

Year: 2014 Vol. 80 Ed. 1 - (15º)
Artigo de Revisão
Pages: 78 to 85
 PDF PT
PDF PT  PDF EN
PDF ENOral manifestations resulting from chemotherapy in children with acute lymphoblastic leukemia
Author(s): Everton Freitas de Morais1; Jadson Alexandre da Silva Lira1; Rômulo Augusto de Paiva Macedo1; Klaus Steyllon dos Santos1; Cassandra Teixeira Valle Elias2; Maria de Lourdes Silva de Arruda Morais1,3
DOI: 10.5935/1808-8694.20140015
Keywords: Child; Drug therapy; Leukemia; Oral manifestations
Abstract:
INTRODUCTION: Acute lymphocytic leukemia is a type of cancer most common in children and it is characterized by excessive and disordered immature leukocytes in the bone marrow.
AIM: Identify most frequent oral manifestations in children with acute lymphocytic leukemia under chemotherapy treatment.
METHODOLOGY: The research was conducted on the eletronic database PubMed/Medline, Science Direct, Scielo and Scopus. It has been sought papers with full presentation, wrote in Portuguese, English and Spanish, published between January 1992 and April 2013.
RESULTS: From studies primarily selected, only eight met the criteria of inclusion. All studies performed intraoral examinations to diagnose oral lesions. According to results, the most frequent lesions were mucositis, candidiasis, periodontitis and gingivitis. The oral health condition from acute lymphocytic leukemia carriers varied according oral hygiene of the patient.
CONCLUSION: The results of studies identified such a great part of patients with ALL presented some lesion in oral cavity during or after chemotherapy treatment. The dentist surgeon needs to recognize oral manifestations and intervene in the oral health of patients with ALL, contributing and helping with treatment.
![]()
INTRODUCTION
Leukemia is a disease characterized by progressive and excessive production of leukocytes in the bone marrow, whose immature forms start circulating in blood.1,2 The disseminated proliferation of blasts leads to a substitution of normal bone marrow elements, resulting in the accumulation of immature cells in the blood. The etiology of leukemia is still uncertain, but many studies point to causal factors such as viral infection and radiation and chemical exposure. There are three different subtypes of lymphocytes, and thus there are different types of leukemia, which are classified according to the cell involved, as well as the duration and characteristics of the disease.1-4
Acute lymphoblastic leukemia (ALL) represents approximately 80% of leukemias, and occurs mostly in children.1 ALL results in uncontrolled and excessive production of lymphoid blasts, hindering the normal production of red and white cells, as well as platelets. The chances of survival have increased with advances in anticancer treatment modalities.2,3
The first signs of leukemia can regularly occur in the oral cavity, especially in the acute phase of cancer, as common lesions at this stage of the disease that can be observed and recognized primarily by the dentist.4,5 The most common manifestations of leukemia in the oral cavity are gingival bleeding, hyperplasia, opportunistic infections, and bone alterations.
During the antineoplastic treatment, the lesions become even more severe, since chemotherapy acts on poorly differentiated or high-metabolism cells, affecting not only blast cells, but also normal body cells.3,4
The dentist needs to be aware of lesions caused by leukemia and the anticancer treatment in order to improve the patient's oral health. Thus, this study aimed to perform a systematic review of the literature on oral complications secondary to chemotherapy performed in children with ALL.
METHODS
A systematic search of articles in English, Portuguese, and Spanish published between January of 1992 and April of 2013 was performed in the PubMed/MEDLINE, Science Direct, Scopus, and SciELO databases. Studies whose the target population was children aged 2 to 18 years with ALL and that evaluated the complications of anticancer treatment in the oral cavity were selected.
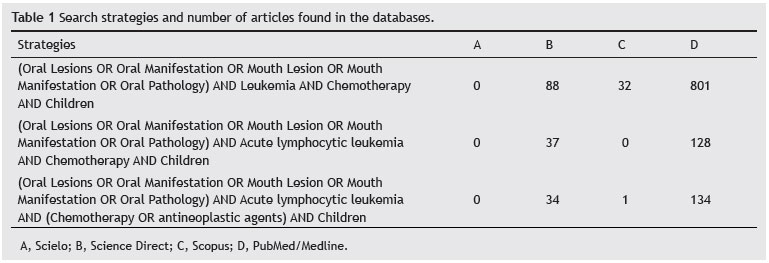
The search used the following terms: oral manifestations, Leukemia, Acute Lymphoblastic Leukemia, ALL, chemotherapy, and children, as well as the corresponding words in Portuguese and Spanish. The Boolean operators AND, OR, NOT were used in the databases, when possible. The search strategies are shown in Table 1.
After the initial search and retrieval of abstracts, four independent evaluators selected the relevant studies according to the inclusion and exclusion criteria. Longitudinal or cross-sectional controlled clinical trials that assessed oral manifestations in children with ALL were included in the systematic review. Studies in languages other than those primarily chosen, in vitro studies, animal studies, literature reviews, case reports, and studies not associated with the target population or the oral manifestations of the disease were excluded.
The first step in study selection was performed by analyzing the titles and abstracts. Subsequently, all studies whose titles or abstracts were considered relevant were obtained in full and thoroughly analyzed. Finally, the articles reviewed and selected through consensus of the five evaluators were included in the data systematization.
RESULTS
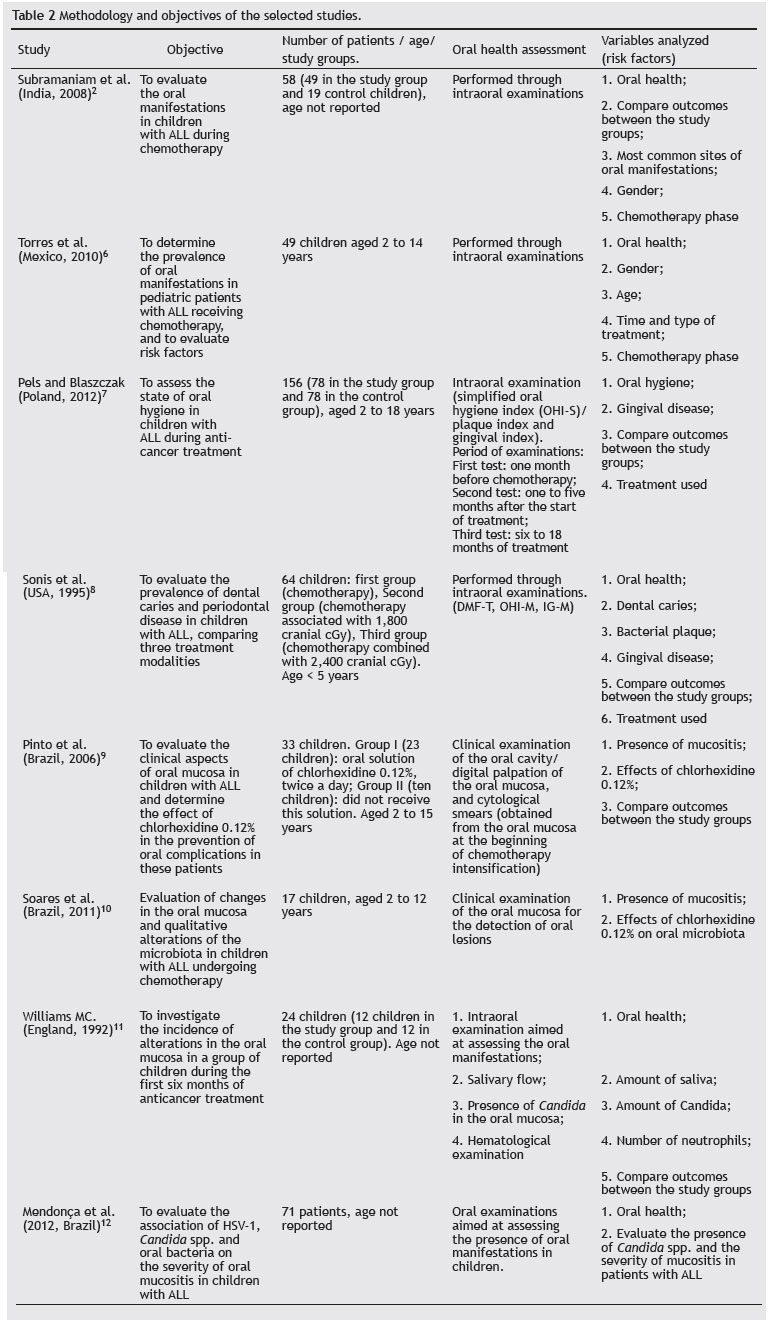
Among the initially selected studies, 18 showed potential to be included in the systematic review; however, after thorough analysis of the studies, only eight met all the inclusion criteria. Among the selected studies, five had been performed in developing countries and three in developed countries; the methods and results of the studies are summarized in Tables 2 and 3.
Regarding the profile of the studies, the sample size ranged between 17 and 156 children, with a total sample size of 472 children aged 2 to 18 years. The selected studies were published between the years 1992 and 2012. Of the selected studies, seven were cross-sectional; only the study by Williams et al.11 was longitudinal. The main objective of all selected studies was the evaluation of oral complications due to chemotherapy in patients with ALL.
The studies by Torres et al.6 and Subramaniam et al.2 evaluated the incidence of oral manifestations between genders. In the study by Torres et al.,6 of the 49 children studied, 26 (53%) were males and 23 (47%) females. In the study by Subramaniam et al.,2 of the 58 children, 37 (63.8%) were males and 21 (36.2%) females. The authors did not establish an association between gender and the frequency of oral manifestations. The remaining studies included in this systematic review did not assess their patients according to gender. In all selected studies, the intraoral examination was used to establish the diagnosis of oral lesions during chemotherapy.
Of all evaluated studies, only Pels et al.7 reported the performance of intraoral clinical examination before the start of chemotherapy. Among the variables analyzed by the authors were chemotherapy, type of drugs used by the children with ALL, use of chlorhexidine gluconate, oral hygiene, and place of residence.
Although six2,6-9,12 of the eight articles mentioned the drugs used for chemotherapy, no clear correlation was established between oral complications and type of drug used. Pels et al.7 established an association between the phase of chemotherapy and oral complications; oral manifestations were more common in the induction phase.
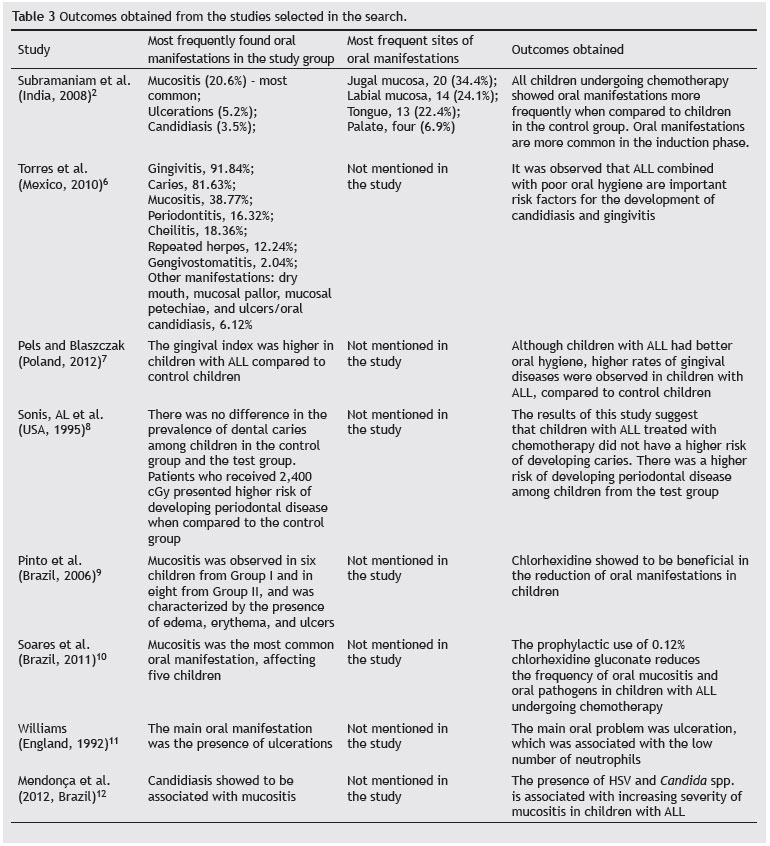
The most frequent oral lesions were mucositis,2,6,9-12 candidiasis,2,6,12 periodontitis,6-8 and gingivitis.6 The most common sites of oral manifestation involvement were the oral mucosa and labial mucosa, according to the study by Subramaniam et al.2 The oral manifestations and most common sites of the selected studies are presented in Table 3.
The prevalence of oral manifestations was related to patients' poor oral hygiene6 and antineoplastic treatment;2,8 in the selected studies, no specific drug was related to the presence of oral manifestations. Another important factor related to oral manifestations was the quality of life and social class of the patients with ALL,6 as the presence of HVS and Candida spp. was associated with increasing severity of mucositis in children with ALL.12
DISCUSSION
The selected studies in this systematic review evaluated the oral manifestations in patients with ALL. The studies by Torres et al.6 and by Subramaniam et al.2 estimated the incidence between genders, but did not establish an association between gender and frequency of oral manifestations; no other study showed such association.
In the study by Subramaniam et al.,2 oral manifestations were observed in 77.8%, 36.4%, 70%, and 66.7% of children, divided according to the groups in the study. In the study by Torres et al.,6 approximately 95% of patients had some type of oral manifestation. These results corroborate the findings from other studies.13,14
Chemotherapy can be directly toxic and affect the oral mucosa through the systemic circulation. Moreover, the drugs used are often secreted through the saliva, which results in drug exposure in the oral cavity.15 However, among the studies selected, only six2,6-9,12 mentioned the drug combinations used in chemotherapy, and none directly correlated the oral manifestations to a specific type of drug.
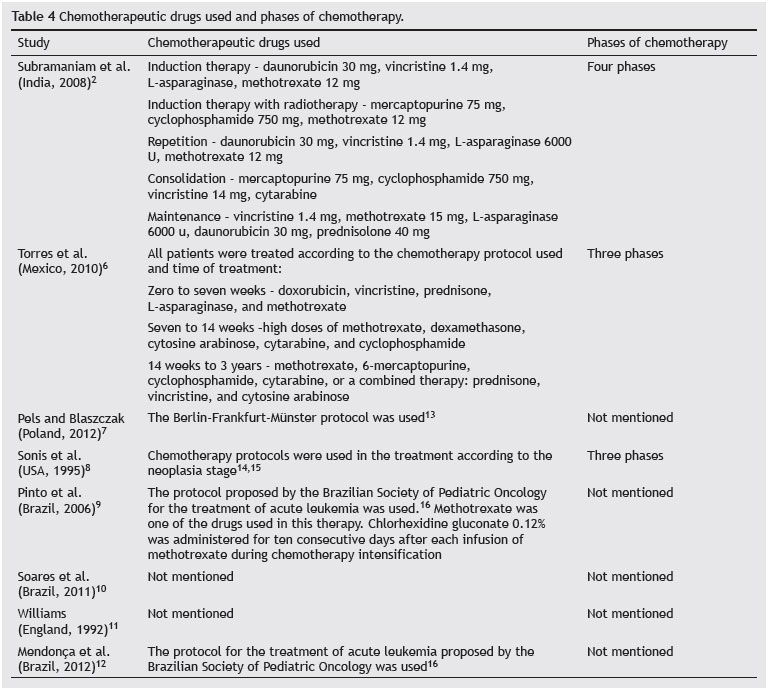
Among the drugs most often associated with oral manifestations, teniposide, paclitaxel, methotrexate, idarubicin, epirubicin, doxorubicin, cisplatin, and cytarabine are associated with mucositis, xerostomia, gingival bleeding, and other diseases of the oral cavity.16,17 Methotrexate, bleomycin, doxorubicin, cisplatin, vinblastine and vincristine are drugs that produce direct toxicity of some of their antimetabolites and other synthetic agents, such as hydroxyurea and procarbazine hydrochloride, which lead to glandular degeneration, changes in collagen, and epithelial dysplasia.15,18 Drug combinations used during chemotherapy in the studies are shown in Table 4.
Mucositis was the most common oral manifestation in the study by Subramaniam et al.,2 affecting 20.6% of patients with leukemia, whereas among children who were not undergoing treatment, only 3.4% had mucositis. For most researchers, mucositis is caused by chemotherapy and occurs due to a dynamic process, resulting in the destruction of the basal cells; the same is stated by Sonis,19 in a study published in 1998, who also mentioned that tissue damage was caused by direct contact with the antineoplastic agents. In the study by Torres et al.,6 mucositis was not the most frequent disease; nevertheless, it affected approximately 38.7% of children.
In the study by Pels et al.,7 although children with ALL had better oral hygiene, they had more oral manifestations than children from the comparison group; oral mucositis was the most common lesion among patients undergoing chemotherapy. Pinto et al.9 concluded that good oral hygiene associated with the use of 0.12% chlorhexidine gluconate prevented oral manifestations in children with ALL, especially mucositis, due to its capacity to interfere with microorganism adhesion, when used as an antiseptic in the oral cavity.
The study by Soares et al.10 showed similar results to the study of Pinto et al.9 children who used chlorhexidine gluconate had fewer oral manifestations when compared to the control group. A microbiological analysis showed a reduction in pathogenic microorganisms in the oral cavity, and mucositis, the most frequent oral manifestation, was observed in five children (29.4% of the sample). Other studies also evaluated the use of chlorhexidine in patients with ALL, with positive results in reducing oral manifestations caused by chemotherapy.20,21
In the study by Torres et al.,6 the most common oral manifestation was gingivitis, affecting 91.84% of the sample; the high rate of gingivitis in this study was associated to poor oral hygiene, in addition to chemotherapy. The chemotherapy phase also showed an association with the onset of gingivitis. In the study by Subramaniam et al.,2 the rate of gingivitis was lower: less than 2% among patients. This difference may be due to the better oral hygiene of the children participating in that study,2 corroborating the findings of Trindade et al.,14 who demonstrated that oral hygiene should be encouraged at any stage of treatment, since it can prevent oral and systemic manifestations.
The study by Sonis et al.8 concluded that patients with ALL treated with chemotherapy had the same probability of dental caries as children from the control group. For the authors, the presence of caries was associated with poor oral hygiene of the participants. These results corroborate the findings of Sepet et al.,22 who assessed the presence of caries among children in the maintenance phase of chemotherapy and in a group of healthy children, observing no correlation between the presence of caries and the use of chemotherapeutic drugs.
Primary herpetic gingivostomatitis was observed in 2.04% of the patients in the study by Torres et al.,6 and recurrent herpes in 12.24% . The presence of herpes in that study could have been caused by the participants' low immunity, associated with exposure to the virus; this result corroborates other studies that also reported the presence of herpetic stomatitis in children with ALL.23,24
In the longitudinal study by Williams et al.,11 all patients had ulcerations in the oral mucosa, whereas oral candidiasis was observed in 10% of tests performed during the study period. The presence of the disease was associated with the low number of neutrophils of leukemia patients in combination with low salivary flow caused by chemotherapy. In the study by Mendonça et al.,12 oral candidiasis was also associated with the presence and severity of mucositis; antifungal prophylaxis was suggested in patients with ALL with mucositis. This same suggestion was made in the study by Pine et al., published in 2010.25 Other oral manifestations observed in these studies were dry mouth, gingival bleeding, oral erythema, toothache, and primary herpetic stomatitis.
CONCLUSION
The oral health status of patients with ALL varies according to a number of factors. The results of the studies demonstrated that most patients with ALL had some lesion in the oral cavity during or after the start of chemotherapy. The dentist is responsible for recognizing these lesions and intervening in the oral health of these patients, thereby contributing to their treatment and quality of life improvement. New studies are required to better elucidate the subject, especially regarding the prevention and control of these oral manifestations.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Costa SS, Silva AM, Macedo IAB. Conhecimento de manifestações orais da Leucemia e protocolo de atendimento odontológico. Rev Odontol Univ São Paulo. 2011;23:70-8.
2. Subramaniam P, Babu KL, Nagarathna J. Oral manifestations in acute lymphoblastic leukemic children under chemotherapy. J Clin Pediatr Dent. 2008;32:319-24.
3. Hamerschlak N. Leukemia: genetics and prognostic factors. J Pediatr. 2008;84:52-7.
4. Maeda YC. Manifestações bucais da leucemia e do tratamento antineoplásico [Monograph]. Piracicaba: Faculdade de Odontologia de Piracicaba; 2008.
5. Silva LCP, Carneiro FM, Cruz RA. Manifestações bucais das leucemias agudas na infância. Arq Bras Odontol. 2008;4:40-54.
6. Torres EP, Ruíz MSR, Alejo GF, Hernández SJF, Pozos GAJ. Oral manifestations in pediatric patients receiving chemotherapy for acute lymphoblastic leukemia. J Clin Pediatr Dent. 2010;34:275-80.
7. Pels E, Mielnik BM. Oral hygiene in children suffering from acute lymphoblastic leukemia living in rural and urban regions. Ann Agric Environ Med. 2012;19:529-33.
8. Sonis AL, Waber DP, Sallan S, Tarbell NJ. The oral health of long-term survivors of acute lymphoblastic leukaemia: a comparison of three treatment modalities. Eur J Cancer B Oral Oncol. 2012;31:250-2.
9. Pinto LP, Souza LB, Gordón-Núñez MA, Soares RC, Costa EMMB, Aquino ARL, et al. Prevention of oral lesions in children with acute lymphoblastic leukemia. Int J Pediatr Otorhinolaryngol. 2006;70:1847-51.
10. Soares AF, Aquino ARL, Carvalho CHP, Nonaka CFW, Almeida D, Pinto LP. Frequency of oral mucositis and microbiological analysis in children with acute lymphoblastic leukemia treated with 0.12% chlorhexidine gluconate. Braz Dent J. 2011;22:312-6.
11. Williams MC, Martin MV. A longitudinal study of the effects on the oral mucosa of treatment for acute childhood leukaemia. Int J Paediatr Dent. 1992;2:73-9.
12. Mendonça RM, Araújo M, Levy CE, Morari J, Silva RA, Yunes JA, et al. Prospective evaluation of HSV, Candida spp., and oral bacteria on the severity of oral mucositis in pediatric acute lymphoblastic leukemia. Support Care Cancer. 2012;20:1101-7.
13. Ribas MO, Costa NP. Estudo das observações clínicas, estomatológicas e radiográficas das alterações dentárias e ósseas nos pacientes com leucemia na infância. Rev Odonto Ciênc. 1995;2:151-84.
14. Trindade AKF, Biases RCCG, Guedes FG, Pereira BC, Sousa ED, Queiroga AS. Manifestações orais em pacientes pediátricos leucêmicos. Arq Odontol. 2009;45:22-9.
15. Epstein JB, Tsang AH, Warkentin D, Ship JA. The role of salivary function in modulating chemotherapy-induced oropharyngeal mucositis: a review of the literature. Oral Surg Oral Med Oral Pathol. 2002;94:39-44.
16. Fonseca SM, Almeida EPM, Massunaga VM. Administração dos quimioterápicos. In: Fonseca SM, Machado RCL, Paiva DRS, Almeida EPM, Massunaga VM, Junior WR, et al. Manual de quimioterapia antineoplásica. Rio de Janeiro: Reichmann e Affonso; 2000. p. 16-9.
17. Miller D. Quimioterapia. In: Administração de medicamentos. Rio de Janeiro: Reichmann e Affonso; 2002. p. 369-82.
18. Bensaudoun RJ, Magné N, Marcy PY, Dermard F. Chemotherapy- and radiotherapy-induced mucositis in head and neck cancer patients; new trends in pathophysiology, prevention and treatment. Eur Arch Otorhinolaryngol. 2007;258:481-7.
19. Sonis ST. Mucositis as a biologic process: a new hypothesis for the development of chemotherapy-induced mucositis. Oral Oncol. 1998;34:39-43.
20. Brito CA, Araújo DS, Granja JG, Souza SM, Lima MAG, Oliveira MC. Efeito da clorexidina e do laser de baixa potência na prevenção e no tratamento da mucosite oral. Rev Odontol UNESP. 2012;41:236-41.
21. Ferretti GA, Raybould TP, Brown AT, McDonald JS, Greenwood M, Maruyama Y, et al. Chlorhexidine prophylaxis for chemotherapy- and radiotherapy-induced stomatitis: a randomized double- blind trial. Oral Surg Oral Med Oral Pathol. 1990;69:331-8.
22. Sepet E, Aytepe Z, Ozerkan AG, Yalman N, Guven Y, Anak S, et al. Acute lymphoblastic dental health na children in maintenance therapy. J Clin Pediatr Dent. 1998;22:257-60.
23. Marques HH, Yamamoto M, Odone FV. Varicela-zoster em imunodeprimidos: Estudo de 12 casos. Rev Pediat. 1981;3:335-7.
24. Childers NK, Stinnett EA, Wheeler P, Wright JT, Castleberry RP, Dasanayake AP. Oral complications in children with cancer. Oral Surg Oral Med Oral Path. 1993;75:41-7.
25. Pinho AP, Misorelli JC, Montelli R, Longato SE. Mucosite no paciente em tratamento de câncer. Science in Health. 2010;1:145-60.
1. Universidade Potiguar, Natal, RN, Brazil
2. Liga Norte-Riograndense Contra o Câncer, Natal, RN, Brazil
3. Universidade Estadual do Rio Grande do Norte (UERN), Natal, RN, Brazil
Corresponding author.
E.F. Morais
E-mail: evertonfreitas2@hotmail.com
Received 30 July 2013.
Accepted 22 September 2013.
Print: ![]()