

Year: 2001 Vol. 67 Ed. 5 - (9º)
Artigos Originais
Pages: 661 to 670
Prevalence of hearing losses in workers in the hiring process of companies in the region of Campinas /SP
Author(s):
Eloísa S. Franco 1,
Ieda C. P. Russo 2
Keywords: hearing loss, worker's health, noise induced hearing loss
Abstract:
Introduction: The work is an eternal natural need, i.e., a process between man and nature. The disease is a biological process older than man. But in man, the disease has also another dimension: the social one. Aim: This study intended to determine the prevalence of hearing losses in workers in the hiring process of companies in the region of Campinas - S.P. Study design: Retrospective clinical. Material e method: The sample comprised 3,117 records of candidates to jobs offered in the industries of different segments in the region of Campinas - S.P. The selected companies were heterogeneous and featured as predominantly unhealthy environments. In order to survey the audiometric configuration of the workers, the audiometric results were evaluated by air conduction and bone conduction. Results: The results showed that 80.4% of the workers presented hearing within the normal standards and 19.6% presented audiometric change. Out of the workers that presented audiometric change, 5.7% presented conductive hearing loss; 65.7% sensorineural hearing loss; 0.7% mixed hearing loss, when we analyzed the right ear only and 7.9% presented conductive hearing loss; 79.7%, sensorineural hearing loss; 1.1% mixed hearing loss, when we analyzed the left ear only. Conclusion: We emphasize the importance of the audiologic work as to the implantation of programs for the prevention of hearing losses, in order to enable the worker's placement in the market without trouble.
![]()
INTRODUCTION
Many doors have closed to a large number of candidates considered inapt and were dismissed from their previous jobs. They face the situation of being prevented from joining a new company because of minor audiometric alterations; in some situations, they are also left unsupported by the welfare legislation16.
In deviation from its functions, pre- hiring physical examinations have been used to prevent people with hearing loss from getting a new job18. In some cases companies have admitted responsibility for the occupational, damage of its employees when a severe hearing loss is detected, as defined by social security, therefore granting them job stability and better working conditions. However, employees who do not meet these criteria are not able to reap the same benefits. The market is responsible for absorbing and reintegrating them into jobs, providing strict hearing preservation programs and preventing social-economic imbalance. This fact is perfectly visible when we see a candidate who gets a new job, regaining his self-esteem, the support of the family and the responsibility to guarantee dignity and hope for their dependents.
Market place
Work, a natural necessity, is a process in the relation of man and nature. It implies the process of social reproduction, with two moments of production and consumption, which form a unit. During work the worker not only transforms the product, but by doing so, he transforms himself.
Bosi5 defined that in its corporal and subjective character, work means the compulsory insertion of the subject in the system of economic and social relations. A job means not only a salary source, but also a place in the hierarchy of society made up of classes and status groups.
In Brazil, it is considered that work is part of citizenship. The unemployed is excluded from many social achievements and is at the disposal of goodwill and public charity14. Deprived from work, human beings many times feel degraded, lose their self-esteem and die.
Workers with hearing loss at hiring
In our country, the legislation in force requires the worker to be submitted to a pre-hiring physical examination. Among them, the results of pure tone audiometry are eventually used to select candidates at hiring. Testing is required by NR-7 PCMSO (Program of Medical Control of Occupational Health), from the Labor Ministry. The result of this practice is the existence of a large number of workers with hearing. loss of different degrees who can not be admitted and are prevented from being hired.
The National Committee on Noise and Hearing Conservation6, according to its bulletin No.3, suggested administrative and interventions for workers with noise induced hearing loss (NIHL). The Committee, based on previous tests, considers of little risk the hiring of workers with NIHL who had stabilized hearing thresholds and without clinical symptomatology; at the same time, they believe it is of high risk to hire workers with NIHL to jobs that are performed in noisy environments. Regardless of the existence of previous tests, the committee considers of high risk the hiring of workers with unilateral anacusia, even in the presence of contralateral normal hearing, to noisy positions. It also considers of high risk hiring worker with sensorineural hearing loss caused by other etiologies than noise, whose loss affects middle frequencies. Hiring of workers with hearing loss in companies in which there is no program of hearing conservation in place is also considered high risk.
Almeida and Resende1 pointed out that auditory curve suggestive of NIHL in the pre-hiring physical examination should not disqualify the workers from doing a professional activity. NIHL, in most cases, is not incompatible with work and should not necessarily exclude the; workers from labor life.
According to Kwitko18, undoubtedly, pre-hiring physical examinations indicate who are the individuals with hearing loss. Under such circumstances, the test should be used as a safeguard for the company in case of a labor lawsuit, or serve as information for the development of a hearing conservation program. Its use as a tool to qualify workers to different positions is a very debatable issue. If the result of the examination shows hearing loss, it will be interpreted as a hindrance for working in a noisy environment. The author concluded that a subject with NIHL should not be considered disabled to work both in absolute and universal terms. Disability, if present, should be regarded as a specific task performed under specific conditions, within a determined work environment. He emphasized, however, that workers whose jobs require appropriate hearing conditions - air and land traffic controllers, aircraft pilots, telephone operators, musicians and radio announcers, should be submitted to different kind of occupational examinations. The presence of hearing loss, followed by functional deficiency and other predisposing or aggravating factors, may suffice to characterize the disability to perform such activities.
Ferreira Junior11 stated that in various times, workers with NIHL, even with mild loss, had to interrupt their work because they were said to be incapable in carrying out their activities, even though their production performance was satisfactory. According to the author, this is a deviation of the objectives of occupational medicine, now trying to identify perfectly healthy individuals or those who are ultra-resistant.
Kwitkol18 noticed that normal hearing individuals also run the risk, in short, of developing a hearing loss. In addition, workers with preexisting hearing loss have to engage in the Hearing Conservation Program (PCA). Nevertheless, there are no reasons why the same program can not be provided to normal hearing individuals that share the same noise environment. The author claimed that there is no evidence that people with hearing loss will lose their hearing similarly to normal hearing people.
Ferreira Júnior11 considered that most employers are interested in having highly qualified workers on their payroll, even if they have hearing loss. He emphasized the importance of having good hearing conservation programs, which will keep highly skilled workers on their jobs even if they have NIHL, and with no further risk of aggravating the disease, and at the same time, preserving their occupational capacity. He wondered what kind of guarantee the physician had that the worker would keep his hearing unaltered throughout time. Therefore, hiring employees, especially to very noisy areas, should necessarily be followed by the implantation of a hearing conservation program to all workers, regardless of the presence of NIHL.
Etiologies of hearing loss
According to Fiorini13, there is a set of endogenous factors (characteristics of the individuals) that when added to exogenous factors (exposure to noise, vibration and chemical, among others), cause a series of health problems, among others, irreversible hearing loss.
The author emphasized that while the concern of exogenous factor exposure was directed to work environments, projects and measures were implemented to protect workers. However, there are some noisy activities beyond the work environment and NIHL should not be considered a work-related affliction any longer.
Noise is the occupational factor that most frequently causes hearing loss. However, other conditions should not be excluded, such as chemicals, ionizing radiation, accidents with cranial traumas, barotrauma and allergens.
To the Comite Nacional de Ruído a Conservação Auditiva7, in its Bulletin No.1, work-related hearing loss is a gradual decrease of hearing acuity resultant from the exposure to high levels of noise. It is characterized by being sensorineural, since the Corti's organs cells are affected. It is irreversible and almost always bilateral and rarely comes to be profound because it does not exceed 40dbHL in low frequencies and 75dBHL in high frequencies. Initially it is manifested predominantly by affecting the frequencies 6 kHz, 4 kHz or 3 kHz, and progressed to affecting 8 kHz, 2 kHz, 1 kHz, 0.50 kHz and 0.25 kHz. IT is a cochlear pathology and the person should present tinnitus and intolerance to loud sounds, plus compromise of speech intelligibility. Once exposure is interrupted, there is no further progression of the loss, and it is influenced by physical characteristics of noise, duration of exposure and individual susceptibility. NIHL may be aggravated by the simultaneous exposure to loud noise and other agents, such as chemicals and vibration. The use of ototoxic or the presence of some diseases may enhance the individual susceptibility to noise.
NIHL is not caused only by industrial noise, but also by daily life noises, called "sociacusia". Celeni et al.10 tested 27 common toys in order to determine sound levels produced by them. The results showed that some toys might lead to hearing loss, such as toy cars with alarms (fire engines, police cars and ambulances). Therefore, the authors concluded that our education is influenced by sound pollution. Rolla 26 conducted a study in Campinas/ SP, surveying noise levels in the city. The values were 72.5 dBHL; 75.7 dBHL; 71.7dBHL, in the main crossroads of avenues downtown and a mean of 76.3dBHL in the roads that came into town. In urban bus stations, noise levels were approximately 62.9dBHL, which showed that the main sources of noise in the city are the cars.
Exposure to non-occupational noise has been researched in different countries, including Brazil. Also, new leisure activities are very noisy - such as individual Walkman devices at loud intensity, rock/pop concerts, discos and car radio/CD systems. These are all part of the lives of young people who live in large cities and may lead to irreversible hearing loss27.
Nogueira23, in an article published in Veja/São Paulo, reported sound levels recorded in some places of the city of São Paulo, such as: a bus stop in the Anhangabau tunnel - 97dBHL, under the Minhocao expressway - 92dBHL, and the intersections between Av. Paulista and Av. Brigadeiro Luis Antonio - 83dBHL.
Sound pollution, considered by the World Health Organization as one of the three ecological priorities for the next decade, is not visible; and the perception of the problem sometimes takes longer.
The worse are individuals who are exposed to loud sound intensities, being the majority young people, and even before they start their productive life they may acquire a hearing loss.
Fiorini13 concluded that today, noise is part of our daily life (traffic and leisure noise, among others), and she suggested that NIHL could become one of the main chronic diseases of the future of humanity.
On the other hand, Sataloff29 listed- various pathologies that could generate hearing loss at 4kHz, such as noise induced hearing loss, viral infections (rubella, measles, mumps, herpes simples, cytomegalic inclusion and respiratory virosis). Also cranial rheumatism, hereditary hearing loss, ototoxicity (by aminoglycoside antibiotics, diuretic and chemotherapic agents, high dose aspirins, and other chemical products), acoustic neuroma, sudden deafness, multiple sclerosis, others (bacterial infections such as meningitis, endotoxin, neonatal hypoxia, jaundice). The author concluded that an audiogram that shows a fall in 4kHz alone is not enough evidence to diagnose noise induced hearing loss, requiring a complete and careful clinical history that excluded the possibility of other causes.
Almeida2 concluded in a study that because of metabolic and circulatory peculiarities, the inner ear is the target of different systemic diseases of common incidence in the population. It also results in sensorineural hearing loss with audiometric configuration similar to exposure to noise, for example, sickle cell anemia, syphilis, renal failure, epidemic parotiditis, measles, cytomegalic inclusion diseases, hypothyroidism, among others.
Upon analyzing the literature, we could observe that most of the studies conducted with workers concluded that there was a predominance of hearing loss in the workplace in more than 50% of the studied individuals12,21,22,24,25,30.
There is still a lot to add from the speech and hearing disorder area to the process of preserving workers' hearing. However, our study intended to plot the hearing profile of the applicant to job offers, contributing to the pre-hiring physical examinations but without masking the need to create an effective prevention program, enabling the applicant to be hired without further barriers.
In view of that, the objectives of the present study were:
1 To study the occurrence of hearing loss in workers who are undergoing the pre-hiring physical examinations in companies of the region of Campinas, São Paulo, according to PCMSO.
2. To describe the type of hearing loss of workers who had audiometric abnormalities.
MATERIAL AND METHOD
The present retrospective descriptive study is a result of the analysis of a database. It was carried out in a company that provides audiological services, among others, to occupational audiometric tests to industries in the region of Campinas, São Paulo. In order to have a reliable sample, we decided to select the pre-hiring physical examinations carried out from January 1997 to June 1999. We had access to identification and clinical files of applicants.
Characterization of sample
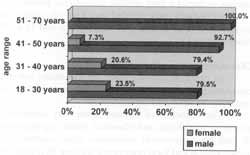
The sample consisted of 3,117 files of applicants for jobs in different types of companies in the region of Campinas, São Paulo. There were 2,462 male applicants and 655 female applicants, ranging in age from 18 to 70 years.
Since one of the purposes of the study was to characterize the auditory conditions of applicants to industrial positions, we did not exclude any subject in an attempt to depict a very reliable audiometric profile.
Individuals were divided into four age ranges: 18 to 30 years; 31 to 40 years; 41 to 50 years; and 51 to 70 years (Figure 1).
Characterization of companies
In order to provide basis for the study, selected companies were heterogeneous and characterized as operating in unhealthy environments.
The branches of industry were very diversified, including metallurgy and chemical plants, agribusiness, IT and pharmaceutical industries, civil construction, transportation and food companies, totaling 18 companies in the region of Campinas, São Paulo.
Procedure
Audiologists, reinforcing the reliability of the data, as provided by Act 6965/81 conducted all procedures, as well as the analysis of the results.
Anamnesis and Meatoscopy
We studied the questionnaire answered by the patients in order to collect data about personal identification, professional and health history, previous otological problems, main complaints, habits and auditory difficulties.
We noticed in the files that the tests were conducted in accordance with the advocated audiometric assessment - Administrative Act No. 24 - in which meatoscopy is recommended as a strategy to check the presence of foreign bodies or obstructive wax that could hinder the audiometric assessment9.
To meet the requirements defined by the legislation in place, auditory rest for at least 14 hours was respected before the tests were carried out.
Audiometric assessment
We carried out pure tone audiometry in frequencies of 0.25 kHz, 0.50 kHz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz and 8 kHz. Also bone tones, whenever necessary, of 0.50 kHz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, respecting the criteria set forth by Santos a Russo28.
The equipment used was an audiometer Madsen Midimate 602, calibrated according to ANSI S3.624. They also carried out biological calibration to detect any acoustic modifications in the device.
All audiometric studies of the present retrospective analysis were carried out in a sound booth, according to Norm ANSI S3-125.
Criteria for analysis of audiograms
So as to follow the parameters advocated by the Labor Safety and Health Agency (Administrative Act No. 19 - 1998), we decided to analyze audiometric configurations based on the criteria determined by the PCMSO, at the moment of hiring8.
Figure 1. Distribution of workers who participated in the study according to age ranges and gender.
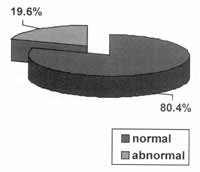
Figure 2. Distribution of workers who participated in the study according to PCMSO criteria.
Figure 3. Mean, standard error (+- 5td. Err.) and standard deviation (+- 5td. SD) of audiometric thresholds (in dBHL) of 0.25 kHz to 8 kHz, on the left ear.
Figure 4. Mean, standard error (+- 5td. Err.) and standard deviation (+- 5td. SD) of audiometric thresholds (in dBHL) of 0.25 kHz to 8 KHZ, on the right ear.
The interpretation of results respected the following the parameters:
Normal - or within normal ranges - cases whose audiograms showed hearing thresholds lower or equal to 25dBHL in all studied frequencies;
Abnormal - or suggestive or not of NIHL - cases whose audiograms showed hearing thresholds higher or equal to 25dBHL in at least one of the studied frequencies.
In order to characterize the audiometric findings as to the type of hearing loss, we followed the criteria described by Santos and Russo28, in which hearing loss is divided by conductive, sensorineural and mixed, following the criteria below:
Conductive loss: pure tone loss greater than 25dBHL, and bone thresholds within normal ranges. There is an air-bone gap greater than 15dB.
Sensorineural loss: hearing loss greater than 25dBHL, both for air and bone thresholds. There is an air/bone gap below 15dB.
Mixed loss: pure tone audiometry presents air/ bone gap in some frequencies, and similar thresholds in others.
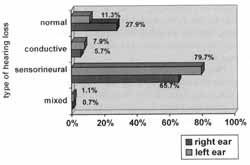
Figure 5. Percentage of workers who participated in the study according to type of hearing loss and analyzed ear.
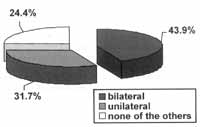
Figure 6. Percentage of workers who participated in the study according to audiometric curve suggestive of NIHL.
RESULTS
Out of 3,117 studied workers, 2,507 (80.4%) presented normal audiometry and 610 (19.6%) presented abnormal results (Figure 2).
Based on the objectives of the present study, we describe next the analysis of the 610 individuals with abnormal hearing test.
In order to learn more, we calculated the mean, median and standard deviation of workers who participated in the study, with audiometric findings according to age. We noticed that the mean and median were 36 years of age for male workers and 30 years of age for female workers.
We also calculated mean, median and standard deviation for thresholds in each audiometric frequency (0.25 kHz, 0.50 kHz, 1 kHz, 2 kHz, 3 kHz, 4 kHz, 6 kHz and 8 kHz), on both right and left ears (Figures 3 and 4).
The results of audiometry of workers who had audiometric alterations indicate in both ears audiometric profiles with the worst responses in 6 kHz, 4 kHz and 8 kHz.
Out of 610 workers with abnormal audiometry, 35 (5.7%) had conductive loss, 401(65.7%), had sensorineural loss and 4 (0.7%), had mixed loss, when we analyzed only the right ear. It means 69 (11.3%) workers with hearing abnormalities presented normal hearing in the left.
Out of 610 workers with hearing loss, 48 (7.9%) presented conductive hearing loss, 486 (79,7%), had sensorineural loss and 7 (1.1%), had mixed loss if we analyzed only the left ear (Figure 5).
The analysis revealed that 170 (27.9%) of the workers with hearing abnormalities who participated in the study had normal hearing in the right ear.
We could also notice that 440 (73.1%) workers with audiometric alterations had hearing loss in the right ear, whereas 541 (88.7%) of the workers with audiometric alterations had it in the left ear.
Based on the collected data, we noticed a high incidence of sensorineural loss and we concluded that part of the studied population had typical audiometric profile, suggestive of NIHL, without masking the existence of the other curves.
Therefore, we defined the tendency of the profile, exploring the audiometric finding suggestive of NIHL.
Data determined that 268 (43.9%) of the workers had suggestive NIHL audiometric profile bilaterally and 193 (31.7%) of the workers had suggestive NIHL audiometric profile unilaterally, whereas 149 (24.4%) did not have a typical NIHL profile (Figure 6).
Therefore, we could define that 461(75.6%) workers had a typical NIHL audiometric profile in at least one of the ears.
DISCUSSION
Audiometric findings collected from the present study are in accordance with the statement by Kitamura16, who confirmed the existence of a large group of job applicants with hearing loss that prevented them from being hired by a new company, sometimes due to minor abnormalities.
Therefore, only part of the population available for the job market (80.4%) could join a company's staff without restraints. Kwitko18 pointed out that the pre-hiring physical examination has been used to refrain people with hearing loss from being hired, which is far from what was initially intended with the test.
Results revealed that a considerable number of applicants - 610 (19.6%) would possibly have problems when joining a new company since they presented some kind of hearing loss.
Similar data were observed by Kwitko18, who confirmed that the audiometry used as a routine for hiring purposes may identify individuals who already have hearing loss, therefore, be used as an instrument to motivate the development of a hearing conversation program in the company. The definition of pure tone thresholds only shows that there has been a damage of cochlear hair cells, but it does not provide a precise indication of the level of functional compromise of hearing.
Kobata17 developed a similar study in which he studied the audiometric profile of workers submitted to tests during the pre-hiring physical examination. Out of a total, 244 (34.27%) presented some kind of abnormal configuration. Although findings resultant from the present study present fewer applicants with audiometric abnormalities, that is, 610 (19.6%) of the applicants, it also showed that a significant portion of the population would possibly start the professional activity with some sort of hearing damage.
It is worth mentioning that NIHL is not produced only by industrial noise, but also by everyday sounds, causing the so-called sociacusia.
Various authors investigated extra-occupational noise exposure in order to highlight the influence of this kind of exposure on the hearing of individuals.
Campinas is a very noisy city, similar to all large centers. Daily environmental noise made by urban and industrial sources contributes to increase the risk to auditory health, and in most situations, it provides quite a loud level of noise.
The aggravating factor is that individuals exposed to these sound levels are in general young people, who present some kind of hearing damage even before they start their professional lives.
Data reinforce such comments, showing how young people were the applicants studied here.
This issue is also supported by studies that emphasize that work is the compulsory insertion of the subject into a system of social and economic relations, and that it has been an important factor for enjoyment of citizenship5,14.
It is also important to point out that a number of diseases may generate hearing loss in the range of 4kHz, presenting an audiogram configuration with a drop in 4kHz, which is not enough evidence to diagnose a NIHL. This requires complete clinical history to exclude the likelihood of other causes29.
A valuable contribution was made by Almeida2, when she concluded that because of metabolic and circulatory peculiarities, the inner ear could be the target of various systemic diseases of common incidence in the population. Manifesting sensorineural audiometric profile similar to the one caused by noise, such as sickle cell anemia, syphilis, renal failure, epidemic parotiditis, measles, mumps, cytomegalic inclusion disease and hypothyroidism, among others.
We agree with Almeida and Resende1 that the suggestive result of NIHL in the applicant's test should not disqualify him or her from working. In most cases, NIHL does not result in disability to work and should not necessarily make the worker interrupt his or her job. In order to follow such a principle, we have to assume that all companies have an efficient hearing loss prevention program in place, coordinated by skilled professionals, who will be responsible for following up the individuals and integrating them in new positions.
According to the studied literature, a number of causes of sensorineural, conductive and mixed loss may affect the population in general without manifesting clinical symptomatology.
Quite frequently, workers who are submitted to audiometric tests are not aware of their hearing acuity and they are taken aback by the results in many situations.
The audiologist has a key role in the process, not only to perform the test, but also because it is one of the few people who have direct and prolonged contact with the worker, in a moment in which the hearing loss is a top priority. It is the right moment to refer the patients to a specialist, providing treatment and/or adequate medical intervention and follow-up. In many situations, the initial problem is solved.
The studies by Maciel et al.20 demonstrate this hypothesis. They investigated the influence of earwax on the pure tone thresholds and their modification after its removal. If excessive and impacted, earwax may cause a conductive hearing loss.
Jerger a Jerger15 studied the result of false-positive losses determined by conductive losses caused by closing of the external acoustic canal under the pressure of the earphones during the test.
Tympanic perforation, in turn, depending on size and location, may determine hearing loss of variable degrees, but they may be submitted to treatment and recovery of audiometric thresholds.
Companies that have an active program of prevention of hearing loss will not probably be subject to these kinds of events. One of the purposes of the program is to identify those who need referral to otorhinolaryngologists in order to perform differential diagnosis or treat possible external and/or middle ear.
The diagnosis of noise induced hearing loss is not always precise especially when there is some other associated disease.
To guarantee the hypothesis made, we quote the studies by Jerger and Jerger15, who described otosclerosis characterized by progressive sensorineural loss, excellent discrimination in young adults, and Lopes Filho19, who described that ototoxic drugs may result in severe sensorial hearing impairment bilaterally.
Nevertheless, we should not exclude the likelihood of these workers having a NIHL, since they are exposed to occupational noise and others.
These data are in accordance with Fiorini13, who concluded that noise is currently part of our everyday life (traffic noise and leisure, among others), and considered that NIHL may become one of the main chronic diseases of the future.
It is important to highlight that a subject with NIHL should not be considered disable to work, neither absolute or universally. Disability, if present, concerns one specific task performed under specific conditions and within the company's environment.
Companies that have an effective program of prevention of hearing loss are not subject to such events, since it is part of program to define the baseline audiogram of workers, identifying their auditory situation and providing a rigorous follow-up, in order to keep workers hearing.
Based on the data, we inferred that part of the studied population had audiometric profiles typically suggestive of NIHL, without masking the existence of the other profiles.
Therefore, we defined a tendency of profile, exploring the NIHL suggestive profile.
All in all, we found that 461 (75.6%) of the workers presented NIHL typical curve at least in one of the ears.
Based on the studied literature, we observed that most of the studies conducted with workers concluded that there is a predominance of hearing loss in the workplace in more than 50% of the studied individuals, in accordance with the findings from the present study12,21,22,24,25,30.
The fact is a number of workers have been rejected in their job applications because they have minor audiometric alterations and were considered disabled and inapt to work.
CONCLUSION
Results indicated that 80.4% of workers presented hearing levels within normal ranges and 19.6% presented audiometric abnormality.
As to prevalence of hearing loss and type of loss, results indicated that when we analyzed only the right ear, out of the 610 workers who had audiometric alterations, 5,7% presented conductive hearing loss, 65,7% had sensorineural hearing loss, and 0.7% had mixed loss. When we considered only the left ear, 7.9% had conductive loss, 79.7% had sensorineural loss, and 1.1% had mixed loss.
The present study identified a large number of workers that have some kind of hearing impairment who will not be hired for a new job. Excluded from the marketplace, and forbidden to do what they have been specialized in, applicants are faced with unemployment and might end up having a marginal life.
Operational resources should be employed to guarantee the preservation of hearing acuity, either by preserving normal hearing or residual hearing, and referring the patients. Job positions that require absolutely normal hearing acuity, such as air traffic controller, aircraft pilots and musicians, and those with progressive hearing loss, should be rigorously and carefully followed up.
Employers are always interested in having and maintaining the most skillful workers for each task, and many of them have hearing problems. Therefore, we emphasize the importance of implementing a good-quality program of hearing preservation so that qualified workers with NIHL may be kept in his/her department without having the aggravation from the disease, preserving his/ her occupational capacity.
REFERENCES
1. ALMEIDA, E.R. & REZENDE, V.A. - Implicações médico-legais da P.A.I.R., F. Med (BR), 117 (Supl 1):25-31, 1998.
2. ALMEIDA, S.I.C. - Diagnóstico diferencial da disacusia neurossensorial induzida pelo ruído. Rev. Assoc. Med. Bras., 37(3):150-2, 1991.
3. AMERICAN NATIONAL STANDARDS INSTITUTE - Maximum permissible environment noise levels for audiometric test rooms. ANSI S3.1-1991, New York, 1991.
4. AMERICAN NATIONAL STANDARDS INSTITUTE - Specification for audiometers. ANSI S3.6-1989, New York, 1989.
5. BOSI, E. - Memória a sociedade: lembranças de velhos. São Paulo, Companhia das Letras, 1994.
6. BRASIL - COMITÊ NACIONAL DE RUÍDO E CONSERVAÇÃO AUDITIVA - Boletim n ° 3 - Condutas na perda auditiva induzida pelo ruído. Belo Horizonte, 1995.
7. BRASIL - COMITÊ NACIONAL DE RUÍDO E CONSERVAÇÃO AUDITIVA - Boletim n° 1 - Perda auditiva induzida pelo ruído relacionada ao trabalho. Acústica a Vibrações, 13:123-5, 1994.
8. BRASIL - NORMA TÉCNICA PARA CONTROLE DA AUDIÇÃO PARA TRABALHADORES - (Port. n° 19 de 09.04.1998). Secretaria de segurança a saúde no trabalho. D.O.U. de 22.04.1998.
9. BRASIL - NORMA TÉCNICA PARA CONTROLE DA AUDIÇÃO PARA TRABALHADORES - (Port. N° 24 de 29.12.1994). Secretaria de segurança a saúde no trabalho. D.O.U. de 30.12.1994
10. CELANI, A.C.; COSTA FILHO, O.A.; TROISE, S.J. - Brinquedos a seus níveis de ruído. Rev. Dist. Com., 4(1):49-58, 1991.
11. FERREIRA JUNIOR, M. - Perda auditiva induzida pelo ruído - Bom senso a consenso. São Paulo: Ed. VK, 1998.
12. FIORINI, A.C. - Conservação Auditiva: Estudo sobre o monitoramento audiométrico em trabalhadores de urna ind6stria metalúrgica. São Paulo, 1994a [Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo].
13. FIORINI, A.C. - O use de registros de emissões otoacusticas como instrumento de vigilância epidemiológica de alterações auditivas em trabalhadores expostos a ruído. São Paulo, 2000 [Tese de Doutorado - Universidade de São Paulo].
14. JANUZZI, G.S.M. - Mercado de trabalho do deficiente: aspectos da legislação brasileira. Temas sobre Desenvolvimento. 4(21): 14-9.1994.
15. JERGER, S. & JERGER, J. - Alterações auditivas. Ed. Atheneu, São Paulo, 1989.
16. KITAMURA, S. - Contribuição ao estudo da audiometria normal: os exames audiométricos pró-admissionais. Rev. Bras. Saúde Ocup., 71:46-9, 1990.
17. KOBATA, D.Y. - Perfil audiométrico de trabalhadores submetidos a exame admissional. São Paulo, 1997 [Monografia apresentada no curso de Especialização em Audiologia - CEFAC - CEDIAU].
18. KWITKO, A. - Audiometria ocupacional no programa de conservação auditiva: relevância a confiabilidade. Rev. Brasil. ORL., 5:66-72, 1998.
19. LOPES FILHO, O.C. - Deficiência auditiva. - In: LOPES FILHO, O.C. - Tratado de Fonoaudiologia - São Paulo, Ed. Roca, 3-24, 1997.
20. MACIEL, J.P.; CAVADAS M.; FROTA S.; KOS M.I. - A influencia da rolha de cera nos limiares tonais por via aérea. Anais do XIV Encontro Internacional de Audiologia, Rio de Janeiro, 1999.
21. MARQUES, S.R. - Os efeitos do ruído em motoristas de ônibus urbanos do município de São Paulo. São Paulo, 1998 [Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo].
22. MORATA, T.C. - Saúde do trabalhador: estudo sobre a exposição simultanea a ruído a dissulfeto de carbono. São Paulo, 1986. [Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo].
23. NOGUEIRA, K. - Durma com todo esse barulho. Rev. Veja, 28(21):12 18 1445
24. PEREIRA, C.A. - Surdez profissional em trabalhadores metalúrgicos: estudo epidemiológico em uma indústria da Grande São Paulo. São Paulo, 1978 [Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo].
25. PR6SPERO, A.C. - Estudo dos efeitos do ruído em servidores do centro técnico aeroespacial. São Paulo, 1999 [Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo].
26. ROLLA, S. - Avaliação da poluição sonora na cidade de Campinas S.P. Anais do Congresso Brasil/ Argentina a Encontro da Sociedade Brasileira de Acústica (SOBRAC), Florianópolis, 1994.
27. RUSSO, I.C.P.; SANTOS, T.M.M.; OSTERNE, F.J.S.; BUSGAIB, B.B. Um estudo comparativo sobre os efeitos da exposição a musica em músicos de trio elétricos. Rev. Brasil. ORL., 61(6):477-84, 1995.
28. SANTOS, T.M.M. & RUSSO, I.C.P. - A pratica da audiologia clinica. 4ª ed. São Paulo, Cortez Editora, 1993.
29. SATALOFF, R.T. - The 4.000 Hz audiometric dip. Ear Nose & Throat J, 59:24-32, 1980.
30. SOUZA, M.T. - Efeitos auditivos provocados pela interação entre ruído a solvente, uma alternative em audiologia voltada a saúde do trabalhador. São Paulo, 1994. [Dissertação de Mestrado - Pontifícia Universidade Católica de São Paulo].
1 Audiologist, Master in Speech and Hearing Disorders, PUGSP, São Paulo/Brazil; Professor of the Speech and Hearing Disorders School, UNIMEP, Piracicaba, São Paulo/ Brazil.
2 Audiologist, Faculty Professor, Post-Graduate Studies Program in Speech and Hearing Disorders, PUC- SP, Brazil.
3 Part of the Master Degree dissertation, Post-Graduate Studies Program in Speech and Hearing Disorders, PUC- SP,- Brazil.
Address correspondence to: R. Maria Monteiro, 1297 apto. 72 - Cambuí - CEP; 13025-152 Campinas/SP - Brazil. Tel: (55 19) 3252-3032.
Study presented at XVI Encontro Internacional de Audiologia - Rio de Janeiro - April 5 - 8, 2001.
Article submitted on March 20, 2001. Article accepted on June 18, 2001.
Print: ![]()