

Year: 2001 Vol. 67 Ed. 3 - (19º)
Relato de Casos
Pages: 423 to 426
Spontaneous Hemorrhage from the Palatin Tonsils: A Case Report.
Author(s):
Miguel A. Hyppolito*,
José A. A. Oliveira***,
João V. Dorgam**,
Daniel D. C. Pinheiro*.
Keywords: palatin tonsils, tonsillitis, hemorrhage
Abstract:
Spontaneous hemorrhage from palatin tonsil is rare. Infectious mononucleosis is the most common etiology. Spontaneous loosing of the palatin tonsils, causing spontaneous oral hemorrhage, was not reported in our literature revision. On this case, we report a possible cause to spontaneous palatin tonsil hemorrhage without a infectious or a traumatic etiology.
![]()
INTRODUCTION
Spontaneous oral bleeding from palatine tonsil, with no iatrogenic cause, has been rarely reported10,8,11,3,5,1. In most cases, it is related to infections and causes of idiopathic nature, as described in the literature9,7,12.
Acute or chronic local infection processes lead to erosion of large vessels such as carotid artery or peripheral palatine tonsil vessels2,13. The erosion that affects large vessels normally results in major bleedings, which might be fatal. However, such a fact has not been observed since the advent of antibiotics.
Griffles et al., in 1998, analyzed 860 cases of oral bleeding and identified 10 cases of spontaneous palatine tonsil hemorrhage. Among them, eight had acute or chronic bacterial tonsillitis and the other two cases were related to infectious mononucleosis and tonsil neoplasia. These findings suggested that chronic tonsillitis would be a significant predisposing factor for spontaneous palatine tonsil bleeding. In the study, the authors observed that all cases of bleeding were from venous origin and from small peripheral palatine tonsil vessels3.
Other less frequent causes of tonsillar bleeding are trauma in the cervical and intraoral regions, forming cervical aneurysms and direct vascular trauma, respectively.
Palatine tonsillar abscess has been reported as a cause of major spontaneous tonsillar hemorrhage, and it may lead to septic necrosis of internal carotid artery; such cases have become extremely rare after the introduction of antibiotics2. However, minor bleedings are still observed and they present spontaneous resolution after the treatment of peritonsillar abscess.
The treatment advocated for spontaneous tonsillar hemorrhage, with peripheral vascular impairment of palatine tonsils and moderate bleedings, is tonsillectomy for definite resolution of the case, regardless of the predisposing bleeding or infectious nature.
In cases of major hemorrhage with suspicion of involvement of large arterial vessels, previous arteriography is advocated in order to identify the compromised vessel, conduct the selective ligature and, finally, perform the tonsillectomy.
In order to identify the possible causes of infrequent spontaneous palatine tonsillar bleeding we reported a clinical case treated in our service for the first time.
Case Report
Twenty-year old patient, a Caucasian married man, born in Ribeirão Preto, São Paulo, came to the emergency service of Hospital das Clínicas de Ribeirão Preto, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo, in February 1998. The patient reported a history of sudden oral bleeding, which had started approximately two hours before and progressed with middle-proportion bleeding. In addition to oral bleeding, he also reported pain on the left submandibular side, difficulty to open the mouth, odynophagia and sialorrhea: The patient reported ingestion of alcohol and fish, but did not correlate fish spines and the event. He did not report any type of oral or cervical trauma, or previous history of acute or chronic palatine tonsil infection or recent manifestations of fever.
As to personal history, the patient reported use of inhalation illegal drugs, but no use of injected drugs. He did not report any other infectious or contagious diseases or homosexual or promiscuous sexual behavior.
General and otorhinolaryngologic physical exam
The patient was in good general status, hemodynamically stable, anxious.
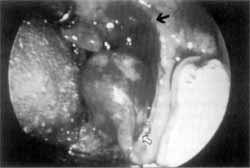
At the oral exam, he presented difficulty to open the mouth and moderate oral bleeding coming from the left palatine tonsil. The left palatine tonsil was detached from its site, pending in the oropharynx towards the hypopharynx, sustained by the inferior pole. The right palatine tonsil was difficult to evaluate but seemed to be normal (Photo 1).
Pre-operative exams
Hemoglobin; hematocrit, red and white cell line count.
Intraoperative period
The patient was submitted to tonsillectomy and we confirmed the findings of the ENT physical exam, but left palatine tonsil site was not damaged (Photo 1).
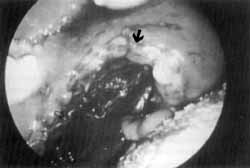
We also detected a bleeding lesion on the right anterior tonsil pillar at the superior pole, following the same characteristics as those found for the left tonsil (Photo 2).
The removed tonsils were sent to pathology and culture for aerobic agents, fungi and tuberculosis. The sample was not sent to anaerobic agent analysis because the laboratory was not available to receive it immediately
Post-operative period (Photos 3 and 4)
The patient did not present bleeding in the early post-operative period, showing apparently normal palatine tonsil site.
The patient was discharged after being submitted to serology.
Ten days post-operatively, the palatine tonsil sites showed apparently normal aspect.
Laboratory tests
The pathology revealed whitish multinuclear, fiberelastic palatine tonsils, presenting a whitish tissue with multiple sulci inside it and some darkened areas as well.
Photo 1. Intraoperative aspect of left palatine tonsil, showing the area of spontaneous detachment from where the bleeding originated (?) and left palatine tonsil sustained by its inferior pole (?).
Photo 2. Intraoperative aspect of right palatine tonsil, showing the area of spontaneous detachment on the anterior pillar, at the superior pole (?)
Photo 3. Post-operative aspect, showing left palatine tonsillar site. Note the difference between the spontaneously detached area (?) and the surgically detached area (?).
Photo 4. Post-operative aspect, showing the right palatine tonsil site. Note the difference between the spontaneously detached area (?) and the surgically detached area (?).
Conclusion: retrotonsillar abscess associated with chronic hypertrophic and cryptic tonsillitis.
Culture of palatine tonsillar tissue
Mycobacterium: negative (bacilloscopy and culture).
Fungi: negative for 48 hours and three months - Candida parapsulosis.
Aerobic agents: Klebsiella pneumoniae - ampicillin and carbenecillin-resistant.
Serology
Fungi, tuberculosis and infectious mononucleosis serology: negative.
Elisa anti-HIV negative
FINAL COMMENTS
Spontaneous acute tonsillar bleeding is a rare entity. In addition, in most cases it is associated with acute or chronic tonsil infection10,8,11,43,5,1.
The literature correlated those cases with tonsil affection by beta-hemolytic or viral Streptococcus (infectious mononucleosis)13 and rare cases of oral and cervical trauma or palatine tonsil neoplasia6,4. There were two case reports of idiopathic tonsillar hemorrhage described in the literature.
As far as manifestations are concerned, in addition to hemorrhage, there may also be detachment and fall of tonsil in the hypopharynx, which could result in upper airway obstructions.
In the case reported here, the clinical history and emergency complementary tests (blood count) did not show indications of infection.
We submitted the patient to tonsillectomy, as advocated in the literature, because the left palatine tonsil was collapsed in the oropharynx, with local hemorrhage and risk of upper airway obstruction.
Post-surgical laboratory tests, pathology and tonsillar tissue bacterial culture indicated potential chronic tonsillar infectious process, showing areas of local necrosis suggestive of local abscess. The tissue culture identified the presence of Klebsiella pneumoniae, but no other agents, such as beta-hemolytic streptococcus, were found.
The presence of Klebsiella pneumoniae in the oral cavity may be considered part of the local microbiota, which does not affect the subject. However, the sample was collected from the tonsillar tissue and no other pathogen that could have been responsible for the infectious picture was identified.
In the present case of spontaneous palatine tonsil hemorrhage, we have identified the cause of local infectious process, in accordance with the literature, but we did not confirm that the agent responsible for the tonsillitis was Klebsiella pneumoniae. Pathology results, showing areas of micronecrosis, suggested the presence of anaerobic agents; all in all, the cause may have been a multimicrobial agent.
REFERENCES
1. BAERTHOLD, W. - Haemorrhage from the ORL Area. Zeitscbrift fur Arztliche Fortbildung., 89(7): 703-706, 1995.
2. BLUM, D. J.; McCAFFREY, T. V. - Septic Necrosis of the Internal Carotid Artery: a Complication of Peritonsillar Abscess. Otolaryngol Head Neck Surg., 91(2): 114-118, 1983.
3. GRIFFIES, W. S.; WOTOWIC, E W; WILDES, T. O. Spontaneous Tonsillar Haemorrhage. Laryngoscope, 98(4):365-8, 1988.
4. HEFER, T; NETZER, A.; JOACHIMS, H. Z.; GOLZ, A. Upper Airway Obstruction -A Rare Complication After Anticoagulant Therapy. Harefuah., 124(6): 336-8, 1993.
5. JAWAD, J.; BLAYNEY, A. W - Spontaneous Tonsillar Haemorrhage in acute Tonsillitis. Journal of Laryngology & Otology., 108(9): 791-4, 1988.
6. JOHN, D. G.; THOMAS, E L.; SEMERARO, D. - Tonsillar Haemorrhage and Measles. Journal of Laryngology & Otology., 102(1): 64-6, 1988.
7. KOAY, C. B.; NORVAL, C. - An Unusual Presentation of Unusual Complication of Infectious Mononucleosis: Haematemesis and Melena. Journal of Laryngology & Otology., 109(4): 335-6, 1995.
8. McCORMICK, M. S.; HASSET, P - Spontaneous Haemorrhage From the Tonsil (A Case Report). Journal of Laryngology & Otology., 101(6): 613-6, 1987.
9. RIOS, O. A. B.; LESSA, R. M.; GRANATA, L. - Hemorragia espontinea da amigdala. Relato de caso a revisão da literatura. Rev. Bras. Otorrinolaring., 65(5): 901-4, 1999.
10. SINZINGER, G. - Clinical Contribution to the Problem of Spontaneous Hemorrhage From the Tonsils. Monatsscbr Ohrenbeilkd Laryngorhinol., 102 (5): 326-332, 1968.
11. SKINNER, D. W; CHUI, E - Spontaneous Tonsillar Haemorrhage: Two Cases. Journal of Laryngology & Otology, 101(6): 611-2, 1987.
12. SZEREMETA, W; NOVELLY, N. J.; BENNINGER, M. Postoperative Bleeding in Tonsillectomy Patients. Ear, Nose & Throat Journal, 75(6): 373-6, 1996.
13. TILLMANN, B.; CHRISTOFIDES, C. - The "Dangerous Loop" of the Internal Carotid Artery. An Anatomic Study. HNO., 43(10): 601-4, 1995.
14. VAUGHAN, M. M.; PARKER, J. - Idiopathic Spontaneous Tonsillar Haemorrhage. Journal of Laryngology & Otology., 107(1): 44-5, 1993.
* Physician, Department of Ophthalmology and Otorhinolaryngology - Area of Otorhinolaryngology, Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto - Universidade de São Paulo.
** Master studies under course, Department of Ophthalmology and Otorhinolaryngology - Area of Otorhinolaryngology, Faculdade de Medicina de Ribeirão Preto - Universidade de São Paulo.
*** Faculty Professor, Department of Ophthalmology and Otorhinolaryngology - Area of Otorhinolaryngology, Faculdade de Medicina de Ribeirão Preto - Universidade de São Paulo.
Study presented as poster at the 34° Congresso Brasileiro de Otorrinolaringologia, in Porto Alegre /RS, in 1999.
Address correspondence to: Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto - USP - Departamento de oftalmologia a Otorrinolaringologia.
Avenida Bandeirantes, 3900 - Campus Universitário - Monte Alegre - 14049-900 - Ribeirão Preto/SP
Article submitted on November 13, 2000. Article accepted on January 15, 2001.


Print: ![]()