

Year: 2001 Vol. 67 Ed. 4 - (17º)
Relato de Casos
Pages: 557 to 557
Laryngeal Posterior Granuloma: Follow-Up After Botox Injection.
Author(s):
Noemi De Biase*,
Suely Master**,
Paulo Pontes***,
Simone De Biase****.
Keywords: larynx, granuloma, vocal fold, botox, botulinum toxin
Abstract:
Laryngeal posterior granuloma normally affects arytenoid region, usually over the vocal process, and it is related to three predisposing factors: vocal abuse, gastroesophageal reflux disease (GERD) and orotracheal intubation. If there is no evidence of these factors, we consider it as an idiopathic cause. Surgical removal leads to frequent recurrence, except in post-intubation cases. Treatment directed to triggering factors has shown promising results, but regression is not always achieved. Injection of toxin botulinum (Botox) in the vocal fold has been recently applied as an alternative procedure, producing good results in cases in which other treatment options had failed. Our aim was to report a case of laryngeal posterior granuloma, describing its follow-up and regression after Botox injection in the thyroarytenoid muscle.
![]()
INTRODUCTION
Laryngeal posterior granuloma normally affects the area that corresponds to the arytenoid vocal process and it is related to three predisposing factors: vocal abuse, gastroesophageal reflux disease (GERD) and orotracheal intubation7-9,12,15,16,20. In the absence of evidence of any of these factors, we consider idiopathic cause 16. It is a non-specific inflammatory process formed by granulation tissue1g, highly predominant in males, except in cases of post-intubation16. Since the first descriptions in the literature, the role of vocal abuse in its genesis has been stresses9; nevertheless, the preferred treatment used to be surgical approach, which produced frustrating results because recurrence was very frequent after surgery, except in cases of post-intubation2,10,16. The identification of triggering factors and cause-oriented treatment approaches have shown promising results6,7,16, but regression is not always achieved, especially in idiopathic cases, even when voice therapy is associated with GERD treatment16. Recently, the injection of botulinum toxin (Botox) in the vocal folds as an alternative approach for ineffective treatment results produced satisfactory responses 14,16. Botulinum toxin is a neurotoxin produced by gram negative anaerobic bacterium Clostridium botulinum, which acts selectively in the cholinergic nervous endings, blocking the release of acetylcholine chemical mediator3,11,19,21. The blockage of the mediator release on the neuromuscular junction causes functional muscle denervation, manifested by muscle paresis or paralysis. This neurotoxin-driven chemical denervation stimulates the growth of lateral axonal sprouts; the effect of Botox will last until one of the sprouts establishes a new neuromuscular junction, which usually happens within approximately three months1.
The purpose of the present study was to report a case of laryngeal posterior granuloma whose follow-up showed regression of condition after injection of Botox in the thyroarytenoid muscle.
CASE REPORT
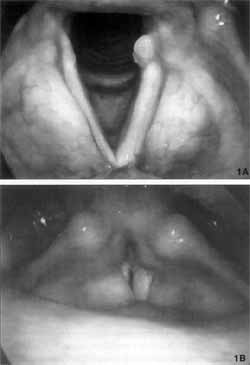
Patient aged 53 years, complaining of sore throat for 6 months, presented granuloma of the vocal process of the left arytenoid evidenced in the telelaryngoscopy (Figure 1a) and medialization of right vestibular fold during phonation (Figure 1b). Since there were symptoms suggestive of GERD, the patient was medicated with Omeprazole, 40 mg/day, and Cisapride, 20 mg/day, plus concomitant speech therapy to reduce tension during phonation. After 40 days of treatment, there was no regression of the granuloma and we indicated Botox injection. The patient was injected 5 UI of botulinum toxin via transcutaneous and transluminar access in the left thyroarytenoid muscle, after topical laryngeal anesthesia with neotutocaine at 2%, under fibroscopic visualization. The follow-up was carried out with telelaryngoscopy at days one, seven, thirty and one year after the injection.
Figure 1a and 1b. Telelaryngoscopy before Botox® injection-a: breathing, b: phonation.
RESULTS
Figures 1 to 5 show the images of the larynx of the patient before the injection with Botox and seven and thirty days and one year after the procedure.
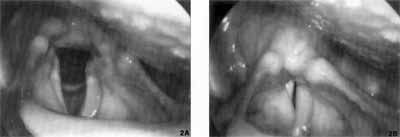
Figure 2a and 2b. Telelaryngoscopy 7 days after injection of Botox® - a: breathing, b: phonation.
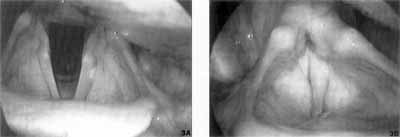
Figure 3a and 3b. Telelaryngoscopy 30 days after injection of Botox® - a: breathing, b: phonation
DISCUSSION
In cases of post-intubation granuloma, the mucosal trauma of the arytenoid region may generate a lesion whose repair causes the onset of a granuloma. The mucosa of the arytenoid region is thinner in women 20, which could explain the higher incidence of this kind of granuloma in female subjects. This fact per se does not explain the genesis of granuloma related to other triggering factors, since the cases not related to intubation seem to affect exclusively male subjects7,8,12,16. In order to explain this fact, we may evoke the laryngeal configuration of women, which is not similar to men's. The ratio between intermembranous and intercartilaginous portions (glottic proportion - GP) of male vocal folds is higher than female vocal folds, which makes the female larynx more susceptible to orotracheal intubation trauma on the posterior region17. Similarly to the cases of post-intubation, the causal factor of granuloma is not maintained; usually, there is spontaneous regression, regression thanks to aggressive speech therapy, or resolution after surgical exeresis, normally performed in larger and bilateral cases16.
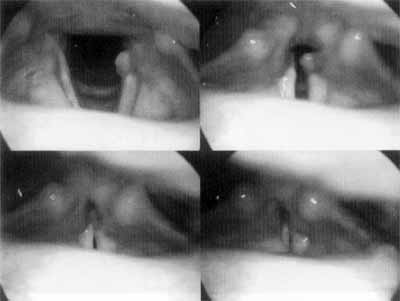
Conversely, the same female laryngeal configuration, in which triangular posterior or middle chink is frequent, because of GP, provides further protection to the arytenoid region, with less impact during the adduction of the vocal folds. Alternatively, the absence of posterior chinks in male larynxes, related to higher GP, makes the region more susceptible to receiving the initial impact of adductor forces of phonation (Figure 4). Figure 4 shows the approximation pattern of adduction of the vocal folds, starting from the vocal processes, in male larynxes.
Figure 4. Telelaryngoscopy showing the sequence of adduction for onset of laryngeal phonation, male pattern - impact on the arytenoid region.
In granulomas non-related to orotracheal intubation, one triggering factor may be vocal abuse9,16 responsible for the trauma in the arytenoid region during the adduction of vocal folds for phonation. Isolated GERD may cause chemical irritation of the posterior laryngeal region or non-phonation traumas, such as cough and throat clearing habits. These symptoms may be related to local irritation caused by the reflux, or a consequence of vagus reflex, or the result of both processes acting together15. Aggression caused by GERD may also be associated with vocal abuse. Treatment directed to these factors not always produce spontaneous regression of granuloma; in fact, even surgeries result in frequent recurrences16.
Our patient presented symptoms of reflux and signs of vocal abuse, with medialization of the right vestibular fold, evidenced at telelaryngoscopy (Figure lb). In view of that, we administered treatment both for GERD and vocal abuse, during 40 days, with no modification of granuloma size (Figures 1a and 1b).
Botulinum toxin has been frequently used to improve the voice in adduction laryngeal focal dystonia (spasmodic dysphonia)4,5,13. The chemical denervation that results in paresis of thyroarytenoid muscle and sometimes of lateral cricoarytenoid14 does not cause considerable alterations. Its use in granulomas aims at reducing adductor forces during phonation, swallowing, cough and throat clearing. The early follow-up of the Botox injected patient showed little modification of laryngeal mobility. However, seven days later, telelaryngoscopy showed paresis of left vocal fold and significant reduction of granuloma. As a side effect, the voice was breathy and soft because there was a chink during phonation (Figures 2a and 2b).
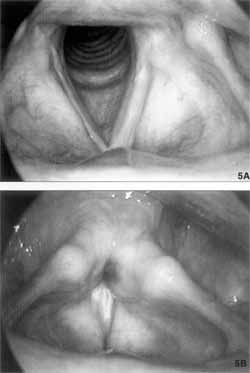
Figure 5. Telelaryngoscopy one year after injection of Botox®.
Thirty days after the injection, the granuloma had disappeared and there was significant improvement in vocal breathiness (Figures 3a and 3b). The evolution of the case indicated that the suppression or reduction of trauma in the arytenoid region was enough for the body to recover. The disappearance of Botox effect in the vocal fold occurred three months later. One-year follow-up showed the same hyperkinetic behavior and permanence of initial contact of arytenoid vocal processes at adduction (Figure 4). However, there was no evidence of the formation of a new granuloma, (Figures 4 and 5), demonstrating the long-term efficacy of treatment.
Except for the fact that the patient presented 30 days of breathy voice, which did not prevent communication and professional activities as head of personnel, Botox use showed great efficacy in this patient, with no occupational damage and low surgical costs.
FINAL COMMENTS
We concluded that Botox laryngeal injection is a great advance in the treatment of granuloma. It is a safe and effective procedure that may be used in cases that do not respond to clinical treatment.
REFERENCES
1. ALDERSON, K.; HOLDS, J. B.; ANDERSON, R. L. Botulinum-induced alteration of nerve-muscle interactions in the human orbicularis oculi following treatment for bhlepharospasm. Neurology, 41(11): 18005, 1991.
2. BENJAMIN, B. & CROXSON, G. - Vocal cord granulomas. Ann. Otol. Rhinol. Laryngol., 94: 538-41, 1985.
3. BLASI, J.; CHAPMAN, E. R.; LINK, E.; BINZ, T; YAMASAKI, S.; DE CAMILLI, E; SUDHOF, T. C.; NIEMANN, H.; JAHN, R. - Botulinum neurotoxin. A selectively cleaves the synaptic protein SNAP-25. Nature, 365: 160-3, 1993.
4. BLITZER, A. & BRIN, M. F. - Laryngeal Dystonia: a series with Botulinum Toxin Therapy. Arch. Otol. Rhinol. Laryngol., 100: 85-90, 1991.
5. BLITZER, A.; BRIN, M. F.; STEWART, C.; AVIV J. E.; FAHN, S. - Abductor laryngeal dystonia: a series treated with Botulinum Toxin. Laryngoscope, 102: 163-7, 1992.
6. BLOCK, C. S.; GOULD, W J.; HIRANO, M. - Effect of voice therapy on contact granuloma of the vocal fold. Ann. Otol., 90: 48-51, 1981.
7. CHERRY, J. & MARGULIES, S. I. - Contact ulcer of the larynx. Laryngoscope, 78: 1937-40, 1968.
8. FEDER, R.J. & MICHEL, M.J. - Hyperfunctional, hyperacid, and intubation granulomas. Arch. Otolaryngol., 110: 582-4, 1984.
9. JACKSON, C. - Contact ulcer granuloma and other laryngeal complications of endotracheal anesthesia. Anesthesiology, 14:425-36, 1953.
10. JAROMA, M.; PAKARNEN, L.; NUUTINEN, J. -Treatment of vocal cord granuloma. Acta Otolaryngol (Stockh), 107: 296-99, 1989.
11. KLEIN, A. W - Cosmetic Therapy with Botulinum Toxin. Dermatol. Surg., 22: 757-9, 1996.
12. MCFERRAN, D. J.; ABDULLAH, V; GALLIMORE, A. E; PATH, M. R. C.; PRINGLE, M. B.; CROFT, C. B. - Vocal process granuloma. J Laryngol. Otol., 108 (3): 216-20, 1994.
13. MILLER, R. H.; WOODSON, G. E.; JANKOVIC, J. Botulinum Toxin Injection of the Vocal Folds for Spasmodic Dysphonia. Arch. Otolaryngol., 113: 6035, 1987.
14. NASRI, S.; SERCARZ, J. A.; MCALPIN, T; BERKE, G. S. - Treatment of vocal fold granuloma using Botulinum Toxin Type A. Laryngoscope, 105: 585-8, 1995.
15. OHMAN, L.; OLOFSSON, J.; TIBBLING, L.; ERICSSON, G. - Esophageal dysfunction in patients with contact ulcer of the larynx. Ann. Otol. Rhinol. Laryngol., 92: 228-30, 1983.
16. PONTES, E; DE BIASE, N.; GADELHA, M. E. - Clinical evolution of laryngeal granulomas: treatment and prognosis. Laryngoscope, 109: 289-94.
17. PONTES, E; DE BIASE, N.; KYRILLOS, L.; PONTES, A. - The importance of glottic configuration in the development of posterior granuloma. Ann. Otol. Rhinol. Laryngol. (to be print).
18. SHUMRICK, K. A.; SHUMRICK, D. A.; VIETTI, M. J. Inflammatory diseases of the larynx. In: FRIED, M. - The Larynx: a multidisciplinary approach. 2°d. Ed. St Louis. Mosby. 1996, p. 283-306.
19. SIMPSON, L. L. - The origin, structure, and pharmacological activity of Botulinum Toxin. Pharmacol. Rev., 33(3): 155-188, 1981.
20. SNOW, J. C.; HIRANO, M.; BALOGH, K. - Post-intubation granuloma of the larynx. Anesthesia and Analgesia, 45: 425-9, 1966.
21. WIEDER, J. M. & MOY, R. L. - Understanding Botulinum Toxin. Dermatol. Surg., 24: 1172-4, 1998.
* Ph.D., Assistant Professor, Department of Biological Fundaments, School of Speech and Hearing Pathology, Pontifícia Universidade Católica de São Paulo - PUC - Specialist in otorhinolaryngology
** Master, Assistant of UNESP-IA. Speech and Hearing Pathologist, Specialist in Voice.
*** Faculty Professor of Otorhinolaryngology, Universidade Federal de São Paulo -Escola Paulista de Medicina. Director of INLAR - Instituto da Laringe - SP.
**** Undergraduate, School of Medicine, Pontifícia Universidade Católica de São Paulo.
Address correspondence to: Paulo Pontes - Rua Dr. Diogo de Faria, 171 - Vila Clementino - 04037-000 São Paulo/SP
Tel: (55 11) 5549-2188-Fax: (55 11) 5575-9649.
Article submitted on September 26, 2000. Article accepted on May 30, 2001.
Print: ![]()