

Year: 2001 Vol. 67 Ed. 5 - (12º)
Artigos Originais
Pages: 683 to 687
Stomatological manifestations of paracoccidioidomycosis
Author(s):
Júlio C. Bisinelli 1,
Flávio Q. Telles 2,
Josias A. Sobrinho 3,
Abrão Rapoport 4
Keywords: South american blastomycosis, paracoccioidioidomycosis, oral lesions
Abstract:
Study design: Clinical retrospective. Material and method: develop this research it had been realized a retrospective in reference book of 187 patients proceeding from the Infectology Service at the Deep Mycosis Ambulatory at Federal University of Paraná, in Curitiba, between may 1985 and march 1998. The purpose of this paper was to delineate the epidemic outline describing the stomatologicals manifestations found in the sample, to discuss about the data found and to establish comparison with the pertinent literature, to observe possible changes and if they were significant as well as to notice the dyes sensibility that were used in the histopathology (HE, PAS and GROCOTT), in 20 microscopic slides. It had been settled a previous protocol to get the data concerning to the desease epidemiology such as oral manifestations, describing the kind and localization of the lesions. In the results that were found, references like sex, age, naturalness, origien and profession of the patients were determinant factors in the epidemiologic and demographic outline of the sample studied (187 cases) compared with the pertinent literature. Results: The evaluation of the results showed changes that were not to much significant in relation to the desease epidemiology. On the other hand, it was evidenced the exuberance in oral manifestations of the desease that is very commom and frequently leads the patient to a worse condition or even to a maintenance of the desease by the difficulty of nutrition that increases the immunesuppression. In the sample of these 187 patients studied, 167 (89,3%) were male and 20 (10,7%) female. In relation to the age, 75 (40,1 %) were between 40 and 50 years, with some relevant aspects:81 patients (43,3 %) were agricultural workers, 93 (49,7 %) were from inland areas of Paraná. The loss of weight was related in 72 (17,22%) of the 187 complaints, followed dyspnea. In relation to the shape of the lesions, 85 (41,46%) of the patients did not show visible, the most commom were the ulcerated ones, the granulomatuos ones, followed by moriform one. The place with major incidence of lesions were lips, followed by oropharynx and hard palate, it was also noticed more than one kind of lesion in the same patient, between these 187 patients, five (2,65%) showed also tuberculosis, 140 (72,54%) did not palpable lymphonodes, 127 (67,91%) of the patients denied to use alcoholic drinks, 117 (62,57%) were smokers. The pulmonary envelopment was predominant in 166 (51,78%) of the analized cases. In the histopathology, the technique of dyeing by silver (GROCOTT) showed it self more sensitive than HE and PAS for visualization in demonstration of the etiologic agent P. brasiliensis.
![]()
INTRODUCTION
Paracoccidioidomycosis, also known as Brazilian blastomycosis, South-American blastomycosis or Lutz's disease, was observed for the first time in Brazil in 1908, by Adolpho Lutz, who was attracted by the lesions found in the mouths of some patients. It is a systemic mycosis caused by a dimorphic fungus, natural from Latin America, found especially in Brazil, Colombia and Venezuela.
In Brazil, the highest incidence is found in the South, Southeast and Center-West regions of the country. In Paraná, similarly to other Brazilian states, the disease is endemic among the rural population, and it is important from a public health viewpoint, since it affects people at the peak of their productive life. It is more frequently found among people in the 5th and 6th decades of life, normally men, and subjects who work in agricultural activities, despite the fact that it may affect both genders and also adolescents2,5,6,8,10,11,12,13,16.
The disease involves primarily the lungs by inhalation, and it may later spread to other organs and systems, causing secondary lesions that are frequently seen in mucosa, lymph nodes, skin and adrenal glands5,10,19.
The knowledge of paracoccidioidomycosis is of great interest to Stomatology, since until recently it was believed that the oropharynx was the entry point of the fungus, because of the large number of manifestations found in the region. For this reason, in most cases, the first signs and symptoms will take the patients to the dentist or otorhinolaryngologist office. Mouth and neck are important regions for the manifestation of the disease, since the mouth mucosa provides substrate for the saprophyte life of the fungus, in a protein-rich environment, in a region submitted to minimum temperature variations. In such environments, the fungi grow the micellar phase, producing conidia that survive for many months, enabling spread through the air.
If inhaled, they reach the pulmonary alveoli and originate the subclinical infection that may spread into other organs through lympho-hematogenic route14,17,18,23.
The most common clinical manifestation is chronic disease in male patients, affecting 10 men to one woman, aged between 30 and 50 years, usually smokers and/or alcohol abusers, living in poor social, economic and hygienic conditions, because low immunity favors the progression of the disease. The difference of incidence in both genders is attributed to hormonal factors. Paracoccidioides brasiliensis has -stradiol receptors in its cytoplasrnatic membrane, which prevents the transformation of the filament phase into yeast-like form. It is a consensus that in endocrinologically mature women with appropriate estrogen levels, infecting conidia are unlikely to be transformed into yeast, owing to the female hormonal protective effect7,8,20,22.
Lesions of oral, pharyngeal and laryngeal mucosa are very common and result from hematogenic spread, from the primary pulmonary focus. In the mouth, there is normally moriform stomatitis, as described by Aguiar Pupo15, also known as papullar-erosive stomatitis. It is slow progressing stomatitis, exulcerated, with aspect of thin red and multiple granulations (Photo 1). Sometimes, they may be presented as deeper ulceration (Photo 2). They predominantly affect lip regions of jugal mucosa, gums, tongue and palate; in addition to lesions, there is also pain, bleeding, teeth mobility, sialorrhea, and edema. The affection of larynx and vocal folds causes different degrees of dysphonia and aphonia. Initial lesions, especially on the tongue, may simulate a carcinoma.
Pathology is essential to reach a definite and differentiated diagnosis. Identification of etiological factor may be obtained by visualization of the yeast-like form phase of the fungus in material collected by scrub of the lesion, sputum or biopsy - obviously, the most reliable method. Different histology staining techniques are used, among them, hematoxylin-eosin (HE), Periodic Acid Schiff (PAS) and silver impregnation (Gomori-Grocott1,4,9,16,21).
Photo 1. Lesion with thin granulomatous aspect, with red dots on the upper lip and upper gum.
Photo 2. Ulcerated lesion on the lateral rim of the tongue, observing a thin granulomatous lesion in the lingual dorsum.
Owing to lack of compulsory notification and fully understanding of the epidemiology of the disease, our purpose was to compare the epidemiological and demographic profile of our cases to the literature in the area and to analyze the sensitivity of histology staining HE, PAS and Grocott.
MATERIAL AND METHOD
The studied sample comprised the review of 187 medical files of patients from the Ambulatory of Deep Mycosis, Service of Infectious-Contagious Diseases, Hospital das Clínicas da Universidade Federal do Paraná, from 1985 to 1988, including patients with oral paracoccidioidomycosis confirmed by biopsy of the lesions.
Clinical and demographic characteristics of patients were analyzed concerning place of birth, gender, age, address, occupation, hygiene habits, smoking, alcohol abuse, and dental conservation status, in order to define an epidemiological profile of the disease. We also took into account the physical examination and oral lesion description.
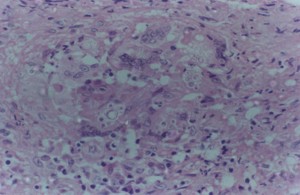
We prepared tables with the variables and the Service of Pathological Anatomy at Medical School of Universidade Federal do Paraná reviewed 20 cases of biopsy, staining the slides by the following methods: HE, PAS and Grocott, to detect Paracoccidioides brasiliensis (Photo 3).
Owing to the nature of the collected data, we carried out a descriptive statistical treatment, with distribution of frequency of the different variables analyzed in the study, using the software Epi-Info, which provided the statistical result. We did not apply statistical tests because the values found did not show statistical differences when compared to the data provided by the literature.
RESULTS
Out of 187 patients, 167 (89.30%) were male and 20 (10.70%) were female patients. As to age, we observed the highest frequency between the 4th and the 5th decades of life (Table 1).Table 1. Distribution according to age.
More than 50% of the patients (52.94%) were from the countryside region of Paraná, showing that this is an endemic region for the disease. Out of 187 studied medical files, 84 (44.03%) were of farmers (Table 2), who reported 376 main complaints, because some of the patients had more than one complaint. The most frequent one was weight loss, followed by dyspnea (Table 3).Table 2. Distribution according to occupation.Table 3. Distribution according to complaint.
As to location of mouth and pharyngeal lesions (Table 4), there was predominance of lip region in 58 cases (19.27%), followed by oropharyngeal affection in 42 cases (13.95%).Table 4. Distribution by site of lesion.
As to type of lesion, 85 (41.46%) patients did not present visible lesions. Among the visible lesions, the most frequent one was ulcerated lesion (24.88%) and granulomatous lesion (14,15%), followed by moriform lesions (7.80%) (Table 5).Table 5. Distribution by type of lesion.
Out of 187 patients, 164 (86.77%) did not present associated pathology. However, in 5 cases (2.65%), concomitant pulmonary tuberculosis was diagnosed. Another 5 cases (2.65%) had candidiasis and 140 (72.54%) did not present palpable lymph nodes and 47 (27.46%) had them in one or more region, especially on the cervical areas, bilaterally.
There were 127 (67.91%) of the patients who admitted alcohol abuse, whereas only 60 subjects (32.09%) said they definitely did not abuse of alcoholic drinks. As to smoking, 117 (62.57%) smoked and 11 (5.88%) did not respond to the question, plus 59 patients (31.55%) whose medical files did not provide information.
Out of 187 studied medical files, only 52.08% informed the dental conditions of patients. Among them, 23.33% had dentition at poor conservation status, and 28.75% had some kind of gingival problem.
Concerning distribution of lesions caused by the disease, some presented one or more local involvement. Pulmonary compromise predominated out of a total of 160 (51.78%) analyzed cases (Table 6).Table 6. Distribution of lesions.
DISCUSSION
Since it is not a compulsory notification disease, it is difficult to define the precise incidence of paracoccidioidomycosis in Brazil. Data concerning geographical and epidemiological distribution are fragmented. Its most common clinical form is the chronic lesion with progressive alteration of the general status, frequently affecting the lungs and the oral cavity. That is why otorhinolaryngologists and dentists should know about this mycosis, especially because polymorphism of its clinical picture hinders the diagnosis12.
In the results found for the present study, gender, age, place of birth and occupation were determinant factors for the description of the epidemiological and demographic profile of the disease, which was comparable with the literature's.
Out of 20 female patients, two (10.00%) were aged between 13 and 14 years, a phase in which sexual immaturity increases the incidence in this age range.
Out of 187 studied cases, we observed that most of them (52.94%) came from agricultural areas2,6,7,8,11, similarly to other literature reports.
The highest incidence of lesions in the lips, gums, palate and tongue were in accordance with the literature (Table 4).
The systemic lesions of the chronic form of mycosis, the lungs and lymph nodes, besides the oral. mucosa and the orhpharynx, were the most involved regions.
In our cases, there were 160 (51.78%) lung affections, 115 (37.22%) oral mucosa or oropharyngeal affection and 53 (27.46%) lesions that affected one or more lymph nodes, in agreement with the literature.
One hundred and seventeen (62.57%) patients were smokers. The high number of smokers indicated that there is a correlation between smoking and paracoccidioidomycosis, as reported by the literature. However, as to alcohol abuse, 127 (67.91%) reported that they did not abuse of alcohol, which is different from what had been reported in the literature. This fact could be explained by failure in asking questions or changes in the profile of our sample.
We revised slides of 20 cases and morphological identification with fungi count was positive in all of them, with staining of HE, PAS and Grocott (silver impregnation). The latter proved to be superior for the fungus of paracoccidioidomycosis, similarly to the studies that evaluated the sensitivity of Gomori-Grocott staining in scrubs from oral lesions by cytological analysis3.
This method detects the presence of glycogen and mucin, enabling release of aldehyde groups, resultant from the pre-treatment with chromic acid. Subsequently, there is the detection of the reduction of alkali complex by silver nitrate, since the cell wall is rich in polysaccharide. This phenomenon allows the observer to clearly and safely identify Paracoccidioides brasidiens4,9. It is a good technique because it is easy to identify and visualize the fungus, besides its low cost and easy execution3 (Photo 3).
As a result of the revision of the medical files, there could be problems when describing the mouth lesions concerning both site of lesion and multiplicity and morphological aspect. This finding showed that there are flaws in the clinical examination that should be solved in order to improve epidemiological studies. Despite these problems, we did not find a change in the epidemiological and demographic profile of our study, comparing with the literature.
Photo 3. Histological section representing granulomatous lesions that contain epithelioid cells and "foreign body" type giant cells among which we may observe rounded organisms, of various diameters, with double refringent capsule and lateral sprouting (HE, X400).
CONCLUSIONS
To sum up, we concluded that:
1. In the epidemiology of paracoccidioidomycosis, male farmers aged between 40 and 60 years, with poor oral hygiene, are considered a risk group;
2. The technique of silver staining (Grocott) showed high level of sensitivity at the histological analysis, proven to be more effective than HE or PAS.
3. Based on the great variety of oral lesions found in the sample, we suggest the development of multidisciplinary medical and dental teams in the risk regions to effectively contribute to diagnosis and treatment of these affections.
REFERENCES
1. ALMEIDA, O.P.; SCULLY, C.; BOZZO, L. - Oral manifestations of paracoccidioidomycosis (South American blastomycosis). Oral Surg. Oral Mad. Oral Pathnl.72:330-45, 1991.
2. ARAIJJO, N.S.; V.C. - Lesões da mucosa bucal por agentes biológicos, físicos a químicos. Patologia Bucal, 1 . ed. São Paulo: Artes Médicas., 53-5, 1984.
3. ARAQO, M.S. - Estudo epidemiológico de pacientes com paracoccidioidomicose crônica, com avaliação da sensibilidade do exame citológico bucal, utilizando a coloração de impregnação pela Prata (Gomori-Grocott). Dissertação (Mestrado). Faculdade de Odontologia da Universidade de São Paulo. 90p., 1999.
4. BANCROFT, J.D; STEVENS, A. - Theory and practice of histological techniques. 4. ed. Hong Kong: Churchill Livingstone., 300-2, 1996.
5. DEL NEGRO, G.; LACAZ, C.S & FIORILHO, A.M. - Paracoccidioidomicose sul-americana. São Paulo, Savier, 1982.
6. FONSECA, J.B. - Blastomicose Sul Americana. Estudo das Lesões dentarias a Paradentarias sob o ponto de vista clínico a histopatológico. São Paulo, 1957. (Tese de Livre Docencia). FONSECA, J.B. Blastomicose Sul- Americana. Estudo das lesões dentais a paradentais sob o ponto de vista clínico a histopatológico. Rev. Bras. Fac. Odont. São Paulo, 1:1-31, 1963.
7. FRANCO, M. - Paracoccidioidomycosis Ann Arbor, Boca Raton, 1994.
8. FRANCO, M. - Host-parasitic relationship in paracoccidioidomycosis. J. Med. Vet. Mucol. 4:187-217, 1989.
9. GROCOTT, R.G.A. - A stain for fungi in tissue sections and smears: using Gomori's methenamine - silver nitrate technique. Am. J Clin. Pathol., 25.,975-9, 1995.
10. KWON-CHUNG, K.G.; BENETT, J.E. -Medical Mycology. Pennsylvania, Lea & Febiger, 594-619, 1992.
11. LASCALA, T.; MOUSSALLI, H. - Periodontia Clinica II. Blastomicose Sul-Americana. Artes Médicas, 892-898, 1989.
12. LONI?ERO, A.T.; MELLO, I.S. - Paracoccidiodomicose. J. Bras. Med. 55(3):96-111, 1988.
13. MOCELLIN, L. et al. - Lesões no setor Otorrinolaringológico em Blastomicose Sul-Americana. An. Med. Uniu. Parand, 18:97-105, 1975.
14. NEGRONI, R. Pathogenesis. In: FRANCO, M.; LACAZ, C.S.; RESTREPO, A.; DEL NEGRO, G. - Paracoccidioidomycosis, Boca Raton: CRC Press., 203-12, 1994.
15. NOVA, R. & PAIVA, L.J. - Les6es orofaringeas. In: DEL NEGRO Paracoccidioidomicose, blastomicose sul-americana. São Paulo: Savier Edusp., 157-160, 1982.
16. ORTEGA, K.L.; OLIVEIRA, P.T.; MAGALHAES, M.H.C.G.; ARAUJO, N.S. - A citologia esfoliativa no diagn6stico da paracoccidioidonucose. R.P.G. 3:148-53, 1996.
17. PADILHA GONÇALVES, A. - Lymph node involvement. In FRANCO, M.; LACAS, C.S.; RESTREPO, A.; DEL NEGRO, J. - Paracoccidioidomycosis. C.R.S. Press, Boca Raton, 410:267-9, 1994.
18. RESTREPO, A. - The ecology of Paracoccidioides brasiliensis: a puzzle still unsolved. J Med. Vet. Mycol., 23:323-34, 1985.
19. RIPPON, J.W. Medical mycology. 3' ed. Philadelphia: W.B. Saunders Company., 506-31, 1988.
20. SALAZAR, M.E.; RESTREPO, A.; STEVENS, D.A. - Inhibition by Estrogens of conidium to yeast. conversion in the fungus Paracoccidioides brasiliensis. Infect Immun., 56.711-3, 1988.
21. VILLALBA, H. - Características microscópicas da Paracoccidioidomicose bucal. Piracicaba, 1998. Tese (Mestrado) Faculdade de Odontologia, Universidade Estadual de Campinas, Piracicaba. 85f.
22. WANKFS, B.; LONDERO, A.T - Epidemiology and Paracoccidioidomycosis. In: FRANCO, M.; LACAZ, C.S.; RESTREPO, A.; DEL NEGRO, G. Paracoccidioidomycosis, Boca Raton: CRC Press., 410:109-20, 1994.
1 Master in Head and Neck Surgery, Hospital Heliópolis, Hosphel, São Paulo
2 Ph.D. in Infectious-Parasitic Diseases, Hospital das Clínicas, Universidade Federal do Paraná
3 Ph.D. in Medicine, Hospital Heliópolis, Hosphel, São Paulo
4 Full Professor, Hospital Heliópolis, Hosphel, São Paulo
Study conducted at the Service of Infectious-Parasitic Diseases, Hospital das Clínicas, Universidade Federal do Paraná
Address correspondence to: Prof. Dr. Abrão Rapoport, Pça. Amadeu Amaral, 47 - cj. 82 - Paraíso, CEP - 01450-020 - Telefax (55 11) 273-8224. E-mail: cpgcp.hosphel@attglobal.net
Article submitted on March 13, 2001. Article accepted on April 20, 2001.


Print: ![]()