

Year: 2003 Vol. 69 Ed. 6 - (20º)
Relato de Caso
Pages: 857 to 860
 PDF PT
PDF PT Kartagener Syndrome: a case report
Author(s):
Rubem C. Swensson1,
José J. Jorge Júnior2,
Rogério P. Swensson3,
Patrícia K. M. S. Machado4,
José F. M. Morad Filho5,
Camila P. Santana6
Keywords: Kartagener syndrome, Kartagener triad, sinusitis, dextrocardia
Abstract:
The Kartagener Syndrome is a rare recessive autossomical disease including the triad: chronical sinusitis, bronchiectasis and situs inversus with dextrocardia. The incidence of this genetical disorder is estimated about 1/25,000. Our purpose in this case report is to include new informations for who search about this syndrome. Tomography of chest, abomen and cranium, audiometry, impedance and nasopharyngoscopy were done.
![]()
INTRODUCTION
Kartagener's syndrome was initially described by Siewert, in 1904, and finally defined by Kartagener in 1933.1-3
Kartagener's syndrome is caused by a rare recessive autosomal disease that presents a triad comprising chronic pansinusitis, bronchiectasis and situs inversus with dextrocardia 1. During the progression of the disease, the patient can present diffuse panbronchiolitis, sterility, chronic otitis media and localized lesions especially on respiratory bronchioles 4.
LITERATURE REVIEW
As already introduced, Kartagener's syndrome is caused by a recessive autosomal disease characterized by situs inversus, bronchiectasis and chronic sinusitis 1. The incidence is of approximately 1/25,000 4.
The patients typically present respiratory tract infections since childhood. In addition to chronic pneumonia, chronic otitis media, nasal polyps, productive cough, hemoptysis and occasional respiratory and cardiac failure 1, 4.
It is a subgroup of ciliary motility syndrome also called primary ciliary dyskinesia 5-7. Ciliary dyskinesia, generator of mechanical force of ciliary movement, is deficient in patients who have Kartagener's syndrome 8.
Kartagener's syndrome and primary ciliary dyskinesia are associated with ciliary structure abnormalities, especially through loss or modification of dynein structure, modifying the radial radius and losing the central part of the microtubules 2, 3. These abnormalities can be observed through spermatozoa flagellum 9, 10.
Electron microscopy of cilia is difficult since the sample for biopsy is frequently affected by recurrent infections experienced by the patients who have the syndrome 11.
The clinical aspect of primary ciliary dyskinesia presents productive cough, pulmonary infections, sinusitis, otitis media and infertility, being attributed, respectively, to reduction of mucous clearance from the airways, paranasal sinuses and reduction of sperm motility 8. Bronchiectasis and chronic infections can result from final stages of pulmonary disease, being followed by dyspnea and heart failure 12.
The diagnosis of bronchiectasis depends on the demonstration of typically irregular saccular or cylindrical bronchial dilations through high resolution computed tomography (CT scan) 13.
Patients with bronchiectasis presented persistent and productive cough and sometimes dyspnea and the symptoms are frequently aggravated by recurrent respiratory infections 14.
CASE REPORT
MPS, 8-year-old male Caucasian. The patient presented history of recurrent pneumonia since 12 days of life, rhinitis, serous otitis media with episodes of acute otitis media and chronic sinusitis. At 12 days of life, he had the first episode of pneumonia and up to 7 months, he had presented two more recurrences.
They detected malformation named situs inversus totalis, through radiology, at 5 years of age and after that, he was referred to the cardiologist because he had heart murmur. There were no cases of malformation in the family.
The physical examination presented affections that suggested the presence of situs inversus, such as palpation of heart ictus on the right, palpation of the liver on the left, and tympanism on the right hypochondrium.
He presented rude breathing on both pulmonary bases, yellowish post-nasal secretion and systolic murmur on mitral focus.
We conducted CT scan of the thorax, abdomen and head, in addition to high resolution CT scan of thorax, audiometry, immittanciometry and videonasofibroscopy.
Figure 1. Dextrocardia.
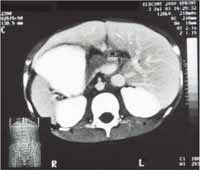
Figure 2. Abdominal organs in inverted situs.
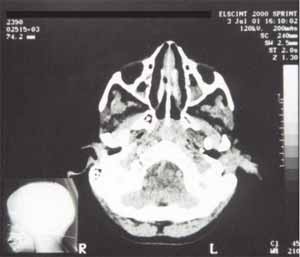
Figure 3. Partial opacification of maxillary sinus.
Figure 4. Partial opacification of maxillary sinus.
DISCUSSION
CT scan of the thorax and abdomen confirmed that the patient had situs inversus totalis, and head CT scan demonstrated opacification of maxillary and ethmoid sinuses, inferring process of inflammatory sinus pathology. The results of the clinical examination and audiological assessment suggested secretory otitis media. Videonasofibroscopy suggested rhinitis, with active sinus pathology. High resolution CT scan of the thorax indicated atelectasia, probably caused by recurrent pulmonary infection learned through the history of the patient, without presenting evident bronchiectasis.
CLOSING REMARKS
Taking into account that Kartagener's syndrome is characterized by situs inversus, chronic sinusitis, serous otitis media and pulmonary processes, the case reported here is very likely an example of the syndrome.
The definite diagnosis is only obtained by ciliary movement test through electron microscopy and saccharin examination of collected sperm, which is ethically not possible owing to the age of the patient, which would require testis punch.
REFERENCES
1. Kartagener M. Zur Pathologie der Bronchiektasien: Bronchiektasien bei situs viscerum invertus. Beitr Klin Tuberk 1933; 83:489-501.
2. Pederson H, Mygind N. Absence of axonemal arms in nasal mucosa cilia in Kartagener's syndrome. Nature 1976; 262:494-5.
3. Homma H, Yamanaka A, Tanimoto S et al. Diffuse panbronchiolitis. A disease of the lung. Chest 1983; 83:63-9.
4. Griffin J, Wilson J. Disorders of the testis. Harrison's Principles of Internal Medicine 1991; 1772.
5. Greenstone M, Cole PJ. Primary ciliary dyskinesia. Arch Dis Child 1984; 59:704-6.
6. Yokota T, Ohno H, Tamura K et al. Ultrastructure and function of cilia and spermatozoa flagella in a patient with Kartagener's syndrome. Int Med 1993; 32: 593-7.
7. Waiter RT, Danielson JR, Reyes HM. Characterization of a chemotactic defect in patients with Kartagener syndrome. Arch Otolaryngol Head Neck Surg 1990; 116: 465-9.
8. Nijs M, Vanderzwalmen P, Vandamme G et al. Fertilizing ability of immotile spermatozo after intrazytoplasmic sperm protein. Hum Reprod 1996; 11:2180-5.
9. Van Steirteghem A, Nagy Z, Joris H et al. High fertilization and implantation rates after intracytoplasmic sperm injection. Hum Reprod 1993; 7:1061-6.
10. Vandervorst M, Tournaye M, Camus M et al. Pacients with absolutely immotile spermatozoa and intracytoplasmic sperm injection. Hum Reprod 1997; 12:2429-33.
11. Schidlow DV, Panitch H, Katz SM. The immotile cilia syndrome. In: Pediatric Respiratory Disease. W.B. Saunders Co. 1993; 550-63.
12. Rossman CM, Forrest JB et al. Immotile Cilia Syndrome in Persons With an Without Kartagener's Syndrome. American Review of Respiratory disease. 1980; 121:1011-6.
13. Mayo PO. Kartagener's syndrome. J Thorac cardiovasc surg 1961; 42:39-42.
14. Turley K. Thoracic Wall Pleura Mediatinum & lung. Current Surgical Diagnosis & Treatment 1994; 3445.
1 Otorhinolaryngologist, Assistant physician, Discipline of Otorhinolaryngology, Medical School of Sorocaba, PUC-SP.
2 Associated Professor, Department of Surgery, Coordinator of the Discipline of Otorhinolaryngology, Medical School, PUC-SP.
3 Undergraduate, Medical School PUC-SP.
4 Undergraduate, Medical School PUC-SP.
5 Undergraduate, Medical School PUC-SP.
6 Undergraduate, Medical School PUC-SP .
Affiliation: Pontifícia Universidade Católica de São Paulo, Medical School of Sorocaba.
Address correspondence to: Rubem Cruz Swensson - R. Rocha Pombo, 139 Sorocaba SP 18044-030
Tel (55 15) 231-1663 / 232-7838 / 221-7866 - Fax (55 15) 220-1926
Study presented as poster at Congresso Brasileiro de ORL in 2002, in Florianópolis.
Article submitted on December 30, 2002. Article accepted on April 10, 2003.


Print: ![]()