

Year: 2001 Vol. 67 Ed. 2 - (15º)
Relato de Casos
Pages: 243 to 246
Syringocystoadenoma Paplliferum of the External Ear.
Author(s):
Roberto C. Meirelles*,
Marcelo M. Tepedino**,
Marcilio F. Marques Filho***.
Keywords: external ear, glandular tumor, adenomas, ceruminoma
Abstract:
The authors present a case of external auditory canal, in a 70 year old mate patient, with conductive deafness. After surgical excision, the pathologic diagnosis were syringocystoadenoma papilliferum, a rare form of benign neoplasm of sudoriparous glands.
![]()
INTRODUCTION
The term syringocystoadenoma comes from Greek: Syrinx means tube, kystis means balloon and aden means gland. Therefore, the term is imprecise and is normally confused with ceruminoma, adenoma and sialoadenoma9.
Syringocystoadenoma papilliferum is an extremely rare variation of a benign neoplasia originated from the sweat glands, which belongs to the adenoma group. It is normally manifested as a single verrucous plaque on the scalp, or is also presented in minor and major labii and perianal region. It has a nodular aspect, with cystic and papilliferous structure. It is commonly associated with different neoplasms, such as hamartoma7, sebaceous nevusland condyloma13. There is a report of common histologic aspects shared by three different tumors, in a single lesion: hidrocystoma, hidroadenoma and syringocystoadenoma12.
Immunohistochemistry and optic and electronic microscopy revealed characteristics that may classify it as a tubular apocrine adenoma2. In 10% of the cases, there was the association with basal cell carcinoma, but there were sebaceous nevi in all of them4.
CASE REPORT
N. B., 70-year-old Caucasian man, lawyer, lived in Nova Iguaçu, Rio de Janeiro. He came to our service complaining of progressive hearing loss on the left for about one year. For some months, he had been feeling ear fullness and autophonia. He had used a number of topic medications but none of them succeeded.
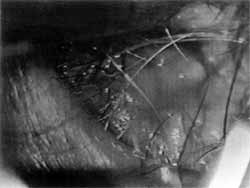
At otoscopy, we observed a single large tumor mass, hard, yellow, with irregular margins that occupied almost all the diameter of the left external ear canal, preventing visualization of tympanic membrane (Figure 1). Audiometry revealed mixed hearing loss on the left at about 50dB in all frequencies. Immitanciometry showed type B curve. CT scan showed circumscribed, single tumor mass apparently restricted to the external auditory canal, with velamentum of mastoid on the same side (Figures 2 and 3).
We conducted surgical removal of the lesion under general anesthesia, via retroauricular access and exploration of mastoid, which was not affected. We removed completely the lesion via endoaural access, followed by cauterization of the region where the tumor had been implanted. During surgery, we noticed integrity of tympanic membrane. Postoperative progression was uneventful. Control audiometry, conducted 30 days after surgery, revealed total recovery of conductive component of the mixed loss.
In the anatomic pathological analysis, macroscopy showed a nodular, irregular, light-brownish and firm mass, apparently encapsulated, measuring 2.0 x 1.5 x 1.3 cm. Upon sectioning, the surface was light brownish and homogenous. Microscopy (Figure 4) revealed epidermis both rectified and with irregular acanthosis. In the dermis, there were various cystic' cavities with innumerous papilliferous projections in the lumen, recovered by glandular epithelium, normally with a double cell layer. Occasionally, cells showed decapitation and cell debris in the lumen. In some areas, the cells of luminal layer were arranged in various layers. There was also a dense plasmacytic infiltrate in the dermis, among the glandular structures. Based on the findings, we made the diagnosis of syringocystoadenoma papilliferum.
Figure 1. Tumor aspect, obstructing almost all the external ear canal (6x microscopy).
DISCUSSION
In 1971, John Stokes described syringocystoadenoma papilliferum for the first time7,5. Since then, 189 cases have been reported9. About 75% of the cases affected the head and neck, 20%, the trunk, and 5% the upper and lower limbs7,1. Ear affection is extremely rare, amounting to 12 cases up to 19959. In approximately 50% of the cases, syringocystoadenoma is present at birth and in 15% of the cases, it is manifested during infant years5.
In the case of auricular presentation, it is localized in the external auditory canal and the onset is asymptomatic. As a result of its growth, the tumor obstructs the canal and impairs elimination of cerumen, causes ear fullness and transmission hearing loss. In many cases there is also secondary external otitis9, 5.
Diagnosis is merely histologic. Syringocystoadenoma papilliferous is normally a benign solitary tumor, with smooth or ulcerated surface, originated from sweat glands7,5,1. It is located in the fibrocartilaginous portion of the external auditory canal. It behaves either as a apocrine gland or as an eccrine gland7,10, projecting to the surface from the superior portion of the dermis1 and developing from pluripotential cell appendixes7,10. It is histologically characterized as having cystic invaginations in the epidermis, extending on the surface, and it has papillary projections shaped as villi, recovered by two layers of epithelial cells one deeper layer of epithelial cells and an external layer of cylindrical cells5,1. On the superficial epidermis, there may be acanthosis and hyperkeratosis, and in the dermis, a dense lymphoplasmacytic infiltrate may be present.
Figure 2. Single circumscribed tumor lesion, apparently restricted to the external ear canal. Homolateral mastoid velamentum.
The site of origin of the lesion is very controversial. Many believe that it derives from apocrine glands because they notice markers of these glands together with the gross cystic affection, fluid protein and epithelial antigens8. There are doubts whether or not the original cells come from apocrine glands. Histologically, the lesion consists of various different sized ducts connecting the lesion to the surface. There are two types of epithelial cells: internal and external cuboid cell layers6. Paradoxically, a number of studies showed that 90% of these lesions occur in areas that do not have apocrine glands. Moreover, apocrine gland formations occur in adolescents and most of these lesions are present at birth or develop during adolescence. It has been mentioned the presence of pluripotential cells, which could originate the lesions6, or the presence of intermediate cells between the two types4. Recent studies11 described the presence of one apocrine glands, explaining the finding of two types of glands in the lesion.
Treatment is mainly surgical. For reconstruction, closure may be primary or with graft. We did not find published discussions about the best access route to the tumor. We employed retroauricular access, with mastoid exploration, to investigate mastoid velamentum and make sure that the lesion did not compromise other important structures. The tumor, which was exclusively restricted to the external auditory canal, was removed via endoaural access, followed by cauterization of implantation site. As to alternatives to removal techniques, cryotherapy with nitrogen has been tried, but not very successfully5. Recent descriptions report the use of CO2 laser, applied to the pinna, with no intracranial prolongation5.
Figure 3. Detail of the tumor in the external ear canal.
Figure 4. Microscopic aspect.
It is important to remind otorhinolaryngologists that there are various rare types of cutaneous tumors that may compromise the external ear. We emphasized the importance of the histopathological exam in any excision biopsy, even if it seems unimportant, so that diagnosis may be finally confirmed.
REFERENCES
1. ANDERSON, W A. D.; KISSANE, J. M. - Patologia 7ª ed. Vo1.2, pp. 1522-1523, 1995.
2. EPSTEIN, B. A.; ARGENYI, Z. B.; GOLDSTEIN, G.; WHITAKER, D. - An unusual presentation of a congenital benign apocrine hamartoma. J. Cutan. Pathol., 17(1): 53-8, 1990.
3. GREER, K. E.; BISHOP, G. F.; OBER, W C. Syringocystoadenoma papilliferum retroauricular and nevus sebaceous. Arch. Dermatol., 112(2): 206-8, 1976.
4. HELLWIG, E. B.; HACKNEY, V C. - Syringocystoadenoma papilliferum: lesions with and without naevus sebaceous and basal carcinoma. Arch. Dermatol., 71: 361-72, 1955.
5. JORDAN, J. A.; BROWN, O. E.; BIAVATI, M. J.; MANNING, S. C. - Congenital syringocystoadenoma papilliferum of the ear and neck treated with the CO2 laser. Int. J. Pediatric Otorhinol., 38: 81-7, 1996.
6. LEVER, W F.; SCHAUMBERG-LEVER, G. -Tumors of the epidermal appendages. In. Histopathology of the skin. Lippincott, Philadelphia, pp. 544-6, 1983.
7. MAMMINO, J. J.; VIDMAR, D. A. - Syringocystoadenoma Papilliferum. International Journal of Dermatology., 30 (11), 763-766, 1991.
8. MAZOUJIAN, G; MARGOLIS, R. - Immunohistochemistry of gross cystic disease fluid protein (GCDFR15) in 65 benign sweat gland tumors of the skin. Am. J Dermatopathot, 10: 28-35, 1988.
9. MOLLER, R.; THEISSIG, F. - Syringocystadenoma papilliferum of the outer ear canal Laryngorhinootologie, 740): 43-5, 1995.
10. PINKUS, H. - Life History of Naevus Syringadenomatosus papilliferus. Arch. Dermatol. Syphilol., 69: 305-322, 1954.
11. SATO, K; SATO, F. - Sweat secretion by human axillary apocrine sweat gland in vitro. Am. J. Physiol., 252: 181-7, 1987.
12. SCHEWACH-MILLET, M.; TRAU, H. - Congenital papillated apocrine cystoadenoma: a mixed form of hidrocystoma, hidroadenoma and Syringocystoadenoma papilliferum. J Am. Acad. Dermatol., 11(2): 374-6, 1984.
13. SKELTON, H. G. 3'; SMITH, K. J.; YOUNG, D.; LUPTON, G. E - Condyloma acuminatum with Syringocystoadenoma papilliferum. Am. J. Dermatol, 16(6): 628-30, 1994.
* Joint Professor at Universidade do Estado do Rio de Janeiro, Ph.D. - Faculdade de Medicina da Universidade de São Paulo, Clinical Head of the Service of Otorhinolaryngology at Policlínica de Botafogo, Rio de Janeiro /RJ.
** Head of the Service of Otorhinolaryngology at Policlínica de Botafogo - Pró-Otorrino.
*** Former Resident Physician of the Service of Otorhinolaryngology at Policlínica de Botafogo - Pró-Otorrino.
Affiliation: Serviço de Otorrinolaringologia da Policlínica de Botafogo - Pró-Otorrino.
Study presented at 33° Congresso Brasileiro de Otorrinolaringologia, November 1 - 6, 1996, in Recife/PE.
Address for correspondence: Avenida Pasteur, 72 - Botafogo - 22290-240 Rio de Janeiro/RJ - Tel: (55 21) 543-1909 - Fax: (55 21) 543-1095.
E-mail: meirelles@radnet.com.br
Article submitted on January 6, 1999. Article accepted on March 19, 2001.



Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial