled and rounded cytoplasm, with ovoid, regular, monomorphic nuclei and discreet mitotic activity.
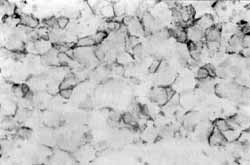
Figure 4. Immunohistochemical analysis: immunoexpression of chromogranin, synaptofisine and enolase.
Collagenic stroma was not clearly evident. Immunohistochemical analysis revealed immunoexpression of chromogranin, synaptoflsine and enolase, confirming neuroendocrine origin highly suggestive of carcinoid tumor (Figure 4).
DISCUSSION
Malignant tumors of nasosinusal tract amount to less than 1% of all body neoplasia and approximately 3% of upper respiratory tract tumors1.
Approximately 55 % of the nasosinusal tumors originate from the maxillary sinus, 35% from the nasal cavity, 9% from ethmoidal cells and only 1% from frontal and sphenoid sinuses1,5. As to histological type, they are divided into: a) epithelial line, such as squamous cells carcinoma, melanoma, neuroendocrine tumors (including carcinoid tumors), salivary glands, mucosa adenocarcinoma, teratoma and teratocarcinoma; b) nonepithelial line, such as those from soft tissues, connective tissue and lymphoreticular tumors; c) metastatic, especially renal and pulmonary. The most common type is squamous cell carcinoma, which amounts to 50 to 80 % of malignant tumors of the nasosinusal tract1,5.
Clinically, the tumor presents the same signs and symptoms of inflammatory diseases in the region, such as nasal obstruction, facial pain and headache, epistaxis and rhinorrhea. This fact hinders diagnostic suspicion, since 20 to 40 % of all otorhinolaryngological visits are related to nasosinusal tract inflammatory and/or infectious diseases. In addition to being extremely rare, these tumors are also asymptomatic in 9 to 12% of the patients during the initial stages of the disease1. All these factors lead to delay in diagnosis, which is generally made in advanced stages of the disease. In the case reported here, the only symptom was headache, whose cause was found out only 10 years after its onset. Owing to its location in the sphenoid sinus, symptoms such as nasal obstruction, epistaxis and rhinorrhea were not found.
The histological type concluded by the pathology analysis - carcinoid tumor - is very uncommon in the nasosinusal tract7,8. In the studied literature, there are only two cases of carcinoid tumor in the maxillary sinus9,10, and no reports were found for the sphenoid sinus. Carcinoid tumors are neoplasias originated from neuroendocrine cells of the whole body, but they are found mainly in the gastrointestinal tract, pulmonary bronchia and pancreas3,4,6. About 90% of these tumors originate from enterochromaffln cells (or Kulchitsky's cells), inside the gastrointestinal tract6. All carcinoid tumors are potentially malignant and tend to have an aggressive behavior depending on some factors, such as site of origin and tumor size. Risk factors for this tumor have not been defined yet.
Since they are from neuroendocrine origin, carcinoid tumors are capable of producing various syndromes or endocrinopathies, as a direct result of the hyper production of a specific biogenic amine or peptide hormone. Some of these neoplasias, especially those located in the gastrointestinal tract and ileum, are associated with a peculiar carcinoid syndrome characterized by paroxysmal blushing, episodes of difficult breathing, such as in asthma, right cardiac insufficiency, episodes of explosive watery diarrhea, abdominal pain, edema and skin and oral mucosa lesions similar to pellagra4,6. A number of secretory products have been identified, such as serotonin (5-hydroxytryptamine; 5 -HT), 5-hydroxytryptophphan (5-HTP), histamine, kallikrein and bradykinin; however, the main generating agent of the syndrome seems to be serotonin. The case of the patient reported here, whose tumor was located only in the sphenoid sinus, did not present other systemic or syndrome-related symptoms.
The diagnosis may be based on dosage of 5hydroxyindol acetic (5-HIAA), which is the main metabolite of serotonin in 24-hour urine2,4, and on biopsy of suspected lesions. In our case, the diagnosis was confirmed by pathology of the lesion in the sphenoid sinus, since clinically the patient presented poor symptomatology.
According to Cotran et al.3, the typical histopathological pattern involves solid nests of cells separated by a delicate mesh of connective tissue. Individual cells are extremely similar one to the other, presenting uniform size and cellular and nuclear shape. Nuclei are rounded and oval and very chromatic with fine dotting.
In general, there are abundant secretory cytoplasmatic granules stained in red with eosin, pale yellow with chromium salts, black with ferric hematoxyhn, and sometimes metallic black with silver salts. Perez-Ordonez8 and McCluggage7 reported that immunohistochemical analysis of neuroendocrine tumors showed positive reactivity to the following markers: CAM (5,2), neuron-specific enolase, synaptofisine and chromogranin.
Pathology of the surgical piece is compatible with the data described in the literature and immunohistochemicg analysis confirmed the diagnosis found.
The treatment includes surgical removal of the lesion, radiotherapy and/or chemotherapy.
Initially, we decided to perform radiotherapy. After two months of radiotherapy sessions we noticed growth of the tumor mass at the same site of the previous lesion. According to Cryer4, these tumors do not tend to respond well to isolated radiotherapy, recommending surgical removal whenever possible. Other authors2,3,6 have also considered tumor resection as the preferred treatment for these tumors. We conducted new surgical intervention, whose initial objective was removal of as much tumor as possible through transnasal endoscopic surgery. However, due to excessive intraoperative bleeding, we performed only partial resection of the tumor. The pathology analysis confirmed carcinoid tumor and currently the patient has been submitted to radiotherapy and chemotherapy for two months, presenting good clinical evolution and waiting for 'a new surgical intervention for tumor resection.
COMMENTS
Nasosinusal tumors are rare and present nonspecific symptomatology most of the times. We described a case of neuroendocrine tumor - carcinoid tumor located in the sphenoid sinus, whose occurrence is extremely rare in the upper respiratory tract. Due to the poor clinical presentation, only the analysis of CT scan and the pathology led to the diagnostic conclusion of isolated sphenoid sinus lesion; based on that, we managed to provide a therapeutic option to the patient.
REFERENCES
1. CARRAU, R. L.; MYERS, E. N. - In Bailey BJ et al; Head and Neck Surgery - Otolaryngology, 2a ed., Philadelphia, Lippincott-Raven Publishers, USA, 1998, pg. 1445-1470.
2. I.OFFEY, A. R.; PETTI Jr., G. H. - In Bailey BJ et al; Head and Neck Surgery - Otolaryngology, 2a ed., Philadelphia, Lippincott-Raven Publishers, USA, 1998, pg. 163-177.
3. COTRAN, R. S.; ROBBINS, S. L.; KUMAR, V - Pathologic Basis of Disease, 5a ed., WB Saunders Company, USA, 1994.
4. CRYER, E E. - In Wyngaarden, JB; Smith LH; Cecil Tratado de Medicina Interna, 18a ed., Ed. Guanabara Koogan, 1990, pg.1291-1292.
5. CUMMINGS, C. W - Otolaryngology - Head and Neck Surgery, 2a ed., Mosby Year Book, USA., 1993.
6. ISSELBACHER, K. J. et al; Harrison's - Principles of Internal Medicine, 13a ed., vol. 2, 1994.
7. McCLUGGAGE, W G.; NAPIER, S. S.; PRIMROSE, W J.; ADAIR, R. A.; TONER, E G. - Sinunasal neuroendocrine carcinoma exhibiting amphicrine differentiation. Histopatbology; 27 (1): 79-82, 1995 Jul.
8. PEREZ-ORDONEZ, B.; CARUANA, S. M.; HUVOS, A. G.; SHAH, J. E - Small cell neuroendocrine carcinoma of the nasal cavity and paranasal sinuses. Human Pathology; 29 (8): 826-32, 1998, Aug.
9. SRIUMPAI, S.; DHARAMADHACH, A. - Carcinoid tumor of the maxillary antrum: a case report. J. Med. Assoc. Thai; 65(1): 45-22, 1982 Jan.
10. YAMAMOTO, K.; SAKAI, S.; HONDA, M.; HYO, Y; HOSHIYA, T - Carcinoid tumour of the maxillary sinus. Jibi-Rinsho (Clip Otorhinol), 68: 965-971, 1975.
* Resident Physician, Discipline of Otorhinolaryngology, Hospital das Clínicas da Faculdade de Medicina, Universidade de São Paulo.
** Postgraduate Physician, Discipline of Otorhinolaryngology, Hospital das Clínicas da Faculdade de Medicina, Universidade de São Paulo.
*** Ph.D., Professor, Discipline of Otorhinolaryngology, Hospital das Clínicas da Faculdade de Medicina, Universidade de São Paulo.
**** Associate Professor, Discipline of Otorhinolaryngology, Faculdade de Medicina, Universidade de São Paulo.
Study conducted in the Department of Otorhinolaryngology, Hospital das Clínicas da Faculdade de Medicina, Universidade de São Paulo.
Study presented at 35° Congresso Brasileiro de Otorrinolaringologia, held on October 17- 20, 2000, in Natal/RN.
Address correspondence to: Elder Yoshimitsu Goto - Rua São Marcelo, 19 - 02250-050 São Paulo/SP - Tel: (55 11) 201-9144 - Fax: (55 11) 202-0827.
Article submitted on January 26, 2001. Article accented on March 9, 2001.


Print: ![]()