

Year: 2001 Vol. 67 Ed. 2 - (9º)
Artigos Originais
Pages: 196 to 201
Surgical Anatomy of the Round Canal.
Author(s):
Fernando Hayashi*,
Flávio M. Amado**,
João A. C. Navarro***,
Marcos L. Navarro****.
Keywords: sphenoid bone, round canal, maxillary nerve
Abstract:
Introduction: The access to the deep areas of the head requires a precise knowledge of it's topography and anatomic variations. Study design: Anatomical experimental. Material and method: In this study we searched the best denomination to the osseous formation that leads the maxillary nerve from the endocraneous to the exocraneous, if round foramen or round canal. Were made direct observations and through silicone (permilastic) moulding. We also verify the existence and frequence of ramifications of this nerve in it's intraosseous path in the sphenoid bone. Branches of the nerve in the canal were searched in 29 half adult heads, wich were demineralized and kept in formol. Results. The round canal regions were dissecated using a microscope and small maxillary nerves branches were found into the round canal in 15 (51,72%) of the cases. Branches had medial direction nine (60%), lateral four (26,67) and inferior two (13,33°/a). In one (6,67%) specimen three thinner branches were found.
![]()
INTRODUCTION
The increasing use of microscopy to perform surgeries in deep regions of the head and the improvement of diagnostic resources using images require constant reviews of craniofacial anatomy1,8,11,13. Consequently, some concepts have been reviewed, suggesting modifications of nomenclature and, in some cases, of location and relation of anatomical structures.
The bone element named round foramen, major round foramen or round canal, takes the maxillary nerve from endocranium to exocranium, specifically into the pterygopalatine fossa.
It is bilateral, located in the major ala of sphenoid bone, right below the upper orbital fissure, anterior to oval and spinosum foramens and lateral to the body of sphenoid.
The term round foramen3,4,5,7,9,10,14,17 was used by almost all studies investigated, whereas round canal was mentioned by only some of them12,18,19,20. The round canal is evidenced if we observe the lateral wall of sphenoid sinus, where it is normally a salient structure8,11,13. In the lateral expansions of the sinus, inside the major ala of the sphenoid, the round canal may be involved and become easily detectable.
Since it is a canal, its direction is from posterior to anterior and from medial to lateral, slightly bent downwards, and opening anteriorly in the pterygopalatine fossa. It also has a regular margin at the coronal plan, by the side of the fossa, whereas the cranial portion is in bevel from inferior to superior, following the inclination of the cranial wall of the major ala of sphenoid bone.
The present study intended to check the frequency of round canal and the existence of ramifications of the maxillary nerve inside it, which would penetrate through bone canaliculi from the walls of the canal.
MATERIAL AND METHOD
We used 32 macerated skulls, without calvaria, and the foramens/canals were measured in silicone molds (permilastic), with a metallic top supported on the endocranial opening of round foramen. From that point, we measured them using a pachymeter (Figures 4 and 5). Foramens were considered canals if they were longer or equal to 1mm (Lang)8.
For cadaver observation, we used 29 half heads of adults, formolized at 10% and demineralized with nitric acid at 5%.
Dissections of maxillary nerve, from its ganglionar origin up to inside the round canal and the emergence into the pterygopalatine fossa, were conducted from the skull middle fossa, using surgical microscope MC-900 (D. F. Vasconcellos), 200-mm objective and 12.5 mm oculars.
Dura mater of skull middle fossa around the round foramen was removed, together with the upper half of the foramen/canal, exposing the epineurium and carefully looking for branches and canaliculi, from the maxillary nerve and the round canal, respectively. Next, the maxillary nerve was sectioned close to its emergence into the foramen/canal, in endocranium, and slightly deviated at different plans so that we could look for intracanal ramification.
RESULTS
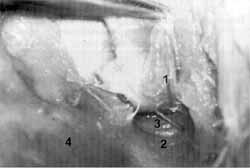
In direct osteologic observations and by means of molding, the round foramen was considered a canal if the extension in the major ala of sphenoid was equal or longer than 1mm. Therefore, we noticed that 32 (100%) of the cases had a canal and not a foramen (Figures 1 and 2).
The longest round canal - 7 mm, was observed in two cases (6.25%) and the shortest one - 1 mm, in three cases (9.35%), mean length of 3.8 mm.
As to diameter of round canal, the largest had 5mm in one case (3.12%), and the smallest - 2.5mm, in two cases (6.25%), mean diameter of 3.27 mm.
In all 29 (100%) dissections, we confirmed the existence of the round canal (Figure 6). In 15 (51.72%) of them, the maxillary nerve had ramifications inside the round canal, comprising one to three very thin accessory branches (Figures 3 and 7).
If single, the accessory branch presented medial direction in nine cases (60%), lateral in four (26.67%) and inferior in two cases (13.33%) (Table 1).
In four cases (26.67%) we found the zygomatic-orbital nerve originated from the interior of round canal, on the superior surface of maxillary nerve (Figure 8).
In only one case (3.44%) there were 3 accessory branches, all medially directed (Table 2).
DISCUSSION
Based on the concept described by Nomina Anatomica and referred by almost all authors as round foramen, this important anatomical element is in fact a canal. Described by some authors3,4,11,12, it was confirmed by the present study. It has an endocranial opening located on the major ala of sphenoid bone, close to the sphenoid body, and anteriorly in the junction of the ala with the pterygoid process of the same bone, in the most superior and lateral portion of pterygopalatine fossa. The posterior-anterior, medial-lateral and posterior-inferior path of round canal results in a lateral and inferior opening, related to endocranial, on the posterior wall of pterygopalatine fossa. The canal serves for the transit of the maxillary nerve and its artery and vein.
The presence of canaliculi from the wall of the canal and of thin branches of maxillary nerve that penetrate through the canaliculi towards sphenoid body has never been described in the literature.
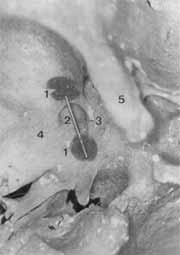
Figure 1. Skull middle fossa, left side: 1. Superior orbital fissure; 2. Narrow and elongated round canal; 3. Minor ala of sphenoid; 4. Sphenoid sinus.
Figure 2. Skull middle fossa, right side: 1. Superior orbital fissure; 2. Minor sphenoid ala; 3. Ample and short round canal.
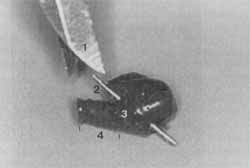
Figure 3. Skull middle fossa, right side: 1. Superior orbital fissure, 2. Minor sphenoid ala, 3. Ample, elongated and showing small openings on inferior-medial wall. 4. Accessory or emissary foramens of skull base.
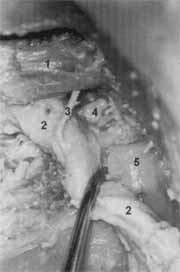
Figure 4. Skull middle fossa, left side half head: 1. Content of round canal pulled up; 2. Pterygopalatine fossa; 3. Round canal; 4. Major sphenoid ala.
Figure 5. Skull middle fossa, left side half head: 1. Content of the canal pulled up; 2. Ample round canal; 3. Thin branch of maxillary nerve directed to the inferior-medial wall of round canal, where it penetrates into the canaliculus; 4. Major sphenoid ala.
TABLE 1 - Dimensions of round canal in adult skulls using elastomeric mold with pachymeter (mm).
TABLE 2 - Occurrence and frequency of maxillary nerve ramifications inside the round canal and its respective direction, observed in dissections of half heads.
Figure 6. Skull middle fossa, left side half head. 1. Content of round canal pulled up; 2. Pterygopalatine fossa; 3. Round canal; 4. Major sphenoid ala.
Figure 7. Skull middle fossa, left side half head: 1. Content of round canal pulled up; 2. Ample round canal; 3. Thin branch of maxillary nerve directed to inferior-medial wall of round canal, where it penetrates into a canaliculus; 4. Major sphenoid ala.
Figure 8. Skull middle fossa, left side half head. Thin maxillary nerve in its path from the middle fossa, through the round canal, up to pterygopalatine fossa; 1. Attachment of temporal muscle in the interior of pterygopalatine fossa; 2. Maxillary nerve; 3. Orbital zygomatic nerve; 4. Pterygopalatine fossa; 5. Inferior wall of round canal, through which the thin branch of maxillary nerve penetrates.
The mean diameter of bone round canal was 3.27mm; the mean bilateral length was 3.8mm.
Out of 29 dissections (100%), we observed ramification of maxillary nerve inside the round canal in 15 cases (51.72%).
CONCLUSIONS
The round canal was found in all cases, both by direct osteologic observations and using molds, as well as in dissections.
The round canal had maximum length of 7.0mm and minimum length of 1.0mm, mean length of 3.8mm.
The largest diameter of round canal was 5.0mm, and the smallest was 2.5mm, mean diameter of 3.27mm.
Maxillary nerve was ramified in the round canal in 15 (51.72%) of the cases, forming very thin branches with medial path in nine of them (60%), lateral path in four (26.76%), and inferior direction in two cases (6.25%), penetrating in accessory canaliculi located on the walls of the canal.
REFERENCES
1. BECKER, S. E -Applied anatomy of the paranasal sinuses with emphasis on endoscopic surgery. Annals of Otology Rhinology & Laryngoscope, 103 (4): 3-32, 1994. Supl 162, part 2.
2. BIROU, G.; GARCIER, J. M.; GUILLOT, M.; VANNEUVILLE, G. and CHAZAL, J. -A study of the lateral pterygoid muscle: anatomic sections and CT appearances. Surg. Radiol. Anat. 13, 307-311, 1991.
3. CHIARUGI, G. - Istituzioni di Anatomia Dell' Uomo., 5, 171, 1965.
4. FIGLTN, M. E.; GARINO, R. R. - Anatomia Odontológica Funcional a Aplicada. 2a edição, Panamericana, São Paulo, 1989.
5. GARDNER; GRAY; O'RAHILLY - Anatomia-Estudo Regional do Corpo Humano. 2a edição, 758, 1967.
6. GOSS, C. M. - Gray - Anatomia. 29a edição. Guanabara, Rio de Janeiro, 1988.
7. HAMILTON, W J. - Textbook of Human Anatomy. Martin's Press, New York, 1958.
8. LANG, J. - Clinical anatomy of the nose nasal cavity and paranasal sinuses. Tieme Medical, New York. 1989.
9. LATARJET, M. LIARD, A. R. - Anatomia Humana, 1, 2ª edição, Panamericana, São Paulo, 1989.
10. LOCKHART, R. D.; HAMILTON, G. F.; FYFE, F. W - Anatomia do Corpo Humano. 2ª edição, Guanabara, p.39-300, 1983.
11. NAVARRO, J. A. C. - Cavidade do Nariz a Seios Paranasais. Anatomia Cirúrgica 1. All Dent, Bauru, 1997.
12. ORTS-LLORCA, F. - Anatomia Humana. Tomo III, 2a edição, Científico-Médica, Madrid, 1962.
13. RICE, D.; SCHAEFFER, S.- Endoscopic paranasal sinus surgery. Raven Press, New York, 1988.
14. ROUVIERE, H. - Anatomia Humana - Descriptiva y Topográfica. Tome 1, 3a edição, Masson, Paris, 1932.
15. SCHAEFFER, J. P - Morris' Human Anatomy 11ª ed. McGraw-Hill, New York, 1953.
16. SICHER, H. & TANDLER, J. -Anatomia para dentistas. Labor, Barcelona, 1960.
17. SICHER & DUBRUL. -Anatomia Oral. 8ª edição, Artes Médicas, 1975.
18. SPALTEHOLZ. W - Atlas de Anatomia Humana. V I, Roca, São Paulo, 1988.
19. TESTUT, L. & LATARJET, A. - Anatomia Humana. Vol. III, Salvat, Barcelona, 1959.
20. TONDURY, G. - Anatomia Topográfica y Aplicada. Científico-Médica, 1958.
* Dental Surgeon, Resident in the area of Dental Implants of HRAC-USP.
** Dental Surgeon.
*** Faculty Professor of the Discipline of Anatomy at Faculdade de Odontologia de Bauru, Universidade de São Paulo.
**** Undergraduate of School of Medicine, PUC-CAMP
Address for correspondence: Prof. Dr. João Adolfo Caldas Navarro - Faculdade de Odontologia da Universidade de São Paulo - Departamento de Ciências Biológicas - Disciplina de Anatomia - Alameda Dr. Octávio Pinheiro Brisola, 9-75 - 17012-901 Bauru /SP
Article submitted on September 1, 2000. Article accepted on December 7, 2000.




Print: ![]()