

Year: 2001 Vol. 67 Ed. 5 - (19º)
Relato de Casos
Pages: 727 to 730
Mucormycosis of the paranasal sinuses and orbit in a immunocompetent patient: A case report and review of the literature
Author(s):
Nícia O. R. Santana 1,
Gustavo B. Pinheiro 2,
Helga M. Kehrle 3,
Isnaldo P. de Faria 3,
Cláudio N. Estrella 4
Keywords: mucormycosis, rhinocerebral phicomycosis and sinusal fungal infections
Abstract:
Rhinocerebral Mucormycosis is an invasive fungal infection initiated in the paranasal sinuses that frequently progresses to orbital and brain involvement. Rhino-Orbital-Cerebral Mucormycosis is usually associated with a poor prognosis and is almost exclusively seen in immunocompromised patients. The autors present a case of an immunocompetent female patient, 41 years old, with sinusal and orbital signs and symptons. The diagnosis of Mucormycosis was based on radiological study, surgical findings and culture. Now, that patient is being looked after in the ambulatory of the Hospital de Base do DF.
![]()
INTRODUCTION
Mucormycosis is a fungal, opportunist and fulminating infection that affects especially debilitated or immunodepressed hosts; it is very rare in healthy subjects.
REVIEW OF LITERATURE
The infection is commonly associated with acidotic patients, especially those patients with diabetic ketoacidosis. The disease my be caused by two groups of fungi: Mucorales, wchih affect debilitated and immunocompromised patients, and Entomophtorales, which affects healthy subjects and has a chronic progression. Even in immunodepressed patients, zicomycosis is a rare opportunist infection. Clinically, it may manifest through six different entities. Rhinocexebral zicomycosis is the most frequent presentation, amounting to more than 75% of all cases reported in the literature, and it is one of the fungal diseases most quickly fatal. Hyphae invade the paranasal sinuses and palate, extending into the ethmoidal sinus, retro-orbital region and/or central nervous system (CNS). Epistaxis, severe headache, alterations of mental state and ocular affections are part of the clinical picture. Examination of the nose reveals necrosis of the nasal cavities. Ocular findings include proptosis, periorbital edema, loss of sight, and palpebral edema, progressing to exophthalmia, complete ophthalmoplegia, blindness and dilated and fixed pupils. Diagnosis depends on direct examination and pathology of scrubs, followed by biopsy of the necrotic material. The treatment is based on early diagnosis, with aggressive surgical debridment and therapy with systemic amphotericin. It has a reserved prognosis, since rhinocerebral zicomycosis has a mortality rate of about 50%.
CASO REPORT
L. B. P., Caucasian, 41-year-old female patient, born in Ouro Preto /RO, was admitted in the emergency room of HBDF with a history of left otalgia for 45 days. The pain started after the removal of an insect from the ear. After 5 days, she experienced high fever, severe holocranial headache, neck rigidity, right peripheral facial paralysis, pain and ocular hyperemia. She was hospitalized in her own hometown for 40 days, treated for meningitis. However, the ocular picture worsened progressively, manifesting proptosis (Figure 1), facial edema and purulent discharge through the mouth, transferred then to our hospital. The patient had good health before the episode and did not refer systemic diseases, such as diabetes mellitus, pneumopathies or recurrent infections and use of immunosuppressant drugs. At examination, she presented drainage of purulent secretion in the region of pre-molar and canine teeth, extra-oral fistula, bilateral amaurosis, rettin necrosis, neck rigidity and peripheral facial paralysis.
Figure 1. Photo of the patient, after hospitalization at HBDF.
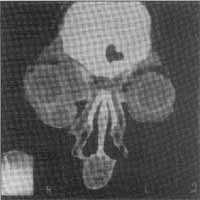
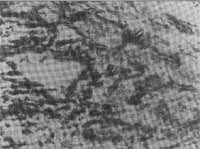
At nasofibroscopy, we observed darkened color of superior and middle turbinates and roof of the nasal fossa. Laboratory analysis revealed normocytic and normochronic anemia, leukocytosis with no deviation to the left, mild hyponatremia and hypocalcemia, normal renal function tests, glucose and transaminase levels. Serum IgG was slightly increased, IgA was normal and HIV serology was negative. Paranasal sinuses x-rays showed partial opacification of all sinuses. Orbit and cranial CT scan (Figures 2 and 3) showed multiple orbital and soft facial tissue abscesses, pansinusitis, obliteration of bilateral orbital fat with two hypodense condensations; measuring about 2cm on the right orbit and diffuse thickness of extra-ocular muscles. Thorax x-ray was normal. The suggested treatment was partial maxillarectomy and bilateral ethmoidectomy, removal of teeth 14, 15 and 16, medium meatotomy and orbitotomy, with removal of necrotic and purulent material from the areas. The result of pathology revealed zicomycosis (Figure 4), starting the administration amphotericin B (1mg/Kg/day), imipeneme and clyndamycin. The patient developed osteomyelitis of the skull base and head, presentation of soft part density in the x-ray, suggesting acute inflammatory process that occupied the orbital cavities, infra-temporal fossae, paranasal sinuses and middle ear structures. The neurosurgery department refused to approach surgically the base skull bones. We interrupted the previous antibiotic therapy and started the administration of cefpirome and metronidazole.
Figures 2 and 3. CT scan showing abscess in the orbits and naso-sinusal alterations.
We conducted a new surgical exploration of paranasal sinuses and bilateral orbitotomy, with surgical debridment. The culture showed MRSA (Methicilin-Resistant Staphyloccocus Aureus), a pathogen commonly associated with patients submitted to prolonged hospital treatment, and the patient was treated with vancomycin for 28 days. She was discharged 6 months later and had improved palpebral edema and proptosis, amaurosis and facial paralysis, but still uses prednisone (5mg/day) and amphotericin B weekly.
DISCUSSION
Fungal sinusitis should be considered in all subjects who had chronic sinusitis. Invasive forms of zicomycosis normally affect immunocompromised people, especially those neutropenic, diabetic, with hemochromatosis and malnutrition, characterized by acute onset of cough, fever, nasal ulceration, epistaxis and headache. Although it is more common in immunecompromised patients, mucormycosis may occasionally affect healthy subjects. Signs of poor prognosis include facial necrosis, nasal deformity and hemiplegia. There are chronic cases of up to 20 years of evolution already described, together with cases of skull base osteomyelitis and cranial nerves paralysis. The treatment consists of surgical debridment of the invaded tissue, associated with chemotherapy with amphotericin B, since the fungus present, according to the literature, is not sensitive to azolic agents, even itraconazole. In the case described here, despite the fact that she developed skull base osteomyelitis with no room for surgical approach, the patient was submitted to a number of surgical procedures, hindering the precise definition of the fungus species. Although the patient presented clinical improvement, we decided to maintain a weekly suppressive treatment with amphotericin B, since it was not possible to make sure that the infection had been completely irradicated.
Figure 4. Histology of the material collected from the sinus lesion.
CONCLUSION
Mucormycosis is a rare opportunist infection with reserved prognosis that generally affects immunocompromised patients. The case reported here is interesting because the diagnosis was sinunasal and periorbital mucormycosis in a immunocompetent patient.
REFERENCES
1. BACKER, R.D. -The pathologic anatomy of mycosis: human infection with fungi actinomycetis and algae, Chapter 21. Springer - Verhag, New York, 1971.
2. CHICK, E.W. et. al. - Treatment of mucormy - cosis in rabbits with amphotericin B. Antibiot. Chemth, 8:394-7, 1958.
3. CUNDARI, M.C.; CAMPANA, D.R.; CEDIN, A.C.; GASEL, JJ.; IRIYA, Y. - Mucormicose Rino-órbito-cerebral. Rev. bras Otorrinolaringol., 53(3):96-101. 1987.
4. FINN, D.G.; FARMAR, J.C. - Chronic mucormycosis - Laryngoscope, 92.761-3, 1982.
5. KAMESWARAN, M.; AL.; WADEI, A.; KHURANA, P.; OKAFUR, B.C. Rhinocerebral Asperglllosis - J. Laryngoscope Otol., 10Cd(11):981-5, 1992.
6. MACARTHUR C. J.; LINDEBECK E.; JONES D.T. - Paranasal phycomycosis in the immunocompetent host - Otolaryngol. Head Neck Surg., 107(3):460-2, 1992.
7. PARFEY, N.A. - Improved diagnosis and prognosis of mucormycosis: A clinicopathological study of 33 cases - Medicine 65.113-23, 1986.
8. PENNISI, A.K. - Paranasal sinus mucormy - cosis in a immunologically competent host - Am. J. Otolaryngol. 6471-3, 1985.
9. PEREIRA, E.A.; STOLZ, D.P.; PALOMBI-NI, B.C.; SEVERO, L.C. Atualização em sinusite fúngica: relato de 15 casos - Rev. bras Otorrinolaringol., 63(1):48-54, 1997.
10. RIOS-GONÇALVES, A. J. - Mucormicose (zigomicose) rinocerebral. Apresentação de dois casos com sobrevida. Arq. Bras. Med., 650(3):287 90, 1991.
11. WYNGAARDEN, J.B. - Cecil Textbook of Medicine, 407.1993-1945, ed. 192., 1992.
1 Resident Physician, Service of Otorhinolaryngology, Hospital de Base do Distrito Federal.
2 Assistant Physician, Service of Otorhinolaryngology, Hospital de Base do Distrito Federal.
3 Assistant Physician, Service of Otorhinolaryngology, Hospital de Base do Distrito Federal.
4 Head Physician, Sector of Head and Neck Surgery, Service of Otorhinolaryngology, HBDF and preceptor of Medical Residence, PRM-ORL, HBDF
Address correspondence to: Isnaldo Piedade de Faria - SQS 108 - Bloco D - Apt. 404 - 70347-040 Brasília/ DF
Tel: (55 61) 9982-2438 - E-mail: isnaldopf@uol.com.br
Study carried out at the Service of Otorhinolaryngology, Hospital de Base do Distrito Federal (SMHS 102 - Bloco B - Asa Sul) - 70335-9110 Brasília/ DF.
Article submitted on January 11, 2001. Article accepted on May 02, 2001.


Print: ![]()