

Year: 2003 Vol. 69 Ed. 6 - (2º)
Artigo Original
Pages: 740 to 743
 PDF PT
PDF PT Contribution to the anatomic study of the innervation of the posterior and lateral crico-arytenoid muscles
Author(s):
João Adolfo Caldas Navarro1,
João Lopes Toledo Filho2,
Jesus Carlos Andreo2,
Gustavo Henrique Souza Silva3,
Marcos Roberto Banhara4
Keywords: larynx, innervation, intrinsic musculature, recurrent laryngeal nerve
Abstract:
The complexity of the laringeal inervation has motivated the appearing of a large number of researches, specially that ones related to the recurrent laringeal nerve (RLN). The plentiful variation, the important surgical appliance and even the dificulties in the functional corroboration of the nervous branchs to the larynx make this subject intriguing and challenging. Facing this, the aim of the current study is the elaborated investigation about the recurring laringeal nerve (RLN) branches, directed to posterior (PCA) and lateral (PCL) cricoarytenoid muscles. Study design: Experimental. Material and Method: It was realized bilateral dissections, on the surgical microscope, in 20 adult's larynxes, from both Sex, referring to posterior and posterolateral regions of the larynx. Results: There are morfological diferences in the RLN's branches that reach the PCA and PCL muscles, observing the unipedicular, bipedicular and tripedicular inervations. There are filaments of PCA muscle arranged obliquely to the main branch, forming "aqueduct", under wich passes the RLN. Conclusions: The recurring laringeal nerve (RLN) penetrates the larynx beneath its inferior border, behind the cricothyroid joint. The caracteristical inervation of both muscles (PCA and PCL) is predominantly bipedicular; the mentioned "aqueduct", formed by the PCA's fiber bundles, is a anatomical variation not much studied.
![]()
INTRODUCTION
The complex laryngeal innervation has motivated the conduction of many studies, especially those related to the laryngeal recurrent nerve (RLN), defined in texts and periodicals as one of the most important branches of the vagus nerve owing to its anatomical and functional relations 7, 9, 10, 11, 15. The many variations, important surgical applications, especially in thyroidectomy 2, 3, 4, and difficulties to functionally confirm the nervous branches of the larynx makes it an intriguing and challenging topic for the researcher to investigate.
The laryngeal recurrent nerve is predominantly motor, comes of the vagus nerve on the upper portion of the thorax, goes through the angle between the trachea and the esophagus and penetrates into the larynx, under the lower margin of the lower pharyngeal constrictor muscle 7, 9, 10, 11, 15. Reaching the posterior aspect of the larynx, it is divided into 5 branches, all motor branches, except for the descending branch of the superior laryngeal nerve, over the posterior aspect of the posterior cricoarytenoid muscle (PCA), forming Galeno's anastomosis 1,5,6,14.
The present study aimed at investigating in details the path of the laryngeal recurrent nerve into the posterior cricoarytenoid and lateral cricoarytenoid muscles. The results obtained are extremely important to better systematize the anatomical relations of RLN in the studied region, since there are few literature references about the anatomical behavior of these nerves and their branches.
MATERIAL AND METHOD
We used 20 adult cadaver larynges without pathology and identification of gender or age, available at the laboratory of Anatomy, Dental School, University of Sao Paulo, during the period of study. They were removed in bloc, placed in formol at 5% and stored in containers without identification. During dissections, we used surgical microscope MC900 (D.F. VASCONCELLOS), 200mm objective and 12.5mm oculars.
Dissections were made on the posterior and posterior-lateral regions of the larynx. To facilitate access to muscles PCA and LCA we removed the laminas of the thyroid cartilage.
Recurrent laryngeal nerve was dissected from the limit between the cricoid cartilage and the trachea, exposing in its path the right and left posterior-lateral walls of the larynx. The ramification of the recurrent laryngeal nerve (RLN) was exposed up to the level of LCA muscle, evidencing the characteristic innervation of muscles PCA and LCA, the main objective of the present study.
Dissections were described and documented with photographs, using a digital camera Nikon Coolpix 990, and printed with HP 840C printer.
RESULTS
Based on the forty dissections of the recurrent laryngeal nerve on the right and left, we observed the following results:
Longitudinal and parallel distribution of the posterior cricoarytenoid muscle, ascending from the cricoid cartilage lamina to the muscle process of the homolateral arytenoid cartilage, in which they were inserted, was observed in 34 dissections (85%) (Figures 1, 2, 3, 4, and 5).
Presence of posterior cricoarytenoid muscle placed obliquely to the main bundle in 6 dissections (15%). The fibers emerged from the main bundle and were attached under the inferior cornus of the thyroid cartilage, in the thyroid articular aspect of the cricoid cartilage. This distribution was similar to the muscle "aqueduct" under which RLN runs (Figure 3).
In 100% of the pieces we observed the same RLN path on the right and left. They run through the angle formed by the trachea and the esophagus and penetrate into the larynx, under the inferior margin of the pharyngeal lower constrictor muscle, through the cricoarytenoid joint (Figures 1, 2, 3, 4, and 5).
Different morphology types of innervation of the anterior branch of RLN reached PCA and LCA muscles: unipedicular, bipedicular and tripedicular. We observed that the most common morphological type in the dissections was bipedicular.
Unipedicular ramification was found in 13 dissections (32.5%) of PCA muscle and in 4 dissections (10%) of LCA muscle (Figure 5). The bipedicular morphological type for muscles PCA and LCA was found in 17 dissections (42.5%) and in 27 dissections (67.5%), respectively (Figure 1). Finally, the tripedicular innervation was observed in muscles PCA and LCA, respectively, in 9 dissections (22.5%) (Figure 2).
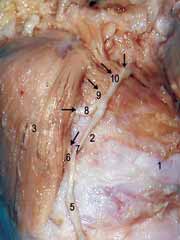
Figure 1. Posterior-lateral view of larynx: 1. Cricoid cartilage 2. Thyroid articular aspect of cricoid cartilage; 3. Posterior cricoarytenoid muscle (PCA); 4. Lateral cricoarytenoid muscle (LCA); 5. Recurrent laryngeal nerve (RLN); 6, 7, 8, 9 and 10. Branch of recurrent laryngeal nerve (arrows). Sites in which the branches of RLN reach muscles PCA and LCA, respectively.
Figure 2. Posterior-lateral view of the left larynx: 1. Cricoid cartilage; 2. Thyroid articular aspect of cricoid cartilage; 3. Posterior cricoarytenoid muscle (PCA); 4. Lateral cricoarytenoid muscle (LCA); 5. Recurrent laryngeal nerve (RLN); 6, 7, 8, 9 and 10. Branch of recurrent laryngeal nerve; (arrows). Sites in which the branches of RLN reach muscles PCA and LCA, respectively.
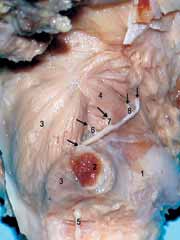
Figure 3. Posterior-lateral view of the right larynx: 1. cricoid cartilage; 2. Thyroid articular aspect of cricoid cartilage; 3. Posterior cricoarytenoid muscle (PCA); 3´. PCA fibers that get separated from the main bundle and get inserted into 2, 4. Lateral cricoarytenoid muscle (LCA); 5. Recurrent laryngeal nerve (RLN); 6, 7 and 8. Branch of recurrent laryngeal nerve; (arrows). Sites in which the branches of RLN reach muscles PCA and LCA, respectively.
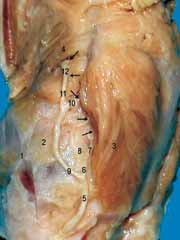
Figure 4. Posterior-lateral view of the left larynx: 1. Cricoid cartilage; 2. Thyroid articular aspect of cricoid cartilage; 3. Posterior cricoarytenoid muscle (PCA); 4. Lateral cricoarytenoid muscle (LCA); 5. Recurrent laryngeal nerve (RLN); 6, 7, 8, 9, 10, 11 and 12. Branch of recurrent laryngeal nerve; (arrows). Sites in which the branches of RLN reach muscles PCA and LCA, respectively.
Figure 5. Posterior-lateral view of the left larynx: 1. Cricoid cartilage; 2. Thyroid articular aspect of cricoid cartilage; 3. Posterior cricoarytenoid muscle (PCA); 4. Lateral cricoarytenoid muscle (LCA); 5. Recurrent laryngeal nerve (RLN); 6, 7 and 8. Branch of recurrent laryngeal nerve; (arrows). Sites in which the branches of RLN reach muscles PCA and LCA, respectively.
DISCUSSION
Dissections confirmed the path of the right and left recurrent laryngeal nerve described in the studies by SPALTEHOLZ (1967), ROMANES (1976), GRAY (1989), PAUWELS (1991) and MOORE (1992). They penetrated in the inferior margin of the right and left pharyngeal lower constrictor muscles through the cricothyroid joint to innervate the intrinsic laryngeal muscles, except for cricothyroid.
According to NGUYEN, 1989, the anterior branch of recurrent laryngeal nerve, in its hypopharyngeal portion, innervates the PCA muscle, presenting three different morphological types: unipedicular, bipedicular and tripedicular. In its laryngeal portion, it sends branches to the LCA muscle, observing the three possibilities of pedicular innervation, being unipedicular the most common one. Through dissections we confirmed what the author reported; however, in both muscles, PCA and LCA the most common morphological type was bipedicular.
SANDERS, in 1994, demonstrated that PCA muscle comprised three neuromuscular behaviors: vertical, oblique and horizontal. He also observed the junction of the vertical and oblique compartments, considered as a single one owing to its characteristic innervation. The main branch of the RLN nerve at the level of PCA is divided into two secondary branches. The first RLN branch innervates the vertical and oblique compartments and the second branch innervates the horizontal compartment. Such conclusions were confirmed. We also observed compartmental division of PCA muscle, evidenced by ramification of the main branch of RLN (bipedicular) in most of the dissections.
The distribution of PCA muscle fibers placed obliquely to the main bundle and inserted under the lower cornus of the thyroid cartilage, in the thyroid articular aspect of the cricoid cartilage, was not observed in any of the studied descriptions.
CONCLUSION
Laryngeal recurrent nerve penetrates into the larynx under the lower margin of the pharyngeal lower constrictor muscle through the cricothyroid joint. The anterior branch runs on the laryngeal posterior-lateral aspect, sends branches to PCA muscle in its hypopharyngeal portion, and to LCA muscle, in its laryngeal portion. The characteristic innervation of both muscles (LCA and PCA) is bipedicular even though it also presents unipedicular and tripedicular morphological types.
CLOSING REMARKS
The present study was based on dissections of the laryngeal recurrent nerve branches, which innervate PCA and LCA muscles in the right and left laryngeal posterior-lateral walls. The results obtained are extremely important to better systematize the anatomical relations of the recurrent laryngeal nerve in the studied region, since there are few literature reports about the anatomical behavior of this nerve and its branches.
ACKNOWLEDGEMENT
We would like to specially thank Prof Dr João Adolfo Caldas Navarro who not only believed in the project but also worked vary hard to support its conduction.
"The one who should have been only a teacher, was a master; as a master, was a friend whose friendship helped us understand and encouraged us to move along our path."
(Unknown author)
REFERENCES
1. Gray H. 1827-1861 - Gray's anatomy/edited by Peter L. Willians et al. Anatomy, descriptive and Surgical. 37th ed. Edinburgh, London, Melbourne: Churchill Livingstone; 1989.
2. Braus H, Elze C. Anatomia des Menschen. 2nd. ed. Aufl, Berlin: Springer; 1934.
3. Hollinshead WH. Anatomy for Surgeons. 1st ed. New York: Hoeber Harper International; 1966.
4. Orts-Llorca FO. Anatomia Humana. 2ª edição. Barcelona: Científico Médica; 1960.
5. Sanders I. The Innervation of the Human Posterior Cricoarytenoide Muscle: evidence for at least two neuromuscular compartments. Laryngoscope 1992; 104: 880-4.
6. Paewels W, Akesson EJ, Stewart PA. Nervios Craneanos - Anatomía y Clínica 1991; Buenos Aires, Bogotá, Madri, México, São Paulo: Editorial Médica Panamericana SA.
7. Romanes GJ. Cunningham Manual de Anatomia Prática. 13ª edição. Editora da Universidade de São Paulo; 1976.
8. Spalteholz W. Atlas de Anatomia Humana Tomo III 3ª edição. Barcelona, Madri, Buenos Aires, Rio de Janeiro: Editorial Labor SA; 1967.
9. Moore KL. Clinically Oriented Anatomy. 3rd ed. Baltimore: Willians & Wilkins; 1992.
10. Tomasoh J, Britton WA. A fibre-analysis of the laryngeal nerve Supply in man. Acta Anat 1955; 23: 396-8.
11. Brandão G, Ferraz A. Cirurgia de cabeça e pescoço/Volume I - Princípios técnicos e terapêuticos. 1.ª ed. São Paulo, SP: Copyright livraria Roca Ltda; 1989.
12. Sanders I. The Innervation of the Human Larynx. Arch Otolaryngol Head Neck Surg 1993; 119: 934-9.
13. Glendon M, Gardner MD. Posterior Glotic Stenosis and Bilateral Vocal Fold Immobility (Diagnosis and Treatment). Otolaryngol Clin North Am 2000; 33(4): 855-74.
14. Testut L, Laterjet M. Tratado de Anatomia Humana. 9ª edição. Barcelona: Salvat Editores, SA ; 1958.
15. Nguyen M, Junien-Lavillauray C, Faure C. Anatomical intra-laryngeal anterior branch study of the recurrent (inferior) laryngeal nerve. Surg Radiol Anat 1989; 11: 123-7.
1 Faculty Professor of Anatomy, Department of Biological Sciences, Dental School of Bauru, University of Sao Paulo (FOB-USP).
2 Associated Professor, Department of Biological Sciences, Full Professor of Anatomy, Dental School of Bauru, University of Sao Paulo (FOB-USP).
3 Dentist, graduated by FOB-USP; Resident dentist, Course on Surgery and Buccomaxillofacial Traumatology, Associação Hospitalar de Bauru,
Brazilian College of Buccomaxillofacial Surgery and Traumatology.
4 Speech Therapist, graduated by FOB-USP; Researcher, Centro de Pesquisas Audiológicas (CPA), Hospital de Reabilitação de Anomalias Craniofaciais (HRAC)
Study conducted at the Department of Biological Sciences, Discipline of Anatomy, Dental School of
Bauru, University of Sao Paulo. Study financially supported by FAPESP.
Address correspondence to: Alameda Octávio Pinheiro Brisolla, 9-75 - Vila Universitária - CEP: 17012-901 - Bauru - SP.
Tel: (55 14) 235-8226 - FAX: (014) 223-8575. E-mail: jnavarro@usp.br
Article submitted on December 12, 2002. Article accepted on September 25, 2003.


Print: ![]()