

Year: 2001 Vol. 67 Ed. 1 - (4º)
Artigos Originais
Pages: 29 to 35
The Voice of Hearing Impaired Children.
Author(s):
Maria C. Giusti*,
Marina M. P. Padovani*,
Maca Behlau**,
Lídio Granato***.
Keywords: acoustic analysis, deafness, voice
Abstract:
Introduction: Hearing has an important role in the achievement of the oral language and the control of the vocal production. Aim: This work investigated the impact of deafness in vocal function and has the aim to evaluate the fundamental frequency and its variability in children's voices with and without sensorioneural hearing impaired from severe to profound levels and also to compare their voices with normal children's voices. Material and method: The subjects of this study were 64 children with pre-lingual deafness from severe to profound levels, age six to 13. The experimental control group was composed by 90 children, without any communication disorders. Each one emited the sustained vowels "a", "i" and "u". The acustic analysis was achieved by the Dr. Speech Sciences (version 4.0). The perceptive auditory evaluation was done by Speech language pathologists speciallysed in voice. Results: We have found a high fundamental frequency (435 Hz) and a great variability (13 semitons) in deaf children comparing to normal children (264 Hz and on semiton). Those vocal characteristics used by deaf people, make us to be able to identify them perceptually (90% positive). Conclusion: Therefore, severe to profound deafness presents a poor laryngeal control and great phonatory instability. This study reinforce that the voice of a hearing impaired individual must be specifically focused to minimize the social impact of deafness.
![]()
INTRODUCTION
Hearing has a key role in oral language acquisition. Severe and profound hearing losses may have a devastating effect in language development and communication is essential not only for the interaction in a healthy social environment but also to help personal and emotional development.
A severe or profound deaf child presents speech development away from the normal range. Normal hearing people rely mainly on auditory signs to develop language: hearing impaired children have to supplement hearing with visual and tactile clues, in addition to other specific strategies according to the treatment approach followed. The different monitoring strategies make hearing impaired children create their own system of vocal production, resulting in great difference between them and normal hearing subjects.
Vocal quality of severe or profound hearing impaired children is normally considered deviated from the auditory perceptual and acoustic perspective. According to Calvert8, the terms commonly used to describe it are tense, breathy, harsh, out of tune and guttural.
Vocal deviations presented by them may interfere in speech intelligibility and compromise the social integration of the individual, because their vocal quality is constantly rejected by hearing people. In the process of rehabilitation of the communication of hearing impaired children therapists usually concentrate on articulation and frequently neglect rehabilitation of vocal function.
Despite the fact that the incidence of vocal disorders is very high in hearing impaired people, there is limitation of objective data that describe the acoustic characteristics of their vocal quality.
Hearing impaired children normally present difficulties to control laryngeal function during speech, resulting in abnormal vocal quality 8,13,14,17,19. Monsen et al. 15 observed that some deaf people have episodes of diplopia and voice cracking, as well as irregular patterns of change of glottic frequencies and intensity, denoting inability to control tension of the vocal folds and subglottic pressure.
There is a consensus among various authors 7,9,15,16,21 that the phonation effort of the hearing impaired is a result of insufficient air flow and subglottic pressure, disturbing aerodynamics of vibration and leading to muscle effort higher than normal and/or an increase in vocal tension to produce and maintain phonation. The effort results in poor speech intelligibility.
The difficulty to maintain the appropriate tension balance between the vocal folds during phonation may explain the harsh vocal quality that is frequently found in the hearing impaired 21,25,27. Besides harshness, excessive tension provides elevation of fundamental frequency 11,16,17. In the description of vocal deviations presented by the hearing impaired, the authors normally refer to inadequate fundamental frequency 8,11,16,18,22, and variability 1,8,10,13,15,16,18,22,27, two acoustic parameters that are extremely important for identification and qualification of voice by the listener.
The literature presents considerable controversy about the values of fundamental frequencies in the voice of hearing impaired children. Some authors reported values within normal ranges 6,10,14,15,20,23,26. Boone6 emphasized that hearing impaired children aged between 7 and 8 years have habitual frequency similar to normal hearing children; however, as they grow, there is no reduction of frequency, as expected from normal hearing adolescents. Osberger and McGarr²° concluded, after a review of a number of studies, that there is no significant difference between fO of hearing impaired children and normal hearing children between the ages 6 and 12. Monsen14, upon studying a group of hearing impaired children aged 3y9m to 6y3m, found an average f0 of 297Hz, a value that falls within the normal range.
Gilbert and Campbell¹° upon studying a group of 62 hearing impaired children divided into 3 groups - aged 4 to 6 years, 8 to 10 years and 16 to 25 years, reported that fundamental frequencies for the boys were, respectively, 346, 306 and 142Hz, and for the girls, 300, 307 and 242Hz, and they did not find statistically significant differences between hearing impaired and normal hearing children. Tone variation was considered more restrictive and repetitive in the hearing impaired children.
Other authors consider vocal fundamental frequency of the hearing impaired higher than that of normal hearing subjects1,16,18. Angelocci et al.¹ evaluated 18 hearing impaired boys aged 11 to 14 years and compared them to normal hearing children. The fundamental frequency of the hearing impaired was 236Hz, significantly higher than that of the normal group, with an average of 193Hz. According to Nickerson18 hearing impaired children have modal frequency and intonation deviations. Frequency is higher and less stable, whereas inappropriate intonation characterizes monotonous voice or excessive and irregular frequency variations.
Pruszewics et al.²² investigated the characteristics of vocal disorders in 18 children with profound hearing loss divided into 3 groups, according to acquisition of loss: congenital, up to 3 years of age, and post-lingual. In the con genital group, there was great variability of fundamental frequency cycle by cycle and lack of control of intensity and frequency, a variability that was progressively reduced in the other groups.
Based on the general overview of the literature, and the importance of fundamental frequency and its variability in vocal quality definition, we investigated the effect of hearing impairment on vocal function and defined its deviation from normal range. Thus, the present study aimed at evaluating the fundamental frequency and its variability in the voices of children who had severe and profound sensorineural hearing impairment and compare with the mean values of normal hearing children.
MATERIAL AND METHOD
Sixty-four hearing impaired children took pant in this study, constituting the experimental group and 90 normal hearing children were the control group; they were all Brazilian and lived in the city of São Paulo, aged between 6 and 13 years, before adolescence vocal change.
Out of 64 hearing impaired children with pre-lingual severe and profound sensorineural loss, 33 were male (51.6%) and 31 were female (48.4%) subjects, all students of a special school. Based on the average of auditory thresholds of 0.5, 1 and 2KHz on the best ear, 18 children (28%) were classified as having severe hearing loss and 46 children (72%) as having profound hearing loss, according to Silman and Silverman24 criteria. We did not find the variables time of diagnosis of hearing loss, type of amplifications, use and maintenance of hearing aids, auditory thresholds with hearing aids and educational history.
Out of 90 children of the control group, 47 were male (52.2%) and 43 (47.8%) were female children, and they al had negative history of communication disorders and were students of regular schools.
The research protocol was previously analyzed and approved by the committee on ethics of the institution. Parents and responsible people were informed about the objective and the procedures involved in the study and signed an informed consent agreeing to participate.
Each subject was submitted to a recording of the voice producing the vowels a, i and u, sustained at habitual frequency and intensity. Recordings were made in a silent room, using unidirectional microphone brand Le Son model SM 58-BK, mounted in a pedestal and positioned at 45° from the mouth of individuals, using the digital recording system of Minidisk Sharp, model MD-MS702.
Recordings were submitted to acoustic and auditory perceptual analyses. To analyze acoustically, we used the software Dr. Speech, Tiger DRS, version 4.0, using the module Real Analysis. Acoustic parameters selected for the analysis were fundamental frequency (in Hertz), standard deviation of fundamental frequency (in Hertz), and range of fundamental frequency during sustained phonation (f0 range, in number of semitones).
Fundamental frequency (f0) is physiologically determined by the number of cycles that the vocal folds realize in one second. It is defined by the natural length of the fold, its elongation, the mass put to vibrate and the tension. It is affected by age and gender. In the Portuguese language spoken in Sao Paulo children have values above 250Hz, reaching 400Hz in babies2,4,5.
Fundamental frequency has a range that is expressed by the number of semitones (f0 range = f0 maximum - f0 minimum), or by applying a calculation of the index of the standard deviation of f0. In normal subjects, this range does not exceed 2Hz³.
For auditory perceptual analysis the recordings in minidisk of voice of hearing impaired and normal hearing children were initially transferred and edited randomly, in cassette tapes Sony, type II high bias UX. These recordings were presented to 14 voice specialists in order to identify the voice of a normal hearing or a hearing impaired child.
Statistical analysis of the study included the variables average of values of fundamental frequency, standard deviation of fundamental frequency and number of semitones of vowels "a", "i" and "u" and age, using the calculation of multiple linear regression (Neter, 1996), because of the wide variability of voice samples. The accordance among results of auditory perceptual analysis was also studied using the kappa statistical test (Agresti, 1990).
RESULTS
Results obtained in acoustic and auditory perceptual analyses of the voice of 64 hearing impaired children (33 male and 31 female children) and its comparison with the values obtained in normal hearing children (47 male and 43 female children), aged between (6 and 13 years, are shown in tables and graphs 1 to 3.
Table 1 and graphs 1 and 2 present the values obtained in models of multiple linear regression concerning the average of fundamental frequency and standard deviation of f0. Values of the model of multiple linear regression for number of semitones are found in Table 2 and graph 3.
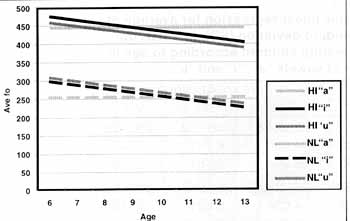
Graph 1. Values obtained in the model of multiple linear regression for average of fundamental frequency values (Ave Fo), in Hertz, according to age in years for hearing impaired and normal hearing children in the production of vowels "a", "i" and "u".
Results concerning auditory perceptual analysis are shown in Table 3.
DISCUSSION
The acoustic analysis of the voice in hearing impaired children showed marked deviations in the analyzed parameters, which has probably guided the identification of voices in the auditory perceptual evaluation made by the specialists.
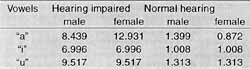
The literature presents controversial results when it comes to fundamental frequency in the hearing impaired children: some authors mention that the values are within normal ranges6,10,14,15,20,23,26.Our results were in accordance with the studies that obtained fundamental frequency values higher than the normal ranges1,16,18. The values of f0 found by us were significantly higher in hearing impaired children (Table 1), and some of the voices in the experimental group were much higher than those described in the literature. We found average values of 447.95 Hz for "a"; 475.97 to 404.78 Hz for "i"; 458.11 to 391.21 Hz for "u", values much higher than those obtained for normal hearing children: 256.24 Hz for "a"; 300.13 to 228.94 Hz for "i"; 308.12 to 241.22 Hz for "u" (Table 1).
The findings by Subtelny et al.25 and Ryalls and Larouche23 revealed that in the hearing impaired higher vowels present values of f0 higher than "a"; however, these findings were not confirmed in our study, because only in ages 6, 7 and 8 years vowel "i" was higher, and in ages 9, 10, 11, 12 and 13 years vowel "a' was the highest (Table 1).
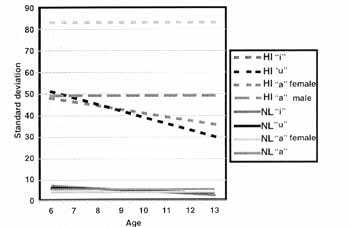
Graph 2. Values obtained in the model of multiple linear regression for standard deviation (SDfO), in Hertz, for hearing impaired and normal hearing children in the production of vowels "a", "i" and "u".
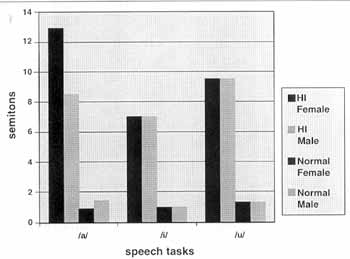
Graph 3. Values obtained in the model of multiple linear regression for number of semitones, in units, according to gender for hearing impaired and normal hearing children in the production of vowels "a", "i" and "u".
In the computer acoustic analysis of the voice of severe and profound hearing impaired children we observed that for the acoustic parameter average of values of fundamental frequency gender was not a significant variable, and children's gender could be identified based on the value of f0. As to age, we observed a gradual reduction of values of f0 as a result of older age in productions of 'i" and "u"; this is physiologically expected by the maturational process of the phonation system. The same reduction was not obtained for vowel "a', demonstrating that it is not sensitive to age range (Graph 1).
TABLE 1 - Values obtained from the model of multiple linear regression for average of fundamental frequency (Ave fo) and standard deviation (SD), in Hertz, obtained in hearing impaired and normal hearing children according to age in years and gender, for emission of vowels "a", "i" and u".
Horii¹¹, upon studying adolescent women found a production of elevated fundamental frequency in the hearing impaired when compared to the normal hearing, referring that the natural reduction of f0 did not occur in the analyzed group. In our study, we observed a reduction of f0 up to the age of 13 years; however, even when reduced, these values were significantly higher than those for normal hearing subjects.
Malmberg¹² explained that the prevalence of high values of fundamental frequency occurs because the sensation of intensity is directly proportional to the potency of 2 of the variation of the frequency of a sound. Therefore, elevated f0 would be a mechanism that the hearing impaired children used to amplify the auditory sensation and, consequently auditory monitoring, facilitating detection of their own voice, even in the presence of little intelligible pattern.
The use of a high fundamental frequency reflects poor laryngeal control, translated by laryngeal elevation and more phonation effort, inability to control tension of the vocal folds and subglottic pressure, as highlighted by many authors7,9,11,15,16,17,19,21,25.
According to a number of authors1,13,16,18,22 the hearing impaired children have excessive variation of fundamental frequency, compatible with the findings in our study (Table 2). The hearing impaired children present a wide range of fundamental frequency, revealed by increased values of standard deviation and number of semitones. According to Monsen14, this variation of fundamental frequency has correlation with vocal quality, resulting in differentiation between good and bad speakers.TABLE 2 - Values obtained from the model of multiple linear regression for number of semitones, in units, obtained in hearing impaired and normal hearing children according to gender, for emission of vowels "a", "i" and "u".
As to standard deviation of f0 in vowels "i" and "u" in both groups (hearing impaired and normal hearing children), gender was not relevant; however, there was reduction of values as a result of age, meaning that more laryngeal stability was acquired by the older children (Table 1 and Graph 2). As to vowel "a", we observed that only the variable gender was significant: hearing impaired girls had higher values than boys, revealing more instability during sustained phonation (Table 1 and Graph 2). Values found in hearing impaired children were extremely higher than those of normal hearing subjects.
Another variable that showed great instability of fundamental frequency was the number of semitones during sustained vowels. In Table 2 we could observe that age was not a significant factor; however, as to gender, we observed a larger number of semitones in hearing impaired girls during production of "a", correlating with the high value of standard deviation. Hearing impaired children had an extremely high value of semitones when compared to the normal hearing. Graph 3 clearly shows these elevated figures obtained for the hearing impaired children.
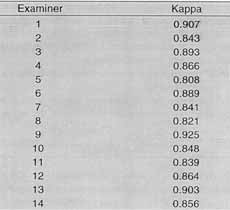
In addition to acoustic assessment, whose data we have already commented, we conducted also an auditory perceptual analysis of voices of children enrolled in the study to check if deviations that we expected to find were important markers of these children's voices. According to the statistical test of kappa (Table 3), we noticed high concordance between the examiners who had to identify the voices as belonging to a hearing impaired or a normal hearing child (between 0.808 and 0.907), which had been previously mentioned by Thomas-Kersting and Casteel 27.Therefore, our data indicated that trained listeners - speech pathologists, clearly identified voices of hearing impaired children.. Calvert8 highlighted that hearing impaired children could not be identified only by vowels, requiring sentences to promote more precise identification, which goes against our findings that the hearing, impaired children were easily identified based on their vocal markers in the production of vowels.TABLE 3 - Values of agreement in Kappa test for normal hearing and hearing impaired children.
Probably the variables that were not controlled, either in this and in other studies described by the literature, as well as methodological issues, are responsible for the differences in results. Due to diversity of aspects related to hearing impairment, such as nature and degree of loss, age, amplification and type of rehabilitation, maybe we will never have objective parameters defined as universal basis. Nevertheless, the presented deviations are evident.
This study demonstrated, by means of acoustic and auditory perceptual analysis in the production of sustained vowels in the hearing impaired, that they have a phonation pattern deviated from the patterns expected for age and gender, facilitating their immediate recognition. It reinforced the idea that voice in the hearing impaired should be specifically addressed in order to minimize the impact of hearing impairment in oral communication and contribute to social integration.
CONCLUSION
Based on the comparative study of vocal acoustic parameters in 64 children who had pre-lingual severe and profound sensorineural hearing impairment and 90 children without history of communication disorders, aged between 6 and 13 years, we concluded that the voice in the hearing impaired children is characterized by:
o Use of very high fundamental frequency, reflecting very poor laryngeal control.
o Presence of excessive fundamental frequency range in sustained emission, revealing the instability of the whole system.
REFERENCES
1. ANGELOCCI, A.; KOPP, G.; HOLBROOK, A. - The vowel formants of deaf and normal-hearing eleven-to fourteen-year old boys. J. Speech. Hear. Disord., 29: 156-170, 1964.
2. BEHLAU, M. S. - Estudo das vogais do português brasileiro falado em São Paulo: perceptual, espectrográfica de formantes e computadorizada de freqüência fundamental. São Paulo, 1984. Dissertação (Mestrado) - Escola Paulista de Medicina.
3. BEHLAU, M. S.; MADAZIO, G & PONTES, P. A- Avaliação de Voz. São Paulo, editora CEV, 2000. /apostila 3/.
4. BEHLAU, M. S. & PONTES, P. A. - Avaliação e Tratamento das Disfonias. São Paulo, editora Lovise, 1995.
5. BEHLAU, M. S.; TOSI, O & PONTES, P. A. - Determinação da freqüência fundamental a suas variações em altura (jitter) e intensidade (shimmer), para falantes do português brasileiro. Acta AWHO, 4: 5-9, 1985.
6. BOONE, D. R. - Modification of the voices, of deaf children. Volta Rev., 68: 686-92, 1966.
7. BORGES, R.H.M. - Avaliação de voz em deficientes auditivos: uma analise critica. In: FERREIRA, L.P. - Dissertando sobre a voz. São Paulo, Pró-Fono, 1998. p150-71. (Série Interfaces- vol.2).
8. CALVERT, D. R. - Deaf voice quality: a preliminary investigation. Volta Rev., 64: 402-3, 1962.
9. FORNER, L.L. & HIXON, T J. - Respiratory kinematics in profoundly hearing-impaired speakers. J Speech Hear. Res., 20: 373-408, 1997.
10. GILBERT, H. & CAMPBELL, M. - Speaking fundamental frequency in three
groups of hearing-impaired individuals. J. Commun. Disord., 13:195-205,1980.
11. HORII, Y. - Some voice fundamental frequency characteristics of oral reading and spontaneous speech by hard of hearing young women. J Speech. Hear. Res., 25: 608-10, 1982.
12. MALMBERG, B. - A fonética: no mundo dos sons da linguagem. Lisboa, Livros do Brasil, 1954. 195p (Coleção Vida e Cultura).
13. MONSEN, R. B. - Toward measuring how well hearing- impaired children speak. J. Speech. Hear. Res., 21 (2): 197-219, 1978.
14. MONSEN, R. B. - Acoustic qualities of phonation in young hearing-impaired children. J. Speech. Hear. Res., 22: 270-88, 1979.
15. MONSEN, R. B.; ENGEBRETSON, A. M.; VEMULA, N. R. Some effects of deafness on the generation of voice. J. Acoust. Soc. Am., 66 (6): 1680-90, 1979.
16. MONSEN, R. B. - Voice quality and speech intelligibility among deaf children. Am. Ann. Deaf., 128 (1):12-19, 1983a.
17. MONSEN, R. B. - The oral speech intelligibility of hearing-impaired talkers. J. Speech. Hear. Disord., 48: 286-96,1983b.
18. NICKERSON, R. S. - Characteristics of speech of deaf persons. Volta Rev. 77, 342-362, 1975.
19. OSBERGER, M. J. & HESKETH, L. J. - Speech and language disorders related to hearing impairment. In: LASS, N. J.; MCREYNOLDS, L.V.; NORTHERN, J. L. & YODER, D. E. Handbook of Speech-Language Pathology and Audiology. Toronto, B.C. .Decker Inc, 1988, p 858-867.
20. OSBERGER, M. J. & MCGARR, N. - Speech production characteristics of the hearing impaired. In: LASS, N.J, - Speech and language: Advances in basic research and practice. New York. Academic Press, 1982, vol.8, p 221-283.
21. PRINZ, P.M. - Desenvolvimento da comunicação e linguagem: avaliação a conduta em indivíduos com deficiência auditiva. In: KATZ, J.- Tratado de Audiologia Clinica. 3.ed. São Paulo, Manole, 1989. p.798-820.
22. PRUSZEWICS, A.; DEMENKO, G. & WIKA, T. - Variability analysis of Fo parameter in the voice of individuals with hearing disturbances. Acta Otolaryngol (Stockh), 113(3): 450-4, 1993.
23. RYALLS, J. & LAROUCHE, A. - Acoustic integrity of speech production in children with moderate and severe hearing impairment. J. Speech. Hear. Res., 35: 88-95, 1992.
24. SILMAN, S. & SILVERMAN, C. A. - Auditory Diagnosis, San Diego. Academic Press Inc., 1991.
25. SUBTELNY, J.D.; WHITEHEAD, R.L. & ORLANDO, N.A. Description and evaluation of an instructional program to improve speech and voice diagnosis of the hearing impaired. Volta Rev.,: 85-95, 1980.
26. SUBTELNY, J. D.; WHITEHEAD, R. L. & SAMAR, V. J. Spectral study of deviant resonance in speech of women who are deaf. J. Speech. Hear. Res., 35(3): 574-9, 1992.
27. THOMAS-KERSTING, C.; CASTEEL, R. L. - Harsh voice: vocal effort perceptual ratings and spectral noise levels of hearing-impaired children. J. Commun. Disord., 22(2): 125-35, 1989.
* Speech and Hearing Pathologist, Specialist in Voice.
* Ph.D., Speech and Hearing Pathologist, Specialist in Voice, Technical and Scientific Coordinator of the Specialization Course on Voice at Centro de Estudos da Voz - CECEV, São Paulo /SP.
*** Ph.D., Professor and Head of the Clinic of the Department of Otorhinolaryngology at Santa Casa de São Paulo.
Study conducted at Centro de Estudos da Voz - CEV, São Paulo /SP.
Study presented at 35° Congresso Brasileiro de Otorrinolaringologia, which was awarded a special citation.
Address for correspondence: Maria do Carmo Giusti - Rua dos Bandeirantes, 98 - Bom Retiro - 01124-010 São Paulo /SP - Tel: (55 11) 229-7533.
E-mail: mamogiusti@uol.com.br
Article submitted on August 15, 2000. Article accepted on October 20, 2000.
Print: ![]()