

Year: 2003 Vol. 69 Ed. 4 - (6º)
Artigo Original
Pages: 472 to 478
 PDF PT
PDF PT Study of demographic, ocupacional and co-carcinogenetics factors in squamous cell carcinoma of base of the tongue in women
Author(s):
Francisco S. Amorim Filho1,
Josias de Andrade Sobrinho2,
Abrão Rapoport2,
Marcos B. Carvalho2,
Neil F. Novo3,
Yara Juliano3
Keywords: base of the tongue, squamous cell carcinoma, alcohol, tobacco, female
Abstract:
Assess the relation between risk factors and squamous cell carcinoma of the tongue in women. Study design: Retrospective non randomized. Objective: Determine the relation between ocupacional history, risk factors (alcohol and tobacco), demographic variables and squamous cell carcinoma of the base of the tongue in women. Material and Methods: retrospective non randomized study in 31 files of women with squamous cell carcinoma of the base of the tongue at the Head and Neck Surgery and Otorhinolaryngolology of Hospital Heliópolis, São Paulo, from 1977 to 2000. Etnic, distribuition, age, occupational activities, tobacco, alcohol, consuption main sympton, interval between the first sypmton and the diagnosis and stage (TNM) were assessed, about statistics, were employed Kappa and Mc Nemar tests. Results: About etnic distribuition, white (58,1%), black (35,5%) and yellow (6,4%), with age ranging from 50 to 59 years, house keeper (83,9%), agriculture workers (6,4%), industry (3,2%), trade and superior level (3,2%). Concerning risk factors, tobacco alone (48,4%) both (45,2%) and none (6,4%). As symptoms, odinophagia (48,4%), neck node (19,3%), disphagia (12,9%), earache (9,7%), tongue wound (6,4%) and hoarseness (3,2%). For TNM stage, T3-4 (74,1%), T1-2 (25,8%), N0 (29,0%), N1 (29,0%), N2-3 (42,0%). Conclusions: Squamous cell carcinoma in women occured with prevalence of the at 6th decade, in white patients, with main symptons as odinophagia and neck node metastasis. In T3 and T4 patients, it was detected the predominance of tobacco, with neck metastasis at the first consultation.
![]()
INTRODUCTION
One of the most important elements related to cancer development, especially of the head and neck, is associated with environmental factors, especially those related to life style. Carcinogenesis can be induced by a combination of factors such as consumption of alcohol, smoking, diet aspects, occupational factors, viral infection, immune factors and genetic affections1, being that the association between alcohol abuse and smoking is the dominant risk factors in people with upper digestive tract cancer, specially of the oropharynx 2-8.
As of the 60's, the inclusion of women in the work force determined a change in social habits (increasing the intake of alcohol and smoking) and consequently the exposure to carcinogenic factors. Thus, it is estimated that there are 800 million smokers in the world and 250 million are females, justifying the significant increase of squamous cell carcinoma of the mouth and oropharynx. In Brazil, there are approximately 36.5 million smokers, being that 40.4% are women. Women became the target audience of the smoking industry and a significant portion of the society started to smoke. We should emphasize that this practice has been associated with the consumption of alcohol beverages encouraged by the large companies that increase production yearly. Such facts resulted in the universalization of the risk factors and modification of the epidemiological profile of the neoplasia, leading to reduction of cancer proportion between male and female subjects9.
Considering the increased incidence of cancer of the oropharynx between women in the past decades, many authors are unanimous to state that male subjects are still the most affected by oropharynx tumors, presenting greater proportion if compared to female patients 1, 3, 4, 10-12.
Despite the rarity of squamous cell carcinoma of the base of the tongue (1%) in Brazil and in the world 7, 13, it is an anatomical site that is predominant in the oropharynx when we consider its frequency compared to the tonsil and the posterior pharyngeal wall8.
Therefore, we tried to define a retrospective study in which the possible correlation between demographic, occupational and co-carcinogenic variables was considered, based on the new world epidemiology.
MATERIAL AND METHOD
We conducted a retrospective study of 31 cases of patients with squamous cell carcinoma of the base of the tongue, female subjects, diagnosed at the Department of Head and Neck Surgery and Otorhinolaryngology, Hospital Heliópolis, Sao Paulo, in the period between December 1977 and July 2000, and only the cases in which the lesion was primarily on the base of the tongue and that at the biopsy, the diagnosis of histology was squamous cell carcinoma.
We checked demographic variables (race, age), occupation, life habits (smoking, alcohol abuse), and we considered alcohol abuse and smoking by such patients in two different decades (as of 1980 in group 1 and as of 1990 in group 2). We analyzed the main complaint, interval of time between the onset of symptoms and the first medical visit, and clinical staging of the disease.
All patients were examined with routine examination, emphasizing the local-regional physical examination that comprised anterior and posterior rhinoscopy, oroscopy, indirect laryngoscopy, bi-digital palpation of the base of the tongue and palpation of the neck. All the data were transcribed to the medical charts associated with detailed anamnesis and personal information of patients collected on the first visit.
As to race, they were classified as Caucasian, Afro-descendent, or Asian-descendent and grouped according to age range after the 4th decade, being that the patients aged over 80 years were considered as a single group. As to main complaint and duration of complaint, we based on the main symptoms that motivated the patient to come to the physician, being the time interval between onset and first care defined in months.
As to occupational history of the patients, we divided them into four groups: agriculture, industry (inhaling agents, wood, chemicals, mechanics) trade and professionals or housewives.
As to life habits, we analyzed smoking and alcohol abuse based on crosses, as standardized in our department, according to the information provided by patients when they came to the first visit:
1. No smoker (-);
2. Smoker: 0 to 10 regular cigarettes, 2 home-made cigarettes, 2 pipes, 2 cigars as (+), and consequently, 11 to 20 cigarettes (++), 21 to 40 (+++), 41 to 60 (++++) and corresponding multiples for different types of smokers.
3. Non alcohol user (-);
4. Alcohol user: (+) for each dose of distilled drink, 1 bottle of beer, and 1 bottle of wine every day. Multiples (++) for 2 doses, 2 bottles of beer and 2 bottles of wine per day, and so forth.
Finally, based on the description of the lesion and its registration in the medical charts, as well as the presence or absence of regional or distant metastasis, the disease stage was reclassified using the TNM system (UICC - 1998) to stage the squamous cell carcinoma.
To statistically analyze the results, we used tests taking into consideration the nature of the studied variable:
1. Kappa Concordance Test (Landis; Kock 1977). In order to study the concordance between grade of alcohol consumption and smoking among women in stage T4 and housewives.
2. McNemar test (Remington; Shork 1970), as a complement of Kappa test, was used to compare the frequency located above or below the concordance diagonal.
In all of them we determined the level of null rejection hypothesis of 0.05 or 5%, marking (*) for the significant values.
RESULTS
Squamous cell carcinoma of the base of the tongue showed greater incidence in Caucasian (58.1%) patients , followed by Afro-descendent patients (35.5%), and there were few Asian-descendent cases (6.4%). Out of the 31 analyzed cases of squamous cell carcinoma of the base of the tongue in women, 14 were diagnosed in the 80's and 17 were diagnosed in the 90's. As to age of patients, we detected the highest incidence in the 6th decade of life (table 1). As to occupation, most of them were housewives (83.9%), followed by other jobs related to agriculture (6.4%), industry (3.2%), trade and professionals (3.2%).
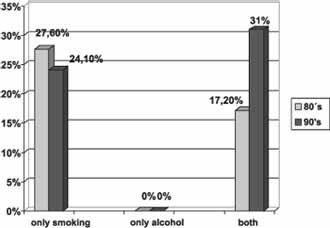
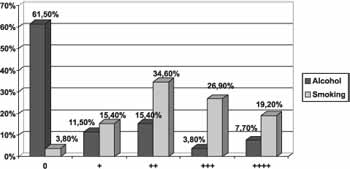
As to life habits (smoking and alcohol abuse), we found a higher frequency of isolated smoking (48.4%), followed by both habits (49.2%) and none of them (6.4%). Analyzing separately smoking and alcohol abuse between women in two different decades (80's and 90's) we could observe that in the 90's women started to associate more alcohol use with smoking (Figure 1).
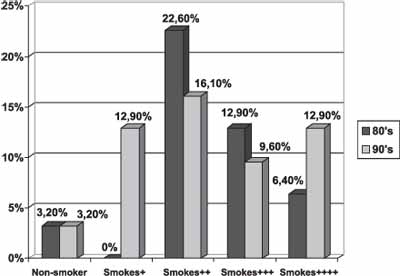
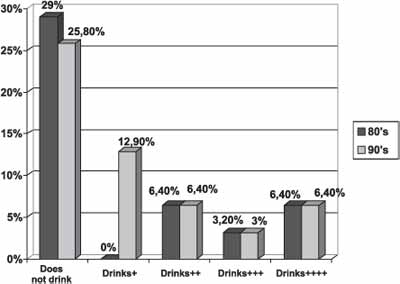
Analyzing the specific amounts of smoking and alcohol intake by women in the two decades, we found increase in daily smoking in the latter decade (Figure 2), as well as considerable increase in alcohol use in smaller quantities (social alcohol intake) (Figure 3).
Upon correlating alcohol intake and smoking in our patients and the most frequent occupation of housewife, we observed that it was more common to find large number of cigarettes smoked associated with little alcohol intake (Table 2).
There was no significant correlation in the Kappa test, showing that there is no direct correlation between the habits. Conversely, the McNemar test proved to be statistically significant smoking in association with small amounts of alcohol in this group. We observed that half of the subjects did not drink alcohol, but the association of both factors was present (Figure 4).
As to the main complaint, women related as the most frequent odynophagia (48.4%), followed by neck lump (19.3%) and dysphagia (12.9%), otalgia (9.7%), tongue wound (6.4%) and hoarseness (3.2%). The interval between initial symptom and first medical visit was of 6 months, and there were no statistically significant differences in the analysis of the variable in different decades (80's and 90's). Among the patients in group one (diagnosed in the 80's), this interval was present in 35.5% of the cases, whereas in the second group (diagnosed in the 90's), interval between initial symptoms and first medical visit of 6 months was 38.7%, with few cases diagnosed over 6 months, being 9.6% and 16.10%, respectively.
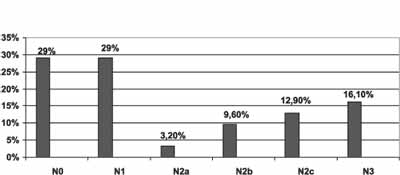
As to TNM classification (UICC-1998), a large proportion of the patients (54.8%) presented advanced stages of the tumor on the first visit (T4) and clinically positive lymph nodes on the neck (71%) (Figures 5 and 6).
When we correlated amount of alcohol intake and smoking by the patients and the advanced stage of tumors (T4) using Kappa and McNemar tests, we obtained the results described in Table 3. We noticed that in the first test, there were no statistically significant responses, whereas in the second one, it was more frequent and statistically significant to smoke a lot associated with little or moderate intake of alcohol.
Table 1. Patients with squamous cell carcinoma of the base of the tongue according to age in years.
Table 2. Patients with squamous cell carcinoma of the base of the tongue according to alcohol consumption and smoking versus professional occupation (housewife).
Kappa Test
Kw = 0.04 (concordance quotient)
Z= 0.56 (not significant)
Table 3. Patients with squamous cell carcinoma of the base of the tongue according to alcohol consumption and smoking versus tumor staging (T4).
Kappa Test
Kw = 0.20 (concordance quotient)
Z= 3.39 (Not significant)
McNemar test
X2 = 6.40 (p< 0.001)
Diagonal concordance = 41.18 %
Over the diagonal = 52.94% (represents greater amount of smoking)
Below the diagonal = 5.88% (represents greater amount of alcohol consumption)
Figure 1. Female patients with squamous cell carcinoma of the base of the tongue, concerning life habits in the 80's and 90's.
Figure 2. Female patients with base of the tongue squamous cell carcinoma concerning smoking in the 80's and 90's.
Figure 3. Female patients with base of the tongue squamous cell carcinoma according to alcohol intake in the 80's and 90's.
Figure 4. Housewives with base of the tongue squamous cell carcinoma according to alcohol intake and smoking.
Figure 5. Female patients with base of the tongue squamous cell carcinoma according to size of the primary tumor.
DISCUSSION
Internationally, the proportion of cancer in men and women has been decreasing since the end of the 60's, with visible increase of new cases of mouth and pharynx cancer among women since the end of the 80's 14. In search for opportunities in the job market, women became more exposed to carcinogenic factors. Their social habits have also been modified, and in the search for equal rights between men and women, they ended up incorporating habits that were frequent only to men, such as smoking and drinking alcohol.
As to race, more than half of our patients were Caucasian (58.1%), predominant in accordance with the literature 2, 15, despite the report of increase alcohol consumption among African descendents, who are more subject to oropharyngeal cancer 16.
As to age, our patients presented an incidence of 38.7% in the 6th decade of life. This result was similar to the findings of the literature that showed an increased incidence of patients with squamous cell carcinoma of the base of the tongue in the age range of 5th to 6th decade 10, 15, 17. Oral cavity and oropharynx cancer in young people is rare (in our study there was no case below the age of 30 years) and if present, female subjects are more affected. Young patients with oral cavity or oropharynx squamous cell carcinomas are more susceptible to the harmful effects of alcohol abuse and smoking, which is possibly related to genetic disorders or immunodeficiency 18, 19.
Considering the occupation of the subjects, 26 of them were housewives, a fact that is confirmed by the literature that states that occupation is not correlated with the genesis of mouth, pharynx and larynx cancer20, 21. Other authors 22 confirmed that only 5% of all deaths by cancer should be associated with occupational factors, being a small risk for the general population. As to involvement of women in out of home activities, there was a greater risk - 3 times greater, of mouth and pharynx cancer among operators of automotive machines, painters and agriculture workers, but those findings are based on small samples 15.
We believe that most of our patients with base of the tongue squamous cell carcinoma are still housewives that maintain home chores. They are not exposed to chemical carcinogenic elements from the industry, so the occupational factors are not important in the genesis of the neoplasm in our sample. Our study showed that the most evident and common life habit among them was smoking, isolated in 48% or associated with alcohol intake in 45.2% of them, showing that smoking is a predominant risk factor among them, with no cases of isolated alcohol abuse (Figure 1).
Upon assessing the behavior of women concerning life style of alcohol consumption and smoking in different decades, we found a significant increase in the association of these two risk factors in the 90's. The woman in the 80's that only smoked modified her behavior in the 90's and started also to take alcohol drinks, increasing her risk of developing base of the tongue squamous cell carcinoma. The percentage of women that associated alcohol use and smoking to their life style practically doubled in the 90's compared to the previous decade (Figure 1). Considering the amount of smoking made by these patients in the specific decades, we found an increase in the daily intake in the 90's, that is, the 80's most women were present in the smokers group (++). For the next decade, most of them started to smoke 40 cigarettes a day (++++) and it doubled compared to the previous decade (Figure 2).
Based on the same analysis with amount of alcohol intake in both decades, we observed that in the 90's, there was an increase in the number of subjects that started to intake alcohol daily (Figure 3). Women are going through changes in social behavior, equal to men not only in the professional field but also concerning life habits, because in recent years they are smoking and drinking alcohol even though it is still in smaller proportions than men.
When we correlate professional occupation and life habits of patients using McNemar test, we observed that for the group of housewives (greater number of cases), smoking was significantly more frequent than alcohol intake, that is, smoking is associated with little alcohol intake. We believe that the occupation does not seem to influence the risk factor in the genesis of base of the tongue squamous cell carcinoma, even in patients less exposed to external carcinogenic factors, such as housewives. We believe that the life habits of these patients are important risk factors for the development of base of the tongue squamous cell carcinoma. In the case of women, smoking is the most important risk factor in the genesis of the tumor and the association with alcohol (the most evident in recent years) seemed to contribute to increase the number of new cases of base of the tongue cancer. Alcohol can play a local synergic effect, acting as a solvent, facilitating the action of tobacco and carcinogenic elements in susceptible tissues 23.
As to symptomatology, women with neoplasia reported pain upon swallowing (odynophagia) in 48.8% of the cases, followed by lump in the throat in 19.3%, in accordance with the literature 24, 25.
As to the intervals between onset of symptoms and first medical visit, most of them were within 6 months, with few cases diagnosed after this period. Analyzing the data in different decades (80's and 90's) we did not observe statistically significant differences among them. Even with the advance of technology and early diagnosis in current days, our patients continued to be diagnosed within the same period as before. It can be explained by the fact that the initial symptoms of squamous cell carcinoma of the base of the tongue are late and when present, the tumor already has an advanced stage.
As to TNM classification, a large number of our patients presented advanced stage primary tumor (T4) and clinically positive neck (N+) (Figures 5 and 6) at diagnosis. This fact showed that the tumor is oligosymptomatic at the disease onset, grows in silence, is aggressive both in men and women and is diagnosed late, since we did not have any case of stage 1 tumor (T1). In our sample, the women presented at diagnosis clinically positive neck in 71% of the cases (Figure 6), in accordance with the literature 26.
Upon assessing the amount of alcohol intake and smoking, the 17 patients with advanced stage (T4) studied by McNemar test, showed more frequent and statistically significant smoking and intake of moderate amounts of alcohol, being that smoking was the predominant risk factor in the group. In our sample, smoking presented higher relation with base of the tongue cancer than alcohol among women. Women continue to smoke more than to drink alcohol. However, we should also take into account the importance of alcohol in the genesis of this neoplasm, especially when associated.
CONCLUSIONS
Squamous cell carcinoma of the base of the tongue in women is more frequent in the 6th decade of life, in Caucasian patients and odynophagia was the most common symptom. Smoking was predominant over alcohol intake, and in past years, the association with alcohol abuse became more evident and common in almost all women, as well as alcohol consumption daily. Most of the malignant tumors (squamous cell carcinoma) of the base of the tongue in women are in advanced stages (T3, T4, N+) on the first visit. The study clearly showed that extensive lesions are predominant in the base of the tongue tumors in housewives in which smoking was more frequent than alcohol intake.
REFERENCES
1. Boffetta P, Merletti F, Magnani C, Terracini B. A population-based study of prognostic factors in oral and oropharyngeal cancer. Oral Oncol Eur J Cancer 1994; 30:369-73.
2. Carvalho MB, Kanda JL, Andrade Sobrinho J, Kowalski LP, Rapoport A, Fava AS, et al. Estudo clínico dos tumores malignos da orofaringe. Rev Bras Cir Cab Pesc 1985; 9:13-27.
3. Day GL, Blot WJ, Austin DF, Bernstein L, Greenberg RS, Preston-Martin S et al. Racial differences in risk of oral and pharyngeal cancer: alcohol, tobacco and other determinants. J Natl Cancer Inst 1993; 85:465-73.
4. Franco EL, Kowalski LP, Oliveira BV, Curado MP, Pereira RN, Silva ME et al. Risk factors for oral cancer in Brazil:a case control study. Int J Cancer 1989; 43:992-1000.
5. Schantz SP, Harrison LB, Forastiere AA. Oral cavity and oropharyngeal cancer. In: De Vitta Jr VT, Hellman S, Rosenberg SA, eds. Cancer: principles and practice of oncology. 5th ed. Philadelphia: Lippincott-Raven; 1997.
6. Gonçalves Leite IC, Koifman S. Revisão dos fatores de risco para o câncer de boca e faringe. Rev Bras Cancerol 1998; 44:317-25.
7. Seikaly H, Rassekh CH. Oropharyngeal cancer. In: Bailey BJ, Calhoum KH, Deskin RW, Johnson JT, Kohut RF, Pillsbury Iii HC et al. Head and Neck Surgery: Otolaryngology. 2nd ed. Philadelphia: Lippincott-Raven; 1998.
8. Kanda JL. Epidemiologia, diagnóstico, patologia e estadiamento dos tumores da faringe. In: Carvalho MB., ed. Tratado de Cirurgia de Cabeça e Pescoço e Otorrinolaringologia. São Paulo: Atheneu; 2001.
9. Rosemberg J. Tabagismo panorama global. Jovem Médico 2001; 1:14-7.
10. Kowalski LP, Franco EL, Torloni H, Fava AS, Andrade Sobrinho J, Ramos GHA et al. Lateness of diagnosis of oral and oropharyngeal carcinoma: factors related to tumor, the patients and helth professionals. Oral Oncol Eur J Cancer 1994; 30:167-73.
11. Azevedo ALR, Dias FL, Spada MV, Santos TCRB, Noronha LHR, Kligerman J et al. Levantamento epidemiológico sobre o câncer da boca e orofaringe do Serviço de Cabeça e Pescoço do Hospital do Câncer-INCA. Rev Bras Cir Cab Pesc 1996; 20: 5-12.
12. Plasencia JD, Ramella ET, Ravello JÁ, Gavidia CG, Abanto WC, Acosta RV. Carcinoma epidermóide de cavidad oral y orofaringe. Diagnostico 1996; 35:14-21.
13. Mirra AP, Franco EL. Cancer mortality in São Paulo-Brazil. São Paulo: Instituto Ludwig for Cancer Research; 1987. (Cancer Epidemiological Monograph Series, v.3).
14. González Borrell A, Luis MN, González AMG. Mortalidad por tumor maligno de la cavidad bical y la faringe.Cuba,1968-1987. Rev Cubana Salud Pub 1990; 16:151-65.
15. Huebner WW, Schoenberg JB, Kelsey JL, Wilcox HB, Mclaughlin JK, Greenberg RS et al. Oral and pharyngeal cancer and ocupation: a case control study. Epidemiology 1992; 3:300-9.
16. Blot WJ, McLaughlin JK, Devesa SS, Fraumeni Junior JF. Cancers of the oral cavity and pharynx. In: Schottenfeld D, fraumeni Junior JF, eds. Cancer epidemiology and prevention. 2nd ed. New York: Oxford; 1996.
17. Dicker A, Harrison LB, Picken CA, Sessions RB, O'Malley BB. Oropharyngeal cancer. In: Harrison LB, Sessions RB, Kihong W Eds. Head and neck cancer: a multidisciplinary approach. Philadelphia: Lippincott-Raven; 1999.
18. Son YH, Kapp DS. Oral cavity and oropharyngeal cancer in a younger population: review of literature and experience at Yale. Cancer 1985; 55:441-4.
19. Lipkin A, Miller RH, Woodson GE. Squamous cell carcinoma of the oral cavity, pharynx and larynx in young adults. Laryngoscope 1985; 95:790-3.
20. Vogler WR, Lloyd JW, Milmore BK. A Retrospective study of etiological factors in cancer of the mouth,pharynx and larynx. Cancer 1962; 15:246-58.
21. Blitzer PH. Epidemiology of head and neck cancer. Semin Oncol 1988; 15: 2-9.
22. Kowalski LP, Nishimoto, I. Epidemiologia do câncer de boca. In: Parise Junior O, ed. Câncer de boca aspectos básicos e terapêuticos. São Paulo: Sarvier; 2000.
23. Macsween RNM. Alcohol and cancer. Br Med Bull 1982; 38:31-3.
24. Durazzo MD, Magalhães RP, Tavares MR, Cernea CR, Cordeiro AC. Diagnostico e tratamento do câncer da faringe. Rev Med São Paulo 1998; 77:143-8.
25. Carter RL, Pittam MR, Tanner NSB. Pain and dysphagia in patients with squamous carcinomas of the head and neck: the role of perineural spread. J Royal Soc Med 1982; 75:598-606.
26. Weber PC, Myers EN, Johnson JT. Squamous cell carcinoma of the base of tongue. Eur Arch Otorhinolaryngol 1993; 250:63-8.
1 Master degree, Course of Post-graduation in Head and Neck Surgery, Hospital Heliópolis, Sao Paulo.
2 Surgeon, Department of Head and Neck Surgery and Otorhinolaryngology, Hospital Heliópolis, Sao Paulo.
3 Faculty Professor, Department of Collective Health, Medical School, Universidade de Santo Amaro.
Address correspondence to: Prof. Dr. Abrão Rapoport - Rua Iramaia nº 136 Jd. Europa 01450-020 Sao Paulo SP
Tel (55 11) 273-8224 - E-mail: cpgcp.hosphel@attglobal.net
Article submitted on November 14, 2002. Article accepted on July 01, 2003.
Print: ![]()