

Year: 2000 Vol. 66 Ed. 5 - (10º)
Artigos Originais
Pages: 486 to 492
Congenital and Adquired Deafness in Childhood.
Author(s):
Adriana S. Lima*,
Ana M. M. Salles**,
Alfredo P. Barreto***.
Keywords: deafness, childhood deafness
Abstract:
Introduction: The childhood deafness constitutes a serious social medical problem which impairs both communication and learning abilities, reflecting many times on a poor social interaction of the child. Purposes: The purposes of this work are: to demonstrate the difficulty of providing patients with a precise etiologic diagnosis, the importance of preventing the available deafness and that of the early diagnosis for the childhood deafness. Material and method: This research has been developed at Felipe Smaldone Institute (a speciality school to teach children deafness) from Belém /PA, in the period within December 1996 and February 1997. Meanwhile,150 children from both sexes between the ages of 3 and 13 years have been registered, giving importance mainly to the possible causes for the childhood deafness and relating the type and degree of deafness. Results: The result showed predomination of those causes which are available, such as: congenit rubeolla (32 cases 22%), meningitis (20 cases - 13%), and the use of ototoxis drugs (14 cases - 9%). Conclusion: It's important to emphasize the large number of cases whose origins remain unidentified due to lack of information or patents' omission which accounts for the difficulty in obtaining a precise etiological diagnosis and thus still defying otorhynolaringologists.
![]()
INTRODUCTION
Hearing loss may be defined as a sign or symptom resulting from one or more damaging factors to the hearing organ22. It may be classified based on topographic location in conductive, sensorineural and mixed, and according to clinical expression in hearing loss, deafness and anacusia2,11,14.
Sensorineural hearing loss, highlighted in the present study, involves sensorial lesions, that it, lesions affecting Corti's organ and inner ear and neural lesions that affect the cochlear nerve up to the auditory nuclei on the brainstem. Its main characteristic is high frequencies hearing loss with or without preservation of low frequencies11,14,19.
According to Bureau International D'Audiophonoiogie (BIAP), hearing loss is classified as mild (20 to 40 dBHL), moderate (40 to 70 dBHL), severe (70 to 90 dBHL) and profound (more than 90 dBHL). The normal threshold is up to 20 dBHL27, although some other institutions, such as The Americana Association of Otorhinolaryngology and Ophthalmology (AAOO) consider up to the threshold of 25 dBHL.
Many studies from Brazil and around the world4,5,9,22,23 have tried to reliably demonstrate the prevalence and incidence of hearing loss in childhood. There are major difficulties associated with the production of precise figures, especially in developing countries. It is due to the fact that there are great epidemiological differences among inhabitants of different countries and sometimes regions of a same country5,12,22.
Despite these differences, general prevalence of hearing loss in childhood is estimated in 1.5/1,000, ranging from 0.8 to 2/1,000 in different areas of the industrialized world9,22. Among children with hearing disabilities, 90% have sensorineural loss, 5%, conductive and 5%, mixed22.
The estimated number of children with congenital hearing loss (present at birth or acquired during neonatal period) should be considered at least of 1.3/1,000, because of late identification, which may affect epidemiological data22.
Owing to the physiopathologic complexity of hearing, it is easy to conclude that deafness may originate from different pathologies. Hearing impairment in children may come from a genetic origin, or be acquired during pre, peri or post-natal periods3,4,11,15,1,7,22,23,31,33.
Heredity is described in the literature as an important cause of deafness, and it may be the only genetic disorder inherit or it may be part of a set of anomalies comprising a syndrome14,16,17,22,23,26,27.
Infections that affect mothers during gestation, or prenatal period, causing damage to fetus, such as rubella, toxoplasmosis, cytomegalovirus, syphilis, parotiditis, caused by simple herpes, and also the use of abortion drugs, are causes of hearing loss in children and should always be investigated during the study of etiology1,3,4,5,8,11,12,14,16,18,22,23,24,26,27,29,32,33.
Peri-natal period comprises the birth until the 8th week after delivery and during this period many factors may permanently affect the hearing mechanism of a child. Some examples are neonatal hypoxia, pre-term delivery, post-term delivery, hyperbilirubinemia, birth traumas, use of ototoxic medication, and exposure to noise of isolette in intensive care units3,4,5,8,11,12,14,16,17,18,19,22,23,26,27,28,31,32,33. They amount to 10 to 13% of hearing loss in children22.
As to post-natal affections, after the 8th week post-delivery, the most frequent causes are otitis media and its complications, measles, mumps, bacterial meningitis, encephalitis, ototoxic drugs, cranioencephalic traumas, acoustic traumas, diabetes mellitus, auto-immune diseases, otosclerosis and auditory nerve tumors. In this period, the use of ototoxic drugs and bacterial meningitis are extremely important because their incidence levels vary from 6 to 11.8%3,8,11,12,17,18,22,28,32.
Many etiologies may be the cause of hearing loss in children. However, about 20 to 40% of the cases are of unknown origin4,5,8,12,18,22,27,28,32.
Hearing evaluation in children is a challenge and special methods are used, different from those normally employed with adults, because of language absence or delay7,23, 34.
The choice of method to determine hearing levels depends on age of child, although symptoms (absence of response to auditory stimulus, delay in language acquisition, uncontrolled cry and poor school performance) are similar in most age ranges7.
In order to facilitate early diagnosis of hearing loss in childhood, the joint Committee on infant Hearing established seven internationally recognized criteria for high risk of hearing loss. They are: family history of hearing loss, intra-uterus or peri-natal infection (toxoplasmosis, cytomegalovirus, syphilis, rubella, herpes), head and neck malformations, neonate with weight at birth below 1,500g, severe neonatal hyperbilirubinemia, bacterial meningitis especially caused by Haemophilus influenzae, and severe hypoxia at birth1,22.
This study, restricted to a group of children from Instituto Felipe Smaldone, intended to investigate the main causes, type and level of hearing loss. The objective was to show the difficulties we face in determining precise etiology of cases and the importance of preventing avoidable cases of hearing loss and of early detection of hearing loss in children.
MATERIAL AND METHOD
Instituto Felipe Smaldone is an Italian school in Brazil specialized in educating hearing impaired children. There, children are submitted to a detailed hearing screening conducted by the departments of audiology, pediatrics, psychology, pedagogy and speech therapy. Only children who have deafness without associated deficiencies are accepted, as well as children until the age of 4 years.
The present study was conducted in this institution, located in Belem do Para, between December 1996 and February 97, when 150 children, both sexes, ranging in ages from 2 to 13 years were analyzed.
We analyzed the school files using questionnaires that had detailed anamnesis and results from complementary tests such as child conditioned audiometry, and brainstem evoked response audiometry (ABR), and we looked for the possible causes and the level of hearing loss.
As to etiological diagnosis, we valued data from family history of hearing loss, affections during pre, peri, and post-natal periods, such as the use of abortion drugs, ototoxic antibiotics, neonatal anoxia, and other similar situations, in order to produce a reliable study.
RESULTS
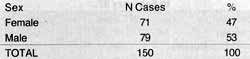
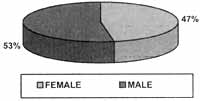
We observed a slight predominance of male subjects. Male patients amounted to 79 cases, corresponding to 53% of the total, whereas there were 71 female cases, amounting to 47% (Table 1 and Figure 1).
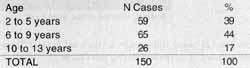
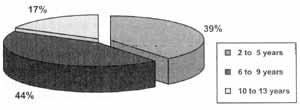
We noticed that between the ages of 6 and 9 years there were 44% of the cases (Table 2 and Figure 2).
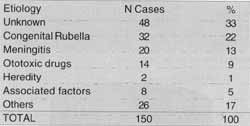
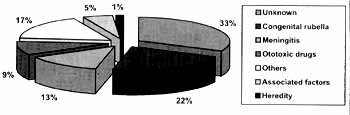
Congenital rubella (32 cases-22%) was the main identifiable cause, followed by meningitis (20 cases-13%o) and use of ototoxic drugs (14 cases-9%). We should also point out that there was a large percentage of cases in which the hearing loss was of unknown origin. (48 cases-33%) (Table 3 and Figure 3).
Under the designation "others" (26 cases-17%), we included other possible causes that may lead to hearing loss, such as the use of abortion drugs (12 cases), neonatal anoxia (10 cases), pre-term delivery (1 case), cranioencephalic traumatism (1 case) and pre-natal infections such as measles and syphilis (1 case each).
As to associated risk factors, we observed the conjunction of up to 3 factors that would imply significant hearing deficit, such as combination of pre-term delivery and use of ototoxic drugs (2 cases) and varicella during gestation and use of abortion drugs (2 cases). Moreover, there were cases of use of ototoxic drugs, use of abortion drugs and pre-term delivery, birth traumatism, pre-term delivery and neonatal anoxia; neonatal anoxia and ototoxic drugs, and neonatal anoxia and post-term delivery (Table 4).
All studied children (150 children) had sensorineural hearing loss.
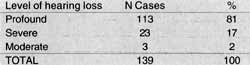
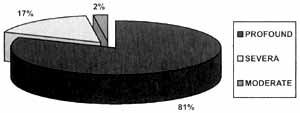
Profound hearing loss was the most frequent, amounting to 113 cases out of 139 cases of symmetrical hearing loss (Table 5 and Figure 4).TABLE 1 - Distribution of cases and sex. Instituto Felipe Smaldone, December 96 to February 97.
Source: Instituto Felipe Smaldone.
Figure 1. Distribution of cases and sex. Instituto Felipe Smaldone, December 96 to February 97.
TABLE 2 - Distribution of cases and age. Instituto Feline Smaldone. December 96 to February 97.
Source: Instituto Felipe Smaldone.
Figure 2. Distribution of cases and age. Instituto Felipe Smaldone December 96 to February 97.
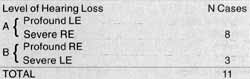
When analyzing the data concerning level of hearing loss, we observed 11 cases with asymmetrical hearing loss (Table 6).
Profound hearing loss was predominant in all analyzed causes (Table 7).
In most cases, congenital rubella corresponded to profound loss (26 cases), followed by severe loss (2 cases). There were no cases of moderate hearing loss (Table 7).TABLE 3 - distribution of cases and etiology of hearing loss. Instituto Felipe Smaldone, December 96 to February 97.
Source: Instituto Felipe Smaldoned
Figure 3. Distribution of etiology of hearing loss: Instituto Felipe Smaldone, December 96 to February 97.
TABLE 4 - Distribution of cases and associated risk factors. Instituto Felipe Smaldone, December 96 to February 97.
Source: Instituto Felipe Smaldone.
DISCUSSION
Etiological diagnosis of hearing loss in children is a difficult task to accomplish; because of that, cases of unknown origin take a key role in the statistics of various scientific studies5,8,12,26,27,28,32, which also happened in the present study. Various factors are responsible for this fact, such as the difficulty to obtain correct data when interviewing the parents and family members, the fact that people do not know the manifestations of viruses during gestation, obstacles to the conduction of a good pre-natal follow-up, and delay in detection of hearing loss, which normally takes place in the 2nd year of life3,5,12,22,25,26,33.
According to the investigation we proceeded, we found that congenital rubella is still the main identifiable cause of hearing loss in childhood, followed by meningitis and use of ototoxic drugs, especially aminoglycoside antibiotics.
In our study, rubella was considered as possible etiology in 22% of the cases, a percentage close to that reported by other studies3,6,28,32.
Congenital rubella caused bilateral and symmetrical sensorineural hearing loss. Profound loss is predominant, followed by severe loss, as widely described by the literature1,3,6,18,24,27 and confirmed by the present study.
Heredity, as consanguinity, is an important cause of hearing loss. There are some regions in the world where marriage among cousins and other, relatives is part of the culture. In Brazil, especially in small towns of Goias and Minas Gerais states and in the Northeastern region, this fact is also extremely common. In such societies, inherit deafness will be much more frequent17,17.
Our study found only 2 cases (1%) of hearing loss because of consanguinity, different from the literature, in which it has a dominant position10,22,26,27. It suggests that in the studied group the incidence of consanguineous marriages was low. We did not observe syndromic cases in our study either.
In post-natal phase, the most frequent risk factors are meningitis and use of ototoxic drugs.
In the present study, meningitis was the second most frequent cause after rubella, amounting to 13% of the causes, a parameter similar to those of other studies5,12. We should always keep in mind that hearing loss is the most common neurological sequela after meningitis, justifying the importance of early hearing tests.after the disease10,17,23.TABLE 5 - Distribution of cases according to level of hearing loss. Instituto Felipe Smaldone, December 96 to February 97.
Source: Instituto Felipe Smaldone
Figure 4. Distribution of cases and level of hearing loss. Instituto Felipe Smaldone, December 96 to February 97.
The abusive use of ototoxic drugs continues to cause sensorineural deafness in expressive indexes5,12,26,28,32, as reveled by most of the researches, including this one. We may point out the excessive and indiscriminate use of aminoglycoside antibiotics in children, part of the routine of bronchopneumonia and enterocolitis treatment, and in some simple cases of upper airway affections. Other antibiotics could equally solve the problem without adding hearing risks27.
Undoubtedly, early diagnosis of hearing loss experienced a major advance thanks to the development of brainstem evoked response audiometry. However, there are still professionals who do not know or do not value properly the criteria adopted for risk factors during gestation and in neonates of hearing loss in children1,3,22.
Finally, there are no studies in the literature that confirm the predominance of hearing loss in male subjects. There are many studies, however, that point out such a tendency5,18,26,27,28,32, a similar conclusion to the one we came to in the present study.
CONCLUSION
Because of difficulties in collecting precise data when interviewing parents and/or family members, we suggest the creation of a more detailed and standardized questionnaire that could he applied in different institutions that deal with the problem, in order to reduce the number of cases recorded as of unknown etiology.TABLE 6 - Distribution of cases of asymmetry and level of hearing loss (Groups A and B). Instituto Felipe Smaldone. December 96 to February 97.
RE = right ear.
LE = left ear.
Source: Instituto Felipe Smaldone.
The predominance of cases with preventable etiologies, such as rubella, meningitis and use of ototoxic drugs, is evident. Therefore, we suggest the introduction of a regular program of rubella vaccination in Brazil especially in childbearing age women. In addition, better medical and sanitary conditions and preventive treatment through immunization would reduce the number of cases of meningitis and avoid possible sequelae.
The amount of drugs known to be ototoxic and still used in children was really astonishing. It shows the need for providing more information for professionals who treat children, clarifying issues regarding the problems of excessive use of these medications and its consequences.
Health care professionals should struggle to detect early hearing losses in children, enabling proper habilitation with hearing aids and speech therapy, reducing the risks of linguistic, educational and psychosocial impairments that may be caused by hearing loss.
TABLE 7 - Relation between etiology and level of deafness. Instituto Felipe Smaldone, December 96 to February 97.
Source: Instituto Felipe Smaldone.
REFERENCES
1. AZEVEDO, M. F. et al. - Rubéola congênita: caracterização dos aspectos clínicos a audiológicos. Acta Awho, 8(3), p97-104, set./ dez. 1989.
2. BALLANTYNE, J. - Surdez: Tipos a características clinicas. In: Surdez. 5.ed. Porto Alegre: Artes Médicas,1995. 312p. p.62-63. 3. BENTO, R. F. et al. - Etiologia da deficiência auditiva: estudo eletrofisiológico de 136 cases. Folha Médica, 93 (516), p:359-366, nov./dez. 1986.
4. CASTAGNO, L. A.; CARVALHO, M. L. - Childhood severe and profound sensorioneural deafness. Folha Médica, 91(516), p.397-400, nov./dez.1985.
5. CASTRO JÚNIOR, N. P. et al. - Deficiência auditiva infantil: aspectos de incidência, etiologia a avaliação audiológica- Revista Brasileira de Otorrinolaringologia, 46, p.228-236, 1980.
6. CÓSER. P. L.: VILANOVA. L. C. P. - Rubéola materno fetal: avaliação a perda auditiva por audiometria de tronco cerebral. Revista Brasileira de Otorrinolaringologia, 62 (5), p.366-374, 1996.
7. DAMASCENO, D. Et al. - Avaliação da criança com deficiência auditiva. Anais do Hospital de Siderurgia Nacional, 9(1); p.4850, jan./mar. 1985.
8. DAS, V. K. - Etiology of bilateral sensorioneural deafness in children. The Journal of Laryngology and Otology, 102(11); p.975-980, Nov.1988.
9. DAVIS, A. A - Prevalência da surdez. In: BALLANTYNE. J. Surdez. 5.ed. Porto Alegre: Artes Médicas, 1995. 321p. p5-15.
10. FARHAT, C. K. - Meningites bacterianas purulentas In: ARHAT, C. K. Infectologia pediátrica. São Paulo: Atheneu,1994. 673p. p100-117.
11. HUNGRIA, H. - Otorrinolaringologia. 7.ed. Rio de Janeiro: Guanabara-Koogan,1995. 489p.
12. LINDEN, A. et al. - Deficientes auditivos severos a profundos: um estudo retrospectivo 2 uma analise prospectiva. Revista Brasileira de Otorrinolaringologia, 56, p.76-79, abr./jun.1990.
13. LOPES FILHO, O. - Anatomofisiologia clínica da audição. In:_______; CAMPOS, C. H. A. Tratado de otorrinolaringologia. São Paulo: roca, 1994. 1147p. p.481-509.
14. __________.- Deficiência auditiva. In:________; CAMPOS, C. A. H. Tratado de Otorrinolaringologia. São Paulo: Roca, 1994. 1147p. p531-543.
15.________; Otite media crônica secretória. In________; CAMPOS, C. A. H. Tratado de Otorrinolaringologia. São Paulo: Roca, 1994. 1147p. p.677-694.
16.___________; RABINOVICH, K. - Avaliação da Audição na Criança. In:______; CAMPOS. C. A. H. Tratado de Otorrinolaringologia. São Paulo: Roca, 1994 p.1147. p.609-619. 17. MARTIN, A. - Causas de Surdez na criança. In Ballantyne, J. Surdez. 5. Ed. Porto Alegre: Artes Médicas, 1995. 321p. p.122171.
18. MARTINS, R. H. G.; HESHIKI, Z.; TAMASHIRO, I. A. - Disacusia neurossensorial em criança. Acta Awho,1(1); p.46-48, dez.1992.
19. MORRISON, A. W. - Surdez sensorioneural Adquirida. In: BALLANTYNE. J. Surdez. 5.ed. Porto Alegre: Artes Medicas,1995. 321p, p173-201.
20. MUNHOZ, M. S. L.; SILVA, M. L. G. - Alguns aspectos sobre anatomofisiologia da audição. Revista Brasileira de Atualização em ORL, 3 (1); p.22-26, Jan. 1996.
21. OLIVEIRA, J. A. A. - Fisiologia clinica da audição - cóclea ativa. In: LOPES FILHO, O.; CAMPOS, C. A. H. Tratado de Otorrinolaringologia. São Paulo: Roca,1994.1147. P.510-608.
22. PARVING, A. - As deficiências auditivas na infância epidemiologia etiologia. Anais Nestlé, 50, p.13-17, 1995.
23. PORTMANN, M.; PORTMANN, C. - Tratado de audiometria clinica. 6° ed. São Paulo: Roca. p.323, 1995.
24. RAMOS, B. D.; FUKUDA, Y.; MASON, M. M. - Rubéola congênita: disacusia neurossensorial a condutiva associadas. Relatos de dois cases. Acta Awho, 11(1), p.46-48, jan./abr.1992.
25. REZENDE, A. G. et al. - Prevenção da instalação de problemas de linguagem decorrentes de perdas auditivas derivadas dos quadros de otite medias crônicas de repetição. RBM Otorrinolaringologia, 2 (2); p.87-89, mar. 1995.
26. SALERNO, R. et al. - Avaliação audiometrica de 840 cases de surdez na criança. Revista Brasileira de Otorrinolaringologia, 45 (3); p.208-214, 1979.
27. SALERNO, R. - Deficiência auditiva na criança. Revista Brasileira de Otorrinolaringologia, 51 (2); p.23-32, abr./jun. 1985.
28. SEIXAS, R. R.; FAZOLO, M.I.; MOREIRA, R. N. - Avaliagao auditiva objetiva através de potenciais evocados. Arquivos de Neuropsiquiatria, 51 (4); p.433-440, 1993.
29. SERVER, J.; VERONESI, R.; CANDEIAS. J. A. N. - A rubeola. In: Veronesi, R. Doenças infecciosas a parasitárias. 8.ed. Rio de Janeiro: Guanabara-Koogan, 1991. 1082p. p.55-63.
30. SHAH, N. - Surdez condutiva. In: BALLANTYNE, J. Surdez. 5.ed. Porto Alegre: Artes Médicas, 1995. 312p. p.90-103.
31. SILVA, A. A. - Aspectos médicos da surdez na infância. Arquivos do Instituto Penido Bum ier, 30 (2); p.107-114, ju1.1988.
32. SILVEIRA, J. A. M. et al. - Potenciais evocados auditivos (EcoG e/ou BERA) em 2.545 crianças com suspeita de disacusia a/ou distúrbio da comunicação (Estudo da etiologia, grau de deficiência auditiva a precocidade do diagnostico). Revista Brasileira de Otorrinolaringologia, 62 (5); p.388-408, 1996.
33. SIMOES, A.M.; MARCIEL-GUERRA. A. T. - A surdez evitável: predominância de fatores ambientais na etiologia da surdez neurossensorial profunda. Jornal de Pediatra, 68 (7/8); p.254257, 1992.
34. TCKER, S. M. - Triagem a tratamento da surdez na pratica clínica. Anais Nestlé, 50, p.18-24, 1995.
* Resident Physician in Otorhinolaryngology at Hospital CEMA.
** Resident Physician in Cardiology at Hospital Sao Paulo - EPM.
*** Faculty Professor of the Discipline of Otorhinolaryngology at UFPA.
Study conducted at Instituto Felipe Smaldone, Belém - Pará, presented as final paper at School of Medicine, UEFA.
Address for correspondence: Adriana S. Lima - Av. Paes de Barros 1667 - Apt° 142/A - Mooca - 03115001 São Paulo/ SP.
Tel: (55 11) 6128-2570-E-mail: adri_lima@hotmail.com
Article submitted on May 22, 2000. Article accepted on July 13, 2000.
Print: ![]()