

Year: 2001 Vol. 67 Ed. 2 - (5º)
Artigos Originais
Pages: 171 to 178
Brainstem Evoked Response Audiometry in Elder With and Without Presbyacusia.
Author(s):
Marcos R. Freitas *;
José A. A. Oliveira**.
Keywords: presbyacusia, elder, auditory evoked potential
Abstract:
Introduction: The phenomenon of presbyacusia is still not fully understood in terms of its physiopathological mechanism, with ongoing debate about the participation of the cochlea and of the nervous structures that compose the auditory pathways in its genesis. Objective: The main objective of the present study were to assess the patterns of variation in I and V wave latency and of MU, III-V and I-V intervals of BERA in elderly subjects with and without presbyacusia and to compare them to those of young individuals in order to establish whether the changes in auditory threshold and discrimination observed in presbyacusic individuals are only cochlear in origin or whether there also a retrocochlear component. Study design: Clinical prospective. Material and methods: Fifty individuals with normal hearing and ten individuals with presbyacusia were submitted to brainstem evoked response audiometry (BERA) in both ears. The individuals were divided into six groups of 10 (five men and five women in each group) according to age and presence or absence of dysacusia. Results: The latency of I and V waves of the BERA is higher among presbyacusic than normoacusic individuals and is higher in males than in females, and that it increases linearly with increasing rate of emission of the sound stimulus. The intervals MU, III-V and I-V did not vary with age, sex or presence or absence of presbyacusia, and only increased with increasing stimulation rate. Conclusion: The increase in the latency of the I and V waves in presbyacusic individuals, taken together with the lack of significant variation in the I-V interval in these individuals, suggest a peripheral etiology of presbyacusia.
![]()
INTRODUCTION
The term presbyacusis 20 indicates the change in hearing function caused by aging, characterized by progressive hearing loss in high frequencies associated with poorer voice discrimination than what would be expected based on pure tone audiometry. This condition may affect about 40% of the subjects over the age of 75 years5.
The phenomenon of presbyacusis in its physiological details is still unknown, since it is argued what is the role in its genesis of the cochlea and the nervous structures that compose the auditory pathways. Based on this assumption, we decided to try to contribute to better understanding presbyacusis by studying the auditory pathways of subjects with presbyacusis by using brainstem evoked potentials audiometry (BERA), which for a long time has been an effective tool for topographic diagnosis of affections that compromise hearing, distinguishing them into cochlear and retrocochlear.
The objectives of the present study were:
1) To assess the variation patterns of latency of waves I and V and intervals I-III, III-V and I-V of Brainstem Evoked Response Audiometry (BERA) in elderly subjects with or without presbyacusis, comparing them to young subjects in order to establish if alterations of thresholds and hearing discrimination, showed in presbyacusis subjects, have a unique cochlear or retrocochlear component.
2) To assess the influence of gender in latency of waves and interpeak intervals and if the influence is somewhat related to age of subjects.
3) To observe the behavior of latency and interpeak interval with variation of stimulation rate by rarefaction of click. Also, to check if overload of stimulation of auditory pathways, with an increase in the production of click rates, affects differently young and elderly subjects with or without presbyacusis.
MATERIAL AND METHOD
BERA was performed in 60 subjects. All tests were performed using an evoked electrical response audiometer brand Nicolet CA2000, comprising sound source, monitor, pre-amplifier and headset type TDH-39.
After previous cleaning of the skin of the cranial vertex, frontal and ear lobes with ether and abrasive material, metal electrode bathed in silver chloride were positioned on these regions, as follows: active electrode, cranial vertex; reference electrode, ipsilateral earlobe; grounding electrode on the frontal region. After these electrodes were connected to the pre-amplifier, it checked to make sure that the impedance was below 4.000 Ohm.
We used stimuli of rarefaction clicks at a rate of 11.4s, 22.8s and 34.2s in each patient, and the number of acquisitions was proportional to the rate of release of clicks, respectively 2,000, 4,000 and 6,000 acquisitions. The increased number of acquisitions for each increase in click release rate is necessary in order to obtain more reproducible waves. Stimuli intensity was constant in 90dNHL, with masking of contralateral ear with white noise produced at 50dNHL. Generated potentials were amplified 100,000 times and filtered by a pass band of 150 and 3,000HZ. The total time for analysis was l0msec.
Patients were not expected to present any diseases that could interfere in wave latencies and amplitude of auditory evoked potentials, such as metabolic alterations (diabetes, hypercholesteronemia, hypertriglyceride), endocrinopathy, nephropathy, cardiopathy, arterial hypertension, neurological diseases. They were all submitted to otoscopy to have external and middle ear assessment, in addition to pure tone audiometry with vocal discrimination and immitanciometry, before the performance of BERA. In order to be included in the study, it was necessary to have tympanometric curve type An.
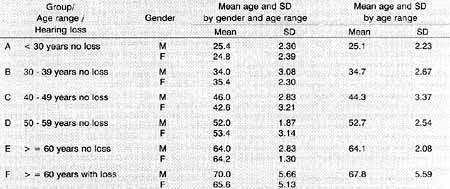
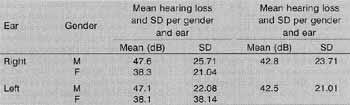
Subjects were divided into six groups, each of them with lb subjects, 5 male and 5 female subjects: group A, younger than 30 years of age normal-hearing subjects; group B, between the age of 30 and 39 normal-hearing subjects; group C, 40-49 year-old normal-hearing subjects; group D, 50-59-year old normal-hearing subjects; group E, older than 60 year-old normal-hearing subjects, and group F, older than 60-year-old subjects with presbyacusis. The mean age of each group is represented by Table 1. Each subject was submitted to right and left ear tests, totaling 100 normal hearing ears and 20 ears with presbyacusis. Normal auditory thresholds were considered those that had an average between 250, 500, 1,000, 2,000, 4,000, 6,000 and 8,000Hz lower or equal to 30dBHL. The average hearing threshold of patients in group F is represented in Table 2.
Tracings of waves I, III and V were perfectly identified and reproduced in at least the second stimulation, that is, there were at least two stimuli presentations for each stimulus.
Statistical analysis was carried out using the mathematical model adjusted to repetitive measures in the same subject, whose tests of main effects were carried out based on variance level. The sub-hypothesis tests were:
a) Orthogonal contrast test to adjust the analysis of profile of stimuli rates.
b) T -student, to compare the means of both genders.
c) Tuckey test, to compare in pairs the means of age ranges with and without hearing loss.
Hypotheses were tested at a maximum significance level (p) of 5%.TABLE 1 - Mean age of studied patients.
TABLE 2 - Mean hearing loss of patients who were at least 60 years and had hearing
loss (group F).
RESULTS
1. Latency analysis of wave I
The mean latency of wave I varied as a result of age (p=0.005), gender (p=0.040) and rate of stimuli (p=0.000).
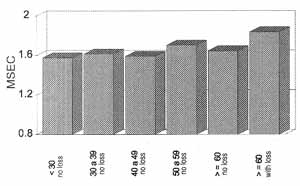
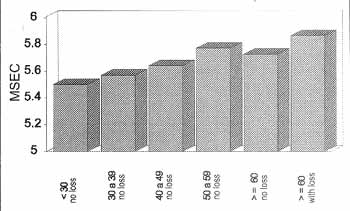
Within a significance level of 5%, there was a trend towards an increase in latency of wave I as a result of aging, and this difference was statistically significant among subjects younger than 50 years and those over the age of 60 years with presbyacusis. The group with presbyacusis was the one that had the highest wave I latency (Graph 1).
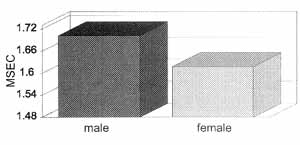
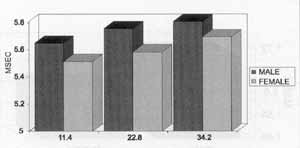
Male subjects had a mean latency of wave I consistently higher than the one from female subjects, in all age ranges (Graph 2).
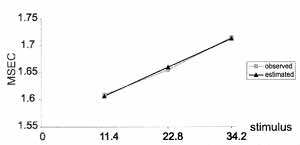
It was observed that there was a linear increase in latency of wave I as a result of increase in the rate of stimuli of 11.4 to 22.8 and to 34.2 clicks per second. This increase may be represented by the equation Latency = 1.5533 + 0.0047. It means that for an increase of 11.4 in rate of stimuli there has been an increase of 0.05msec in latency of wave I, as shown in Graph 3.
2. Analysis of latency of wave V
The mean latency of wave V differed as a result of gender (p=0.000), age (p=0.000), stimuli (p=0.000) and joint effect of gender and stimuli (p=0.027).
Aging was followed by increased latency of wave V within a significance level of 5%. and groups of subjects who were over 50 years of age with or without presbyacusis showed latency of wave V significantly higher than those aged below 30 years. As observed with wave I, subjects had higher latency than those with presbyacusis (Graph 4).
Graph 1. Mean latency observed in the ears and in wave 1, according to age with or without hearing loss.
Graph 2. Mean latency observed in the ears and in wave 1, according to gender.
Graph 3. Response curve of mean latency observed and estimated for the ears, according to stimuli of wave 1.
Graph 4. Mean latency observed in wave V according to ages with or without hearing loss.
As shown in Graph 5, male subjects had wave V latency in average higher than female subjects. However, this difference was only statistically significant (p < 0.05) with click rates at 22.4 and 34.2 seconds.
Wave V latency increased linearly as a result of the stimuli rate of male subjects, and this increase was represented by the equation Latency =5.5331 + 0.0099 (Graph 6). Therefore, for each increase of 11.4 in stimuli rate, there was an increase of 0.11 msec in latency of this wave.
Similarly to what happens in male subjects, in female subjects latency of wave V has also increased linearly with an increase in the stimuli rate and this increase is represented by the equation Latency = 5.4170 + 0.00789, that is, for an increase of 11.4 in the presentation stimuli click, there was an increase of 0.08msec in latency of wave (Graph 7).
3. Analysis of interlatency in interpeak I-III interval Interlatency of interval I-III varied in statistically significantly fashion as a result of stimuli rate (p=0.039), but it did not vary as a result of age or gender.
We observed that interlatency of interval I-III increased linearly as a result of the increase of stimuli rate. Its estimated relation is Interlatency = 2.1174 + 0.0025. Therefore, an increase of 11.4 in the stimuli rate corresponded to an increase of 0.2msec in this interval (Graph 8).
Graph 5. Mean latency observed in wave V according to gender and stimuli
Graph 6. Response curve of mean latency observed and estimated for wave V according to stimuli in male subjects.
Graph 7. Response curve of mean latency observed and estimated for wave V according to stimuli in female subjects.
Graph 8. Mean interlatency observed for interpeak interval I-III according to stimuli.
4. Analysis of interlatency in interpeak I-V interval
Similarly to interval I-III, mean interlatency of interval I-V only showed statistically significant difference as a result of the stimuli (p=0.000).
The relation of interlatency in interval I-V as a result of stimuli is linear and growing, and the estimated relation is Interlatency= 3.8977 + 0.0051. Therefore, this interval increases in 0.05msec for an increase of 11.4 in stimuli rate (Graph 9).
5. Analysis of interlatency in interpeak III-V interval
Also here there was a variation in interpeak III-V as a result of stimuli rate (p=0.000).
Similarly to the other intervals, interval III -V also increased linearly as a result of the increase in stimuli rate and this variation is represented by Interlatency equation = 1.7856 + 0.0025. Thus, if we increase in 11.4 the click stimulation rate, there is an increase corresponding to 0.02msec of interval. III-V (Graph 10).
DISCUSSION
Brainstem auditory evoked potentials have been a valuable instrument for topodiagnosis of hearing disorders. Since its definition, by Jewett in 1971, the waves of early auditory evoked potentials and its possible locals of origin6, a number of authors have published studies emphasizing the importance of BERA in the diagnosis of retrocochlear diseases. In 1976, Starr and Hamilton described the possible origins of waves I and V and demonstrated the value of BERA in the diagnosis of central nervous system disorders16.
Since the creation of the term presbyacusis20 by Zwardemaker in 1894, a number of authors have discovered about the pathophysiological mechanisms of the entity. Some studies tend to relate the alterations of BERA in elderly patients and/or presbyacusis patients, although the results of different studies are extremely disputable.
Therefore, our study does not intend to be definite concerning pathophysiology of presbyacusis, but to create an extra parameter to guide the discussions concerning the topic.
Graph 9. Mean interlatency observed and estimated for interval IV according to stimuli.
Graph 10. Mean interlatency observed and estimated for interval III-V according to stimuli.
Latency of waves I and V varied as a result of age, gender and rate of stimuli and there was a joint effect of gender and stimuli concerning wave V.
Despite the tendency of increase of wave I as a result of aging, there was no statistically significant difference among patients with normal hearing. Statistical significance was observed only for the group below 50 years of age and those aged 60 or more with presbyacusis. Wave V was also significantly higher in presbyacusic elderly patients than in those subjects aged less than 50 years with normal hearing. These results are in accordance with the studies by Rosenhall et al. (1986)12 and Martini et al. (1991), who showed increase of latency of all components of BERA in subjects with presbyacusis, and they also showed that latency modifications are more related to the shape of the audiogram rather than the age itself, ,as proposed by Watson em 199619. Patients with sensorial high frequency losses have shown higher latency of wave I, which is secondary to the activation of more basal portions, than wave V that results from a more diffuse activation of the cochlea.
Male subjects reached wave latencies higher than female subjects. However, for wave V this difference was statistically significant for stimuli rates of 22.8 and 34.2 clicks per second. A number of other studies1,19 showed similar results. This difference is probably due to the size of the head and brainstem that are relatively larger in male than females, providing a longer distance between the generating source and the electrodes that capture electrical activity, or due to other factors, such as length of external auditory canal or diameter of auditory nerve1,17.
Considering the stimulation rate of rarefaction clicks, we observed a linear increase in latencies of waves I and V as a result of increase of stimuli rate. The same ratio was found by the studies of Don et al.4, 1977, Rowe13, 1978 and Soucec and Mason15, 1992. Don et al. suggested that this increase in wave latency would be connected to a mechanism of neural fatigue and accomodation4. These phenomena occur as a result of metabolic alterations of neural receptors after its activation. Sensorial systems require a determined period of time followed by the appropriate stimulus to completely restore its responsiveness. If a new stimulus occuirs before this period, the system will respond abnormally (latency either attenuated or prolonged).
In all three intervals, there was a variation of interlatency related only to stimuli rate, that is to say, interpeak intervals varied linearly and in a growing fashion as a result of the increase in click production rate.
As to stimulus rate, our results confirmed the findings by Rowe13, in 1978, and Stockard et al.17, also in 1979, but the former did not notice variation of III-V interval. The extension of intervals is explained by the phenomenon of adaptation, when repeated stimuli, without the appropriate interstimulus time (IST) lead to reduction of the number of stimulated fibers, as well as reduction of stimulus/frequency of discharge of nervous fibers, such as proposed by Thorton and Coleman 18 in 1975.
Most of the studies that correlated variations of BERA concerning gender have shown that male subjects have higher interpeak intervals than female subjects1,11,17,19. The authors explained this variation because of the difference in size of the brain of men and women. Brain volume in men is in average 10 % larger than in women3. On the other hand, central nervous pathways vary in length as a result of the cube of the brain volume14. Therefore; the highest amount of interpeak interval in male subjects compared to female subjects may be due to a wider compromise of central auditory pathways in the former. In our study, despite the fact that general intervals I-III, III-V and I-V were higher in men than in women, there was no statistically significant difference with the statistical method employed.
The variation of interlatency compared to age and presbyacusis was the parameter that remained uncertain. Studies conducted in normal hearing subjects revealed a progressive increase of intervals, especially of I-V interval as a result of aging9,13. Others related increase of interval I-V in elderly presbyacusic patients with normal hearing young subjects. They advocated that this increase was due to central nervous system alterations of the brainstem, present in the presbyacusis1,8,12. However, studies by Rosenhall et al.11, 1985, Martini et al.7, 1991, Ottaviani et al.10, 1991, Soucec and Mason15,1992 and Watsonl9, 1996, excluded the brainstem as a possible contributing factor for the genesis of presbyacusis. In our study, there was no statistically significant difference in studied intervals (I-III, I-V and IIIV) related to age or presence of presbyacusis, confirming the findings of those authors. This fact, associated with the absolute latency of waves I and V in presbyacusic subjects, suggested a cochlear origin of the condition.
Most studies that presented a positive association between presbyacusis and brainstem pathology did not analyze pure tone thresholds and the shape of the audiogram, which may influence interlatency interval I-V as described by Ottaviani et al.10, in 1991 and Watson19 in 1996. The first authors compared the interval I-V of elderly presbyacusis patients to young subjects with acoustic trauma (a known cochlear lesion), with similar pure tone thresholds and audiogram shape, and there was no statistically significant difference. The second author stated that wave I had latency increase associated with increase of high frequency thresholds, whereas increase of wave V latency was associated with inclination of descending audiogram curve.
Despite the fact that the studies by Behse and Buchthal (1971)2 stated that speed of nervous conduction reduces with age, our study did not show extension of intervals IIII, III-V and I-V in elderly subjects with or without presbyacusis. We may conclude that auditory pathways of brainstem are not affected by a measurable degree in these subjects, that is, damage in presbyacusis is predominantly peripheral.
CONCLUSIONS
1) Absolute latencies of waves I and V are higher in elderly subjects with presbyacusis when compared to those of young normal hearing subjects.
2) Men have higher wave I and V latencies than women, which is probably related to larger cranial volumes in males; consequently, the generating wave source is farther from the surface of the electrode.
3) Latency of waves I and V and interpeak intervals I-III, I-V and III-V increase linearly as a result of the increase of click production rate, and this finding is explained by the phenomena of neural fatigue and accommodation.
4) There was no variation of any of the interpeak intervals related to subjects' gender.
5) In no interpeak intervals there was variation related to age or presence or absence of hearing loss, and that, associated with increase in latency of waves in presbyacusic subjects, suggested the cochlear origin of the pathology.
ACKNOWLEDGEMENT
To Professor Rosa Mota, from the Department of Statistics and Applied Medicine at Universidade Federal do Ceará, for the statistical analysis of the results.
To Ms. Maria Rossato, lab technician of the Division of Otorhinolaryngology at HCFMRR-USP, for having selected patients and conducted the tests.
REFERENCES
1. ALLISON, T.; WOOD, C. C.; GOFF, W R. - Brain stem auditory, pattern-reversal visual and short latency somatosensory evoked potentials: latencies in relation to age, Sex and brain and body size. Electronencephalogr Clin. Neurophysiol., 55: 619-36, 1983. 2. BHHSE, F.; BUCHTAL, F. - Normal sensory conduction in the nerves of the leg in man. J. Neurosurg. Psychiatry, 34: 404-14, 1971.
3. DEKABAN, A. S.; SADOWSKI, D. - Changes in brain weights during the span of human life: relation of brain weights to body heights and body weights. Ann. Neurol, 4: 345-56, 1978.
4. DON, M.; ALLEN, A. R.; STARR, A. - Effect of click rate on the latency of auditory brain stem responses in humans. Ann. Otol., 88: 186-95, 1977.
5. GATES, G. A.; CASPERY, D. M.; CLARK, W; PILLSBURY, H. C. III; BROWN, S. C.; DOBIE, R. A. - Presbyacusis. Otolaryngol. Head Neck Surg., 100: 266-71, 1986.
6. JEWETT, D. L.; WILLISTON, J. S. - Auditory far fields averaged from the scalp of humans. Brain, 94: 681-96, 1971.
7. MARTINI, A.; COMACHIO, F.; MAGNAVITA, V - Auditory evoked responses (ABR, MLR, SVR) and brain mapping in the elderly. Acta Otolaryngol. (Suppl), 476: 97-104, 1991.
8. MAURIZI, M.; ALTISSIMI, G.; OTTAVIANI, F.; PALUDETTI, G.; BAMBINI, M. - Auditory brainstem responses (ABR) in the aged. Scand Audiol, 11: 213-21, 1982.
9. OKU, T.; HASEGEWA, M. - The influence of aging on auditory brainstem response and electrocochleography in the elderly. ORL J Otorhinolaryngol. Relat Spec., 59 (3): 141-46, 1997.
10. OTTAVIANI, F.; MAURIZI, M.; D'ALATRI, L.; ALMADORI, G. - Auditory brainstem responses in the aged. Acta Otolaryngol. (Suppl), 476: 110-3, 1991.
11. ROSENHALL, U.; BJORKMAN, G.; PEDERSEN, K.; KALL, A. - Brain-stem auditory evoked potentials in different age groups. Electronencephalogr. Clin. Neurophysiol., 62: 42630, 1985.
12. ROSENHALL, U.; PEDERSEN, K.; DOTEVALL, M. -Effects of presbyacusis and other types of hearing loss on auditory brainstem responses. Scand Audiol., 15: 179-85, 1986.
13. ROWE III, M. J. - Normal variability of the brain-stem auditory evoked response in young and old adult subjects. Electronencephalogr Clin. Neurophysiol., 44:459-70, 1978.
14. SCHIMIDT-NIELSEN, K. - Scaling in biology: the consequences of size. J Exp. Zool., 194: 287-307, 1975.
15. SOUCEC, S.; MASON, S. M. - Effects of adaptation on electrocochleography and auditory brain-stem responses in the elderly. Scand. Audiol., 21 (3): 149-52, 1992.
16. STARR, A.; HAMILTON, A. - Correlation between confirmed sites of neurological lesions of far-field auditory brainstem response. Electronencephalogr. Clin. Neurophysiol., 41: 595-608, 1976.
17. STOCKARD, J. E.; STOCKARD, J. J.; WESTMORELAND, B. F.; CORFITS, J. L. - Brainstem auditory-evoked responses: normal variation as a function of stimulus and subject characteristics. Arch. Neurol., 36: 823-31, 1979.
18. THORTON, A. R. D.; COLEMAN, M. J. - The adaptation of cochlear and brainstem auditory evoked potentials in humans. Electronencephalogr Clin. Neurophysiol., 39: 399-406, 1975.
19. WATSON, D. R. - The effects of cochlear hearing loss, age and sex on the auditory brainstem response. Audiology, 35 (5): 246-58, 1996.
20. ZWAARDEMAKER, H. - The range of hearing at various ages. Z. Psychol., 7: 10-28, 1894.
* Assistant Professor of Otorhinolaryngology at Faculdade de Medicina da Universidade Federal do Ceará.
** Faculty Professor and Head of the Department of Otorhinolaryngology and Ophthalmology at Hospital das Clínicas da Faculdadede Medicina de Ribeirão Preto -USP.
Study conducted at the Department of Ophthalmology and Otorhinolaryngology of Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto - USP.
Presented as a free paper poster at 34° Congresso Brasileiro de Otorrinolaringologia, held in Porto Alegre/ RS on November 18 - 22, 1998 and as a conference at I Congesso
Triológico de Otorrinolaringologia, held in São Paulo/ SP on November 13-18, 1999.
Address for correspondence: Departamento de Cirurgia da Faculdade de Medicina da Universidade Federal do Ceará - Rua Professor Costa Mendes, 1608 - Rodolfo Teófilo - 60430-140 Fortaleza /CE - Tel/fax: (55 85) 288-8065.
Article submitted on June 14. 2000. Article accented on December 7, 2000.
Print: ![]()