

Year: 2000 Vol. 66 Ed. 5 - (13º)
Artigos Originais
Pages: 507 to 510
Pre and Post-Operative Conditions of Patients Who Underwent Laryngeal Microsurgery for the Main Benign Lesions.
Author(s):
Paulo S. L. Perazzo*,
Alex C. Cota***,
Milton P. C. Moura***,
Washington L. C. Almeida**,
Carlos R. T. Gois***.
Keywords: lesions, benigns, larynx
Abstract:
Introduction: Benign lesions of larynx, although they are not considered serious pathologies, require proper diagnosis and treatment due to their impact on the voice. This study aims at analysing statistically main benign pathologies of larynx and the functional result of pacients submitted to surgical treatment. Material and method: this study was carried out with a group of 40 pacients, aged between three and 62, with record of chronical disphony. They were submitted to routine ORL test and to complementary videolaringoestroboscopy in pre-and post-operating phases. Result: Female sex predominated, being age group 31 to 40 most affected. Hoarseness was the most frequent symptom and cyst the lesion which happened most. In 15% of the cases, larynx microsurgery helped explain or change diagnosis.
![]()
INTRODUCTION
Despite the fact that they are not nosological entities of major severity, laryngeal benign lesions impact dramatically the voice of patients. Therefore, correct diagnosis is essential, followed by appropriate treatment. This is due not only to the pathological condition per se, but also because surgery may cause dysphonia3.
Among laryngeal benign lesions, we may point out nodules, epidermoid and retention cysts, sulcus vocalis, polyps, Reinke's edema, vascular dysgenesis, microwebs, granuloma and papilloma. Although etiology and initial treatment may differ, they may all follow general procedures4. Surgical procedures, in such cases, aim at improving glottic closure and eliminating factors that interfere in normal vibration of vocal folds.
The objective of the present study was to analyze statistically the main laryngeal benign lesions and functional result of patients submitted to surgical treatment.
MATERIAL AND METHOD
Forty patients were analyzed; they all had chronic dysphonia and ranged in age from 3 to 62 years (mean of 32.5 years), divided into 12 male and 28 female subjects.
They were submitted to routine otorhinolaryngologic exam, according to a standardized protocol. In addition, they underwent complementary assessment with videolaryngostroboscope Kay RLS 9100, pre and post-operatively, since videolaryngostroboscopy is the main instrument for correct diagnosis and indication of laryngeal microsurgery, providing the exact extension of the lesion and its influence on the vocal fold vibration and glottic closure9.
Surgical treatment was defended in cases in which it was indispensable for patients' improvement, or when after performance of voice therapy, there was persistence or recurrence of lesion1. We conducted all surgeries under general anesthesia with endotracheal tube with cuff, because it provided safety and convenience to the surgeon, lying on posterior commissure, far from the membranous portion of the vocal folds, where the surgical procedure is actually conducted4.
Visualization of vocal folds during surgery was guaranteed by suspension laryngoscope and microscope of Katz, using 300mm lenses augmenting 16 or 24 times. In addition, we used rigid endoscope at the beginning of the surgery because it provided a tridimensional view of the lesion and related structures, making it easier to define where to make the incision and avoiding cutting over the lesion14.
In case of nodules, polyps and granulomas, we captured them with microforceps, followed by exeresis with microscissors, preserving normal mucosa4,13. As to cysts, we used lateral or medial microflap technique, with. dissection of pathological tissue from healthy tissue, trying to preserve as much as possible the mucosa of the free margin and vocal ligament, and infiltration of intra-chordal corticoid (0.5 ml of hydrocortisone 100mg), aiming at reducing local inflammatory reactions. In some cases, we used biological glue4. In such cases, we observed better recovery of tissues, presenting normal appearance vocal folds in shorter time.
As to papilloma, we performed exeresis of lesions with Allis clamp trying to preserve mucosa as much as possible. For the treatment of sulcus vocalis, we carefully detached atrophic mucosa from vocal ligament, followed by harvest of fat graft (from abdominal region or earlobe) and placement of graft on thyroarytenoid muscle after opening of a pocket5.
When the clinical pathology was Reinke's edema, we aspired the jelly contents from Reinke's space (superficial layer of lamina propria) and carefully removed excessive mucosa. In some cases, we used biological glue to reposition a flap or to recover areas of resection.
In all surgical procedures in which we removed tissue fragments, they were submitted to anatomical pathological analysis13.
If there was vascular dysgenesis associated with any other laryngeal benign lesion, we performed electrocauterization using Bouchayer's cautery and minimum intensity, in order to interrupt blood flow and to reduce mucosa deformity6,12. After the surgery, patients were instructed to remain in absolute vocal rest for 7 to 9 days, until the first post-op follow-up4,13. Between 151 and 2011 post-op days, patients were re-evaluated to define complementation with voice therapy11.
RESULTS AND DISCUSSION
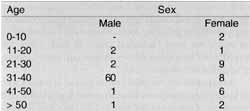
Out of 40 patients, we observed a predominance of female subjects (28 cases), and the most affected age range was between 31 and 40 years (14 cases) (Table 1).
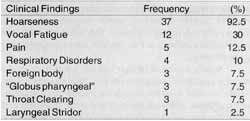
There were various symptoms associated with patients who had laryngeal benign lesions, but hoarseness was present in 37 subjects (92.5% of cases). Other important complaints were vocal fatigue (30%), pain (12.5%), respiratory disorders (10 %), sensation of foreign body (7.5%), "laryngeal globus" (7.5%), throat clearing (7.5%) and laryngeal stridor (2.5%) (Table 2).
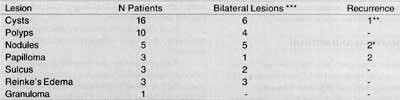
Cysts were the most incident lesions in our study (16 patients). Out of these, one presented post-op recurrence. Six cases included bilateral lesions or contralateral reaction. Polyps were present in 10 patients, whereas nodules, always bilateral by definition11, were present in 5 cases. In two cases there was recurrence after voice therapy, indicating surgical removal (Table 3).
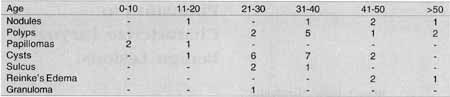
In Table 4 we can observe that, except for papillomas, a recurrent and typical lesion in children, all laryngeal benign lesions predominate in the age range 21 to 50 years of age, compatible with the data in the literature, because this is the phase in life in which subjects have higher occupational production and increase vocal demand4,12,13. It is interesting to point out that patients with Reinke's edema are usually older than patients with other pathologies; it may be explained by the fact that it takes time for vocal fold tobacco-related lesions to manifest13.TABLE 1 - Age/Sex.
TABLE 2 - Distribution of frequency and percentage of the main symptoms.
TABLE 3 - Incidence of benign laryngeal lesions.
* Post-voice therapy ** Post-surgery *** Includes contralateral reactions
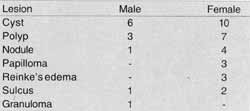
Analyzing Table 15, we could notice that excluding granuloma (only one case in the male group), all lesions present were predominant in the female group. Most of the studies observed also that there is an absolute predominance of nodules and Reinke's edema in women1,4,13. As to Reinke's edema, this discrepancy is probably due to women's concerns about vocal harshness caused by the lesion, motivating them to search more frequently for medical assistance. Similarly to the literature that confirms Reinke's edema as a common pathology among smokers2, the three patients who had the pathology were regular smokers. On the other hand, most studies show that polyps are more frequent among men8,13; however, in the present study, the pathology was predominant in women (70% of the cases). In the 3 cases of vergeture sulcus vocalis, surgery aimed at reducing vocal fatigue, vocal harshness and breathiness4,10,12.
In 6 cases (15%) laryngeal microsurgery helped clarify or modify pre-op diagnosis. The same was observed by various authors4,12,13, showing that regardless of diagnostic measures now available for visualization of vocal folds, palpating them is sometimes essential for diagnostic definition.
CONCLUSION
1. The highest incidence of laryngeal benign lesions was between 31 and 40 years.
2. Female subjects were more affected.
3. Hoarseness was the most frequent symptom.
4. Cyst was the most common benign lesion.
5. Surgical techniques used showed excellent results; except for sulcus vocalis, whose results were fair.
6. Post-op vocal therapy was essential in all cases; presurgically, it was used only in cases of nodules (5 patients), but all patients were submitted to vocal assessment.
7. We realized the need for objective voice assessment (Voice Lab) to control surgical treatment and post-op results, aiming at obtaining a more reliable measure of post-surgical improvement.TABLE 4 - Distribution of lesion according to age.
TABLE 5 - Distribution of laryngeal lesions according to sex.
REFERENCES
1. BENNINGER, M. S.; JACOBSON, B. -Vocal Nodules, Microwebs, and Surgery. Journal of Voice. 1985; vol. 9: 326-331.
2. BETLEJEWSKI, S.; SINKIEWCZ, A.; OWCZAREK; A.; SWIDZINSKI, P. - Functional Voice Evaluation After Reinke's Edema Treated With CO2 Laser and Kleinsasser's Microsurgery. Otolaryngol Pol. (POLAND). 1987; 51 Suppl 25:116-20.
3. BOUCHAYER, M.; CORNUT, G.; LOIRE, R.; ROCHE, J. B.; WITZIG, E.; BASTIAN, R.W. - Epidermoid cysts, sulci and mucosal bridges o f the true vocal cord; a report of 157 cases. Laryngoscope 1985; 95: 1087-94.
4. BOUCHAYER, M.; CORNUT, G. - Microsurgery for Benign Lesions of The Vocal Folds. Ear Nose Throat J. 1988; 67: 446467.
5. BRANDENBURG, J. HUNGER, J. M.; KOSCHKEE, D. - Vocal Cord Injection With Autogenous Fat: A Long-term Magnetic Resonance Imaging Evaluation. Laryngoscope 1996; 106: 174-180.
6. HOCHMAN, I.; SATALOFF, R. T.; HILLMAN, R. E.; ZEITELS, S. M. - Ann Otol Rhinol Laryngol. 1999; 108(1): 10-6.
7. JURKIEWICZ, D.; LIGEZINSKI, A.; KUZME, W. - Laser Surgery and Interferon in The Treatment of Laryngeal Papilloma. Otolaryngol Pol. 1997; 51 Suppl 25 :134-8
8. KLEINSASSER, O. - Pathogenesis of Vocal Cord Polyps. Ann Otol Rhinol Laryngol. 1982; 91: 378-81.
9. MAHIEU, H. F.; DIKKERS, F., G. - Indirect Microlaryngostroboscopic Surgery. Arcb Otolaryngol. Head Neck Surg. 1992; 118: 21-24.
10. MILUTINOVIC, Z. - Critical Review of Phonosurgical Methods in The Treatment of Sulcus Vocalis. Srp Arh Celok LeK (YUGOSLAVIA). 1998; 126(11-12): 495-8.
11. MILUTINOVIC, Z. -Phonosurgical Therapy of Nodular Lesions of The Vocal Cords. Srp Arh Celok LeK (YUGOSLAVIA). 1998; 126(7-8): 248-52.
12. PONTES, P.; BEHLAU, M.; GONQALVES, I. - Alterações Estruturais Mínimas da Laringe (AEM): Considerações Básicas. Acta Awho. 1994; 8(1): 2-6.
13. REMACLE, M.; LAWSON, G.; WATELETJ. B. - Carbon Dioxide Laser Microsurgery of Benign Vocal Fold Lesions: Indications, Techniques, and Results in 251 Patients. Ann Otol Rhinol Laryngol. 1999; 108: 156-164.
14. YEH, A. R.; HUANG, H. M.; CHEN, Y. L. -Telescopic Video Microlaryngeal Surgery. Ann OtolRbinolLaryngol.1999; 108:165-8. 1
* Professor of Speech and Hearing Pathology at Uneb and Otorhinolaryngologist with Clínica Otorrinos.
** Doctorate studies in Otorhinolaryngology under course at USP and Otorhinolaryngologist with Clínica Otorrinos.
*** Otorhinolaryngologist with Clínica Otorrinos.
**** Resident Physician in Otorhinolaryngology at Clínica Otorrinos.
Study presented at 340 Congresso Brasileiro de Otorrinolaringologia, November 18 - 22, 1998, in Porto Alegre/ RS.
Study conducted at Clínica Otorrinos.
Address for correspondence: Rua Bardo de Cotegipe, 1141 - Centro - 44025-030 Feira de Santana/ BA - Brazil - Tel: (55 75) 623-4455 - Fax: (55 75) 223-4117.
E-mail: otorrinos@gd.com.br
Article submitted on June 30, 2000. Article accepted on August 17, 2000.
Print: ![]()