

Year: 2003 Vol. 69 Ed. 6 - (1º)
Artigo Original
Pages: 734 to 738
 PDF PT
PDF PT Histologic study of ossification of the thyroid cartilage
Author(s):
Walter P. Cruz1,
Rogério A. Dedivitis2,
Ângelo Sementilli3,
Abrão Rapoport4
Keywords: larynx, thyroid cartilage, ossification
Abstract:
The process of ossification and formation of bone marrow occurs in the larynx cartilages with age. The knowledge of this change is important for differentiation with cartilage invasion by cancer. Aim: Cranial and caudal segments of the thyroid cartilage were obtained from adult male larynges in order to evaluate comparatively the histological changes regarding to the ossification and the bone marrow formation. Study design: Experimental. Material and Method: Seven male adult larynges were obtained from cadavers underwent necrological examination in Posto Médico-Legal de Santos, da Polícia Civil do Estado de São Paulo. The ages ranged from 39 to 60, with median of 53. There were no available data about tobacco and alcohol consumption. The specimens underwent decalcification and stained with H-E. Histometry was performed for quantitative analysis of the ossification while the bone marrow was analyzed according to qualitative criteria (presence or absence). Results: The average ossification was 42.8% and the bone marrow presence was observed in 57.1% in the cranial segments. In the caudal segments, the average ossification was 72.8%, and the bone marrow was detected in 87.5% of the specimens. Conclusion: The ossification in the thyroid cartilage and the bone marrow formation increase and occur earlier moving downward from the cranial to the caudal aspects.
![]()
INTRODUCTION
Preoperative assessment in patients with larynx carcinoma is essential for the most appropriate therapeutic indication. The combination of endoscopic and radiological studies allows the conduction of tumor staging and detection of laryngeal cartilage invasion. Much important information about laryngeal carcinoma can be obtained by endoscopy, however the profound invasion of the tumor can only be estimated. Computed tomography can detect whether there is no invasion of cartilages, but it is difficult for radiologists to determine the radiological difference of tumor invasion and endochondral ossification.
The invasion of the cartilages by tumor can contraindicate partial resection, however, the process of ossification and formation of bone marrow can mimic this infiltration. Thus, precise knowledge of location of ossification points in the thyroid cartilage can help the diagnosis and therefore, therapeutic management 1.
The purpose of the present study was to assess comparatively histology abnormalities that occur to the thyroid cartilage in male adult subjects concerning ossification and bone marrow formation in cranial and caudal portions.
MATERIAL AND METHOD
After previous authorization of the Forensic Center in Santos/SP, we studied larynges collected from seven cadavers submitted to necropsy at the Forensic Center of Santos, Civil Police of the State of Sao Paulo. Ages ranged from 25 to 63 years, median of 53 and mean of 50 years. The studied specimens were from homeless adult male subjects 8 to 24 hours after death. We excluded cadavers whose cause of death had been directly related to larynx of had been manipulated by laryngotracheal intubation, or when they presented beginning of putrefaction. We had no information concerning smoking and alcohol abuse.
To each cadaver, respecting the incisions habitually conducted for the necropsy examination, we dissected and exposed the larynx, made initial inspection allowing the detection of absence of macroscopic lesions of mucosa and cartilages. We removed the extrinsic muscles and external perichondrium of the thyroid cartilage using an electrical saw, removed a small fragment of thyroid cartilage of total thickness of 5x5 millimeters of cranial portion and other fragment of the same size from the caudal portion of the lamina (Figure 1).
The fragments were placed separately in vials with formol and sent to the laboratory of clinical pathology for microscopic examination. Decalcification was obtained by placing the specimens in formic acid solutions at 5% for a period that ranged from 3 to 5 days. The pathologist that conducted the assessment did not know about topography of the lamina for each fragment and the pieces were stained with hematoxillin-eosin.
To study ossification we used the histometric method based on stereology principles, which by quantitative analysis provides percentage values of the analyzed components in a bi-dimensional plan, providing some notion about three-dimensional plan 2, 3. To reach these values, we used an integrating ocular I Kpl-W10X by Zeiss, with a screen of 25 points geometrically distributed. The values obtained expressed a proportion and not an absolute measure. The projected screen over the sections allowed quantification of hits, that is, the points that coincided over the bone and cartilaginous tissues. This procedure was conducted with an objective of 40x, by the pathologist, and for each specimen, ten fields were counted.
The analysis of the presence of bone marrow was made qualitatively, that is, we considered presence or absence in each studied specimen.Table 1. Percentage of bone tissue found and presence of bone marrow in specimens.
Key: + - presence of bone marrow; 0 - absence of bone marrow.
Table 2. Distribution of seven cases based on cranial and caudal portions.
Legend: No - absence of ossification and bone marrow: Yes - presence of both.
RESULTS
In the regions with typical hyaline cartilage we detected typical condrocytes, flatter cells when close to the joint surface and more rounded cells when deep inside (center of the cartilage) and some aggregated, forming isogeneous groups. Ossification, when present, occupied only a well located area of the cartilage or replaced it completely, with presence of only typical lamellar bone tissues, with some signs of Havers' systems. In the first situation, the bone tissue present was lamellar, and the lamellae were parallel to the cartilage surface. In the center of the bone tissue, we observed in some cases the presence of bone cavity filled with fatty tissue or bone marrow with hematopoietic tissue.
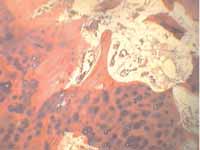
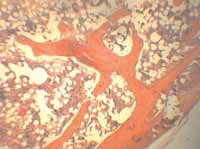
Table 1 represents age, percentage of bone tissue found and presence or not of bone marrow in cranial and causal aspects of the studied cartilage. In the cranial segments, we detected that in three cases there was no ossification or bone marrow. In the other four cases, there was ossification, whose presence varied from 30 to 100% (Figure 2). In all four cases, we observed presence of bone marrow. The mean ossification of the seven cases was 42.8%. The presence of bone marrow was observed in four of the seven cases (57.1%). In caudal segments, only in one case there was no ossification or bone marrow. Ossification was present in all the other cases, ranging from 30 to 100% (Figure 3), being that four of them presented 100% ossification. The mean of seven specimens was 72.8% of ossification. The presence of bone marrow was observed in six of the seven cases (87.5%).
As to statistical analysis, to characterize the sample, we used descriptive statistics. The categorical variables were represented by absolute and relative frequencies and we used central tendency measures and variability for continuous variables (Table 2).
Figure 1. Anatomical specimen studied in cranial (large arrow) and caudal (small arrow) regions in the ala of the thyroid cartilage from where the fragments for histology study were collected.
Figure 2. Section of cranial fragment of thyroid cartilage that reveals cartilage in the margins and beginning of formation of bone lamellae in the center (HE 40x).
Figure 3. Section of caudal fragment of thyroid cartilage showing the bone tissue formed by uniform lamellae and medullar region with hematopoietic cells (HE 40x).
DISCUSSION
Thyroid, cricoid and arytenoid are hyaline cartilages and epiglottis, corniculated, cuneiform and apex of arytenoid are elastic cartilages. As a result of aging, elastic cartilages have a small tendency to calcify, but not to ossify; however, hyaline cartilages become somewhat ossified 4. Thyroid cartilage suffers endochondral ossification as time goes by. The degree of ossification is smaller in female than in male subjects and there is symmetry of ossification of thyroid cartilage in both genders 5.
Hyaline thyroid cartilage presents a progressive increase of collagen fibers and mineralization. The process of mineralization leads to calcification or ossification 6. The process of dissemination of ossification occurs differently for each gender and among people of the same gender and this process is related to the age of subjects 7.
The phenomenon of calcification and ossification should be differentiated. Regardless of the rare cases of true calcareous infiltration, calcium is normally deposited on areas previously affected by other causes. This fact is supported by many pathological descriptions of calcifications of necrotic parts of many organs. The phenomenon is normally observed after the age of 60 years 8. In most of the cases, deposition occurs in the fundamental substance, in which cell death is more marked. Ossification is more frequent in men and after the age of 40 years. The ossified zone presents typical lamellar bone structure. The bone is always delimited by a halo of cartilage, and there is no transition zone, which confirms that it is a replacement process 9.
Calcium is deposited in islands, and there are regions that are densely calcified by the matrix. The degree of differentiation of chondrocytes in the perichondrium is reduced and the cells localized deeply show signs of loss of feasibility, there are focus of erosion and the onset of such affections is sped up by aging 10-12, and it is not observed in neonates or during childhood 13. Osteogenesis may surge as a result of the tension force to which the joint is submitted, such as the stimuli caused by muscle contractions 14. Moreover, disorders of mineral metabolism and other pathological degenerative processes, such as rheumatoid arthritis, impact osteogenesis.
Ossification starts at the subcortical region, involving the central portion of the specimen only in the elderly 15. Ossification of cartilages starts only when the growth of the skeleton is completed 16. There is also the possibility that the stimuli of laryngeal extrinsic and intrinsic muscle contractions have a mechanical effect on tension and pressure, contributing to ossification 17. The case of earliest findings of calcifications was at the end of the second decade of life18. The calcification pattern is similar in identical twins, which indicates hereditary determination 19.
Magnetic resonance study of larynges removed from cadavers showed the presence of hematopoietic tissues in hyaline ossified cartilages. Ossification and signs of bone marrow tissue are observed after the age of 30 years 20. This is the reason why we decided to investigate the age group formed by adults, that is, in subjects that had possibly suffered the histology affection of study, but not too old to have almost completely replacement of the bone tissue in both studied topographies.
The importance of ossification is revealed both by radiological assessment of tumors and conduction of partial laryngectomies, since infiltration of thyroid cartilage stages primary tumors as T4. Tumors frequently present density similar to the portions of the cartilage that have not been ossified. However, the absence of ossification close to a tumor could suggest that the cartilage had been invaded. Tumor invasion can be mistaken by presence of bone marrow, which can mimic infiltration are 21. Tumors do not invade the thyroid cartilage symmetrically as ossification, therefore, the points of ossification should be recognized so that we do not misinterpret the CT scan.
CT scan studies of larynges obtained from cadavers revealed a tendency to ossification as we moved cranial-caudally in the thyroid cartilage1. Simple x-ray studies revealed that ossification of the cartilage occurs in the dorsal-ventral and caudal-cranial direction 5. Our findings coincide with these reports.
CONCLUSION
The analysis of the studied material concluded that in male adults there is a process of ossification and formation of bone marrow with typical hematopoietic tissue in the thyroid cartilage, being more intense in the caudal topography. Such knowledge has an impact in the radiological assessment and management of patients with laryngeal cancer, including the conduction of partial laryngectomies.
REFERENCES
1. Yeager VL, Lawson C, Archer CR. Ossification of the laryngeal cartilages as it relates to computed tomography. Invest Radiol 1982;17:11-9.
2. Underwood EE. Stereology or the quantitative evaluation of microstructure. J Microsc (Oxf.) 1968; 89:161-90.
3. Weibel ER, Kistler GS, Scherle WF. Practical stereological methods for morphometric cytology. J Cell Biol 1970; 30:23-38.
4. Milroy CM. Ossification of the epiglottis. J Laryngol Otol 1992; 106:180-2.
5. Jurik AG. Ossification and calcification of the laryngeal skeleton. Acta Radiol Diagn (Stockh.) 1984; 25:17-22.
6. Strek P, Nowogrodzka-Zagorska M, Skawina A, Olszewski E. Ossification of human thyroid cartilage. Scanning electron microscopic study. Folia Morphol (Warsz.) 1993; 52:47-56.
7. Zeligman SB. Calcification and ossification of thyroid cartilage in men. Arch Anat Histol Embriol 1960;9:97-102.
8. Dedivitis RA, Abrahão M, Simões MJ, Mora AO, Cervantes O. Cricoarytenoid joint: histologic changes during aging. São Paulo Med J 2001; 119:89-90.
9. Amprino R, Bairati A. Studi sulle trasformazione delle cartilagini Del l'uomo nell'accrescimento e nella senescenza. Z Zellforsch Mikrosk Anat 1933;20:143-205.
10. Hass GM. Studies of cartilage IV. A morphologic and chemical analysis of aging human costal cartilage. Arch Pathol 1943; 35:275-84.
11. Kahane JC, Hammons J. Developmental changes in the articular cartilage of the human cricoarytenoid joint. In: Baer T, Harris K, Sasaki C. Vocal Physiology. San Diego: College Hill Press; 1987. p. 14-28.
12. Paulsen FP, Tillmann B. Composition of the extracellular matrix in human cricoarytenoid joint articular cartilage. Arch Histol Cytol 1999; 2:149-63.
13. Hirano M, Sato K. Histological Color Atlas of the Human Larynx, 1a Edição. San Diego: Singular Publishing Group, Inc.; 1993.
14. Thawley SE. Surgical therapy of the larynx: surgical anatomy in Thawley SE, Panje WR, Batsakis JG, Lindberg RD. Comprehensive management of head and neck tumors. 2a Edição. W. B. Saunders Company; 1999.
15. Casiano RR, Ruiz PJ, Goldstein W. Histopathologic changes in the aging human cricoarytenoid joint. Laryngoscope 1994; 104: 533-8.
16. Chiewitz S. Untersuchungen über die veränderungen der menschlichen kehlkopfknorpel. Arch f Anat u Entweklngsgesch 1882; 303-49.
17. Strek P, Skawina A, Petri M, Olszewski E, Nowogrodzka-Zagorska M, Waloch J. The investigations of mechanical properties of ossificationg thyroid cartilages of the human larynx. Folia Morphol (Warsz.) 1993; 52:39-46.
18. Hately W, Evison G, Samuel E. The pattern of ossification in the laryngeal cartilages: a radiological study. Brit J Radiol 1965; 38: 585-91.
19. Vastine II JH, Vastine MF. Calcification in the laryngeal cartilages. Arch Otolaryngol 1952; 55:1-7.
20. Sakai F, Gamsu G, Dillon WP, Lynch DA, Gilbert TJ. MR Imaging of the larynx at 1.6 T J Comp Assist Tomogr 1990; 14:60-71.
21. Kavanagh KT, Salazar JE, Babin RW. Bone marrow expansion of the thyroid cartilage: A source of confusion with malignant invasion in CT studies. J Comp Assist Tomogr 1985; 9:177-9.
1 Master in Health Sciences, Hospital Heliópolis HOSPHEL, Sao Paulo.
2 Ph.D. in Medicine, Course of Post-graduation in Otorhinolaryngology and Head and Neck Surgery, Federal University of
Sao Paulo - Escola Paulista de Medicina, Sao Paulo. Professor, Course of Post-graduation in Health Sciences, Hospital Heliópolis HOSPHEL, Sao Paulo.
3 Master in Clinical Pathology, Federal University of Sao Paulo - Escola Paulista de Medicina, Sao Paulo;
Head of the Service of Clinical Pathology, Hospital Ana Costa, Santos.
4 Full Professor in Head and Neck Surgery, University of Sao Paulo. Coordinator of the Course of
Post-graduation in Health Sciences, Hospital Heliópolis HOSPHEL, Sao Paulo.
Course of Post-graduation in Health Sciences, Hospital Heliópolis HOSPHEL, Sao Paulo.
Address correspondence to: Walter Paiva Cruz - Rua Dr. Olinto Rodrigues Dantas 343 cj. 62 Santos SP 11050-220
Tel (55 13) 3232-9292 - Fax (55 13) 3237-6375 - E-mail: wpcruz@uol.com.br
Article submitted on March 28, 2003. Article accepted on September 11, 2003.

Print: ![]()