

Year: 2014 Vol. 80 Ed. 2 - (19º)
Relato de Caso
Pages: 184 to 185
 PDF PT
PDF PT  PDF EN
PDF ENSolitary neurofibroma of the palate*
Author(s): Fábio Wildson Gurgel Costa1; Francisco Samuel Rodrigues Carvalho1; Cássia Farias de Sousa2; Roberta Barroso Cavalcante3,4; Karuza Maria Alves Pereira3,5
DOI: 10.5935/1808-8694.20140038
![]()
INTRODUCTION
Neurofibromas are benign tumors arising from peripheral nerve sheaths that affect the head and neck region only rarely,1 and consist of Schwann cells, perineural cells, and a variable amount of mature collagen.2 They are classified as solitary when not associated with any syndrome or multiple when associated with autosomal dominant neurofibromatosis syndrome or type III multiple neoplastic syndrome;3 they can also be classified as myxomatous (solid, central, diffuse) or plexiform (peripheral).4 When not associated with syndromes, they rarely occur in the oral cavity, and then most commonly in the tongue.
CASE REPORT
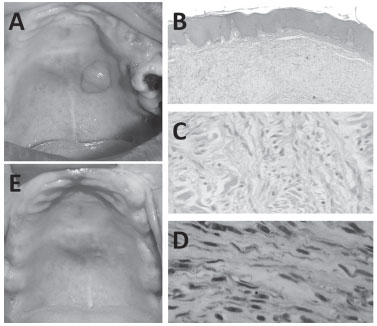
A 54-year-old female patient with melanoderma without systemic involvement, was referred for evaluation of an asymptomatic intraoral pedunculated nodular lesion located on the palate, similar in color to the adjacent mucosa, that measured approximately 8 mm (Fig. 1A), exhibited an uneven surface, had a fibrous consistency, and had been present for three months. Extraoral physical examination revealed characteristic stigmata of neurofibromatosis, involving the chest. An excisional biopsy and histopathological examination were performed, and revealed mucosal fragments covered with stratified squamous epithelium (ortho or parakeratinized), with acanthosis.
Figure 1 Solitary neurofibroma of the palate. A, Initial clinical aspect of the lesion. B, Photomicrograph showing the presence of a nonencapsulated benign tumor, consisting of fusiform cells with undulated nucleus. C, Photomicrograph showing spindle cell proliferation amid a myxomatous stroma, at times microvacuolated (HE, 100×). D, Strong immunohistochemical staining of spindle cells for S-100 protein (200×). E, Extra-oral examination after six months, showing complete healing.
The lamina propria showed spindle cell proliferation, sometimes with undulated nuclei amid marked collagen fiber deposition, arranged in variable-sized bundles in addition to mast cells (Fig. 1B-C). The report suggested a diagnosis of neurofibroma, with the analysis revealing strong immunohistochemical staining for S-100 protein (Fig. 1D). The patient is undergoing clinical follow-up and has shown no signs of recurrence (Fig. 1E).
DISCUSSION
It is believed that the frequency of oral solitary neurofibromas not associated with neurofibromatosis-1 is low,4 with only a few cases located on the palate,2,3 despite a more common occurrence in the tongue.1-4 They are slow-growing, nodular, sessile, and mobile tumors,3 usually painless, although pain or numbness may occur due to nerve compression. Cherrick and Eversole2 observed a higher incidence in females. Chen and Miller5 reported that oral neurofibromas affect individuals between 9 and 72 years of age. Although some lesions require imaging tests to determine possible extension, conventional histological analysis is conclusive when proliferation of Schwann cells, perineural cells, and fibroblasts are observed amid a stroma, sometimes myxomatous and microvacuolated.4
The distinction between solitary neurofibromas and those associated with neurofibromatosis is that the latter, although unencapsulated, show clear distinction between the lesion margin and adjacent tissue.1 The treatment is surgical removal, because of an uncertain risk of recurrence or malignant transformation; the prognosis is excellent.4
FINAL CONSIDERATIONS
Considering that isolated neurofibromas in the oral cavity are rare, the importance of a thorough clinical examination by professionals familiar with examining and treating patients with oral cavity lesions, such as dentists, maxillofacial surgeons, head and neck surgeons, otolaryngologists, as well as dermatologists, is reinforced. Neurofibroma not associated with neurofibromatosis-1 should be included in the differential diagnosis of hyperplastic lesions of the oral cavity, although they are rarely described in such location.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Wright BA, Jackson D. Neural tumors of the oral cavity. A review of the spectrum of benign and malignant oral tumors of the oral cavity and jaws. Oral Surg Oral Med Oral Pathol. 1980;49:509-22.
2. Cherrick HM, Eversole LR. Benign neural sheath neoplasm of the oral cavity. Report of thirty-seven cases. Oral Surg Oral Med Oral Pathol. 1971;32:900-9.
3. Alatli C, Oner B, Unur M, Erseven G. Solitary plexiform neurofibroma of the oral cavity A case report. Int J Oral Maxillofac Surg. 1996;25:379-80.
4. Marocchio LS, Oliveira DT, Pereira MC, Soares CT, Fleury RN. Sporadic and multiple neurofibromas in the head and neck region: a retrospective study of 33 years. Clin Oral Investig. 2007;11:165-9.
5. Chen SY, Miller AS. Neurofibroma and schwannoma of the oral cavity. A clinical and ultrastructural study. Oral Surg Oral Med Oral Pathol. 1979;47:522-8.
1. Department of Oral Surgery, Universidade Federal do Ceará (UFC), Fortaleza, CE, Brazil
2. Universidade Federal do Ceará (UFC), Fortaleza, CE, Brazil
3. Universidade Federal do Rio Grande do Norte (UFRN), Natal, RN, Brazil
4. Department of Oral Pathology, Universidade de Fortaleza (UNIFOR), Fortaleza, CE, Brazil
5. Department of General Pathology, Universidade Federal do Ceará (UFC), Fortaleza, CE, Brazil
Corresponding author.
F.W.G. Costa
E-mail: fwildson@yahoo.com.br
Received 25 August 2012.
Accepted 13 January 2013.
* Study conducted at Universidade Federal do Ceará , Fortaleza, CE, Brazil.
Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial