

Year: 2000 Vol. 66 Ed. 5 - (9º)
Artigos Originais
Pages: 480 to 484
Chronic Voice Disorders in Children and Teenagers: A retrospective Study.
Author(s):
Marcos R. Freitas*,
Sandra Pela**,
Maria L. R. Gonçalves***,
Reginaldo R. Fujita****,
Paulo A. L. Pontes*****,
Luc L. M. Weckx******.
Keywords: chronic dysphonis; child; larynx
Abstract:
Introduction: Dysphonia is a human communication disturb in which the voice fail in carry out its basic role of transmission of the verbal and emotional message of a person. It's not an uncommon symptom in children. The prevalence of dysphonia and articulatory problems in general population of children related in most of epidemic studies, ranges from 6 to 9%. Objective: The purpose of the present study is to discuss the main causes of dysphonia in children and teenagers seen in an outpatient department of a tertiary hospital. Material and method: Forty nine patients (32 boys and 17 girls) attended at division of pediatric otorhinolaryngology of Universidade Federal de São Paulo (UNIFESP/ EPM), with complaint of voice disorder, were evaluated retrospectively. Results: The age range from 3 to 16 years old, with predominance between 4 and 11 years old. The most frequent lesions were vocal nodules (44,89%) and minimal structural alterations (36,73%). Minimal structural alterations were related mainly to harsh breathy vocal quality while vocal nodules to hoarse breathy. Conclusions: Vocal nodules are the lesions more frequently diagnosed between children and teenagers with complain of dysphonia, prevailing in boys under 12 years old, and girls from this age.
![]()
INTRODUCTION
Spoken language is the primary means of communication among human beings. Not only words convey meaning, but also the voice reaches the listener, expressing emotions, fears, anxiety, happiness - feelings. Voice is the physical reflection of thought. To define vocal quality is not an easy task because normal parameters are related to biological sociocultural and personality factors. However, any deviation from patterns established by the social group may lead to social stigma of people. This is especially true if the alteration takes place at an early phase of character and personality formation, such as childhood and teenager years.
Harmonious voice is the voice that reaches listeners with good quality and is produced by the speaker without tension or discomfort. In order to achieve that, it is necessary to have a perfect interaction between all muscles employed in voice production, in addition to integrity of all tissues that serve speech mechanism. If this situation is present, we call it euphonia16. Dysphonia is a situation in which there is a rupture of these interrelations, at the level of air column production (rib cage, lungs and diaphragm), vibrating system (vocal folds), resonance system (nasal, oral and pharyngeal cavities), articulation system (lips, tongue, teeth, soft and hard palate and mandible) or at auditory feedback.
Dysphonia is a disorder of human communication in which the voice does not play its basic role of transmitting a verbal and emotional message from a subject. It represents any difficulties in vocal utterance that impairs natural vocal production, manifested by a limited series of alterations, such as tension during production, difficulty to maintain voice, fatigue during speech, variations of habitual fundamental frequency, hoarseness, lack of volume and projection, loss of vocal efficiency, and low vocal resistance, among others. Classification of dysphonias according to etiology is divided into 3 categories: functional, organic-functional and organic dysphonias3.
As children grow older and are exposed to a variety of groups and role models, they normally learn how to adjust spontaneously their vocal style according to the communication setting. If the vocal problem is related to anatomical or physiological deviations of vocal tract, children tend to compensate them. Many factors operate simultaneously to aggravate and maintain the problem. In most cases, voice problems seem to be correlated with vocal abuse1.
Dysphonia is not an uncommon symptom in children. Most epidemiological studies report a prevalence of 6 to 9% of dysphonia and articulation problems in childhood4,5,9, and in 2/ 3 of the cases, the affected subject is a boy11. Etiologies differ a lot, from functional alterations, to nodule lesions and disabling and life-threatening lesions, such as tumors and different degrees of laryngeal stenosis. Therefore, a thorough diagnostic assessment is always required and it has been made easier in recent years thanks to the development of effective little invasive methods, such as videolaryngoscopy and videolaryngostroboscopy.
Risk factors vary according to type of etiology of dysphonia and include vocal abuse and vocal misuse3,18, family history, velopharyngeal insufficiency, use of inhaling steroids, endotracheal intubation2, gastroesophageal reflux and allergy10, among others.
The present study aimed at identifying the main causes of dysphonia among children and teenagers treated at a specialized ambulatory of a tertiary hospital, highlighting the importance of early diagnosis and appropriate treatment.
MATERIAL AND METHOD
Between June and December 1997, 49 patients, aged between 3 and 16 years (mean age 8.8 years) and complaining of dysphonia, were treated at Sector of Laryngology and Voice Disorders of the Discipline of Pediatric Otorhinolaryngology at Universidade Federal de São Paulo (UNIFESP/EPM). The present study was carried out retrospectively.
All patients were submitted to videoendoscopic exam to define etiologic diagnosis of affection. In 25 (51%), we carried out laryngoscopy with 3.2mm flexible endoscope; in 15 (30.6%), with 8.Omm rigid endoscope, and in 9 (18.4%), with both methods.
Topic anesthesia with neotutocaine 2% in the nasal fossae and/or lidocaine spray 10% in the oral cavity were employed before the procedure. In younger children, we rarely required physical restraint because parents helped us with that.
Exams were conducted by otorhinolaryngologists followed by the speech pathologist responsible for the case. Organic alterations of vocal folds were identified according to the definition by Bouchayer and Cornut6, except for minimal laryngeal structural alterations, defined according to Pontes et al.17.
Assessment of vocal quality was performed on the same day using a speech and hearing screening instrument. Alterations of quality are perturbations of sound generated at the level of vocal folds and/or vocal tract. The main vocal quality alterations were hoarseness, breathiness and harshness19.
RESULTS
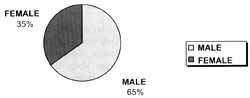
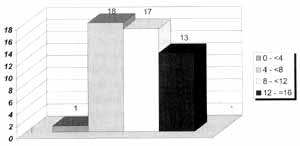
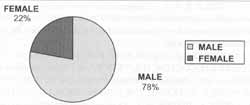
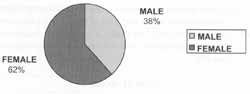
Among 49 studied subjects, 32 were male and 17 were female patients, resulting in a ratio of approximately 2 boys to 1 girl (Graph 1). Most of the patients (71.42%) were in the age range 4 to 11 years (Graph 2). When considered according to age range, up to 11 years, lesions were predominant in male subjects (77.77%) (Graph 3), whereas from 12 years of age on, there was a predominance of female patients (61.54%) (Graph 4).
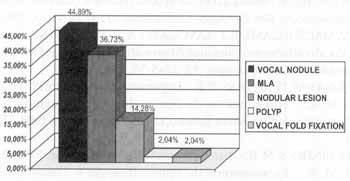
The most frequently diagnosed lesions were vocal nodule in 44.89% of patients, and laryngeal minimal structural alterations in 36.73%. In one patient we detected polyp of vocal fold and, in another, fixation of vocal fold secondary to subglottic stenosis post-orotracheal intubation. In 7 patients (14.28%) it was not possible during the initial assessment to conclude differential diagnosis between vocal nodule and minimal laryngeal alterations. Therefore, these alterations were identified as nodule lesions (Graph 5).
Considering the diagnosis of vocal nodule, among children younger than 12 years there was a predominance in male subjects (approximately 2:1). From then on, girls were clearly more affected than boys (1:5) were. The same was true for the group younger than 12 years with diagnosis of minimal laryngeal alterations, with predominance of male patients (12:1). In the group older than 12 years, despite the small number of cases, there was no predominance of sex.
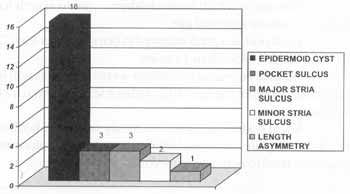
Minimal laryngeal structural alterations found were epidermoid cyst (16), pocket sulcus (3), major stria sulcus (3), minor stria sulcus (2) and asymmetry of length (1) (Graph 6).
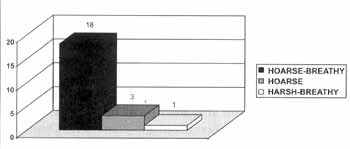
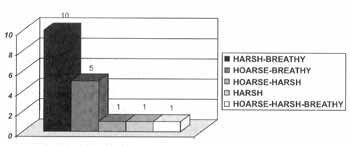
All assessed patients had some kind of primary or secondary organic lesion, characterizing situations of organic or organic-functional dysphonia. Speech and hearing screening revealed vocal quality predominantly hoarse and breathy in patients with vocal nodules (Graph 7) and harsh and breathy in patients with minimal laryngeal alterations (Graph 8).
DISCUSSION
The approach of vocal problems in children differs a lot from aspects concerning the adults. In addition to the fact that these problems may be associated with other developmental disorders, children are not normally prone to cooperate with diagnostic and therapeutic procedures, which should be, therefore, minimally invasive and the least tiring possible. Moreover, involvement of parents and other family members is essential for precise diagnosis and successful therapy.
As shown in our study, voice problems in children before vocal changes are more common in boys, in a ratio of about 3.5:1. Studies by Leqoq and Drap showed similar results. It is believed that it is more predominant in male patients because boys tend to play more aggressive and competitive role socially speaking', which leads to an intense use of speaking system. From 12 years of age on, alterations are more predominant in female patients, because of the higher prevalence of vocal nodules in people of the sex.
The highest incidence (71.42%) was concentrated in school age children (4 to 11 years). It is believed that this fact is related to more vocal use when children are at school, there are more interpersonal relationships and enhanced aggressiveness observed, after the passive dependence of the baby in the first years of life and the relative independence of childhood18.
Graph 1. Distribution of sex.
Graph 2. Distribution of age ranges.
Vocal nodules were the most frequent lesions, followed by minimal laryngeal alterations. Other studies estimated that nodules account for 38 to 78% of chronic dysphonia in childhood7.
In most studies, authors reported predominance of vocal nodules in male children4,7,13. Our sample revealed a higher prevalence in boys than in girls below 12 years of age. In children older than 12 years, there was an inverted predominance. This change may be explained by the fact that from adolescence on, anterior-posterior growth of larynx in male subjects leads to a glottic proportion (GP = relation between intermembranous and intercartilaginous of glottis) that develops from 1 to 1.3 and it remains approximately 1 in female larynxes. Male glottic proportion (1.3), associated with a smaller opening angle of vocal folds, favors glottic coaptation17, reducing the prevalence of vocal nodules in men after adolescence.
Güntert observed in a study with 40 children that 20 patients with vocal nodules, when compared to control children (without vocal nodules), had more difficulties in emotional and cognitive aspects. It may lead to communication and language inability, resulting in incorrect use of voice and originating organic-functional dysphonias.
Graph 3. Distribution of sex up to 11 years.
Graph 4. Distribution of sex after 12 years.
Graph 5. Diagnoses.
Graph 6. Minimal structural alterations.
Graph7. Vocal nodule - vocal quality.
Graph 8. MLA - vocal quality.
As to minimal laryngeal alterations, there was clear predominance of male subjects before the age of 12 years. Since these minor anatomical deviations or small alterations of structural configuration of larynx may or may not impact voice15, we can not conclude that this finding corresponds to what would be the result in the general population (many asymptomatic cases), or if it reflects only the fact that the complaint of dysphonia is more common among boys because of what has already been listed before.
There are 3 basic alterations of vocal quality that may be identified during the assessment of dysphonic patient: hoarseness, normally corresponding to irregularity of vibration of vocal fold mucosa, is phonation produced together with extra noise in voice; harshness, that reflects reduction or absence of vocal fold mucosal wave, producing a not very pleasant sound, and breathiness, that corresponds to the presence of audible background noise, and the common pathophysiologic correlate is the presence of glottic chink14. Therefore, lesions that have a mass effect on the vocal folds such as nodules and polyps, resulting in irregularities of vibration, are more associated with hoarse voice, whereas minimal laryngeal structural alterations manifest with harsh voice.
To treat early and correctly the voice disorders in children is the task that voice therapists and otorhinolaryngologists should keep in mind, because the cry of a child today may turn tomorrow into the voice of a singer, actor, lawyer, teacher or any other professional who will rely on the voice to carry out his or her job.
CONCLUSIONS
1. Vocal nodules are the most frequently diagnosed lesions in children and adolescents who complain of dysphonia, followed by minimal laryngeal structural alterations.
2. The age in which more, children come to search for medical treatment is school age.
3. Vocal nodules predominated in boys younger than 12 years and in girls older than 12 years.
4. Minimal laryngeal alterations were more common in male subjects before the age of 12, without sex predominance after that.
5. Vocal nodules are predominantly related to hoarse-breathy vocal quality, whereas laryngeal minimal alterations are more correlated to harsh-breathy voice.
REFERENCE
1. ANDREWS, M. L. - Terapia vocal para crianças: os primeiros anos escolares. Porto Alegre, Artes Médicas, 1998, 240p.
2. BECKFORD, N. S.; MAYO, R.; WILKINSON, A., III; TIERNEY, M. - Effects of short-term endotracheal intubation on vocal function. Laryngoscope, 100: 331-6, 1990.
3. BEHLAU, M. S.; PONTES, P. A. L. - Avaliação a tratamento das disfonias. São Paulo, Lovise, 1995, 312p.
4. BELHAU, M. S.; GONQALVES, M. I. R. - Considerações sobre disfonia infantil. In: FERREIRA, L. P. - Trabalhando a Voz, São Paulo, Summus Editorial, 1987, 99-107.
5. BLOOM, L.; ROOD, S. - Voice disorders in children: structure and evaluation. Pediatr. Clin. North. Amen, 28: 957-63, 1981.
6. BOUCHAYER, M.; CORNUT, G. - Microsurgery for benign lesions of the vocal folds. Ear Nose Throat J., 67 446-66, 1988.
7. GRAY, S. D.; SMITH, M. E.; SCHNEIDER, H. - Voice disorders in children. Pediat. Clin. North Amer.. 43 (6):1357-84. 1996.
8. GÜNTER, A. E. V. A. - Crianças com nódulo vocal: estudo da personalidade por meio da prova de Rorschach. São Paulo, 1996. [Tese de Doutorado-Universidade Federal de São Paulo / Escola Paulista de Medicina].
9. HIRSCHBERG, J.; DEJONCKERE, P. H.; HIRANO, M.; MORI, K.; SCHULTZ-COULON, H. J.; VRTICKA, K. -Voice disorders in children. Int. J. Pediatr. Otorhinolaryngol., 32: S109-25,1995.
10. HONE, S. W.; DONELLY, M. J.; ROBERTSON, J.; COAKLEY, R.; O'NEIL, S.; WALSH, M. J. - La dysphonie et l'inhalaion des corticoides: une étude prospective. Rev. Laryngol. Otol. Rhinol., 117 (4): 323-25, 1996.
11. LEQOC, M.; DRAP, F.: Enquête epidemiologique sur la dysphonie de l'enfant a l'occasion de sa rentrée scolaire en cours préparatoire. Rev. Laryngol. Otol. Rhinol., 114 (4): 331-3, 1996.
12. MACWILLIAMS, B. J.; LAVORATO, A. S.; BLUESTONE, C. D. -Vocal cord abnormalities in children with velopharyngeal valving problems. Laryngoscope, 83: 1745-53, 1973.
13. NAVAS, D. M.; DIAS, P. R. - Disfonias funcionais. In: PINHO, S. M. R. - Fundamentos de Fonoaudiologia - Tratando os Distúrbios da Voz, Rio de Janeiro, Guanabara Koogan,1998, 739.
14. PINHO, S. M. R. - Avaliação e tratamento da voz. In: PINHO, S. M. R. - Fundamentos de Fonoaudiologia - Tratando os Distúrbios da Voz, Rio de Janeiro, Guanabara Koogan,1998, 03-64.
15. PONTES, P.; BEHLAU, M.; GONÇALVES, I. - Alterações estruturais mínimas de laringe (AEM): considerações básicas. Acta Awho, 13 (1): 02-06, 1994.
16. PONTES, P. A.; BELHAU, M. S. - Disfonias funcionais. In: COSTA, S. S.; CRUZ, O. L. M.; OLIVEIRA, J. A. A. Otorrinolaringologia, Princípios e Prática, Porto Alegre, Artes Medicas, 1994, 444-53.
17. PONTES, P. A. L.; GADELHA, M. E. C.; GONCALVES, M. I. R. - Alerações Estruturais Mínimas da Laringe. In: PINHO, S. M. R. - Fundamentos de Fonoaudiologia -Tratando os Distúrbios da Voz, Rio de Janeiro, Guanabara Koogan, 1998, 65-71.
18. TOOHILL, R. J. - The psychosomatic aspects of children with vocal nodules. Arch. Otolaryngol., 101: 591-95, 1975.
19. WILSON, K. - Problemas de voz em crianças. Terceira edição, São Paulo, Manole, 1994, 384p.
* Assistant Professor of otorhinolaryngology at Faculdade de Medicina da Universidade Federal do Ceara (UFC), Specialist in Pediatric Otorhinolaryngology at UNIFESP/EPM
** Master Degree studies in Human Communication Disorders under course at UNIFESP/EPM. Professor of Speech and Hearing Pathology at Unicastelo and Uniban.
*** Post-Doctorate Degree at University of California, Davis, USA. Head of Ambulatory of Voice of the Discipline of Human Disorders at UNIFESP/EPM.
**** Doctor Degree in Medicine and Master in Otorhinolaryngology at UNIFESP/EPM. Head of the Clinic of the Discipline of Pediatric Otorhinolaryngology at UNIFESP/EPM.
***** Faculty Professor of the Discipline of Pediatric Otorhinolaryngology at UNIFESP/EPM.
****** Full Professor and Head of the Discipline of Pediatric Otorhinolaryngology at UNIFESP/EPM.
Affiliation: Discipline of Pediatric Otorhinolaryngology, Department of Otorhinolaryngology and Human Communication Disorders - EPM-UNIFESP.
Study presented at 34° Congresso Brasileiro de Otorrinolaringologia, held in Porto Alegre - RS, November 18 - 22 1998.
Address for correspondence: Rua dos Otonis, 684 - Vila Clementino - 04025-001 São Paulo /SP. Tel/Fax: (55 11) 576-4395 - E-mail: marrabelo@uol.com.br
Article submitted on May 18, 2000. Article accepted on July 13, 2000.
Print: ![]()