

Year: 2014 Vol. 80 Ed. 1 - (12º)
Artigo Original
Pages: 54 to 59
 PDF PT
PDF PT  PDF EN
PDF ENCould the type of treatment for chronic kidney disease affect the auditory system?
Author(s): Priscila Suman Lopez1; Daniela Polo Camargo da Silva1; Luis Cuadrado Martin2; Jair Cortez Montovani1
DOI: 10.5935/1808-8694.20140012
Keywords: Hypertension; Diabetes mellitus; Hearing loss; Renal insufficiency chronic; Electrophysiology
Abstract:
INTRODUCTION: Chronic kidney disease (CKD) is defined as the presence of renal injury that leads to the slow and progressive loss of kidney function.
AIM: To compare audiological tests between patients with CKD receiving different types of treatment.
MATERIAL AND METHOD: This was a clinical and transversal study. Groups were divided according to treatment: hemodialysis (n = 35), peritoneal dialysis (n = 15), and conservative (n = 51), and were compared to 27 healthy controls. Patients older than 60 years; those with congenital hearing loss, genetic syndromes, and middle-ear infections; and those who had been submitted to a kidney transplant were excluded. Audiologic evaluation included puretone audiometry, transient evoked otoacoustic emissions, and auditory brainstem response (ABR). The variables considered were gender, age, diagnosis of arterial hypertension, time since the diagnosis of diabetes and hypertension, CKD stage, duration of CKD, and duration of treatment.
RESULTS: The variables age, presence of arterial hypertension, and time of CKD were statistically significant and controlled. The auditory thresholds measured by pure-tone threshold audiometry were worse for the conservative treatment group, and the III-V interval of the ABR of the conservative treatment group was significantly greater than that of the hemodialysis groups.
CONCLUSION: The conservative treatment group presented worse audiological tests, regardless of hypertension and diabetes, reinforcing that patients need to undergo a complete hearing assessment for better understanding of the disease and its effects on the auditory system.
![]()
INTRODUCTION
Chronic kidney disease (CKD) is defined as the presence of renal injury that leads to the slow and progressive loss of kidney function.1
An association between CKD and hearing loss was first described in patients with Alport syndrome.2 However, anatomical, physiological, pathological, and pharmacological similarities between the nephron and stria vascularis of the cochlea may explain this association in cases that are not related to syndromes or genetic diseases.3,4 Sensorineural hearing loss at high frequencies is the most common type in patients with CKD, and includes both cochlear impairment and lesions to particular portions of the auditory pathway.5-8
However, the influence of CKD treatment on auditory function is inconclusive,8 and hypertension and diabetes mellitus are frequently associated with CKD and hearing loss; these variables were not considered when analyzing these findings.
In the present study, the audiological tests between patients with CKD receiving different types of treatment were compared and associated with hypertension and diabetes mellitus.
METHODS
Study population
This was a cross-sectional study conducted in a tertiary referral center. The target population consisted of patients with CKD from the region around the hospital with a non-probabilistic intentional sample.
The exclusion criteria were: previous kidney transplant, congenital hearing loss or middle ear alterations, genetic syndromes, history of excessive exposure to noise, history of use of ototoxic medications, and age greater than 60 years. These data were confirmed by the patient's clinical history or medical information.
Patients were divided into groups according to treatment: hemodialysis (n = 35), peritoneal dialysis (n = 15), and conservative (n = 51), as well as 27 healthy subjects.
Audiological assessment
This audiologic evaluation consists of pure-tone audiometry (PTA), transient evoked otoacoustic emissions (TEOAEs) and auditory brainstem response (ABR).
The PTA was performed by an audiologist in a sound-treated room using standard TDH-39 earphones and an InteracousticsAD229b audiometer. Audiometric thresholds for air-conduction stimuli in both ears were established for frequencies at 250, 500, 1,000, 2,000, 3,000, 4,000, 6,000, and 8,000 Hz.
TEOAEs measurements were performed using Otodynamics ILO 288, USB II system with standard settings. The stimulus level was set to 84 dB SPL a number of 260 averages was used. Values < 3 dB amplitude were considered as negative.9
For the ABR analysis, the rarefaction click stimulus was presented by the 3 Ω insertion phone, with 90 dBnHL intensity and a presentation rate of 20.1 c/s with a band-pass filter of 100 and 3,000 Hz and average of 2,000 stimuli, using Interacoustics EP15 Eclipse. The ABR were captured through ECG disposable electrodes (MEDITRACETM 200), with EEG conductive paste (Tem 20TM) placed after cleaning the skin with ECG/EEG abrasive gel (NUPREP). The impedance level was kept between 1 and 3 kΩ for the electrodes; the active electrode was positioned in Fz, the reference electrode in M1 and M2, and the ground electrode in Fpz.10,11
Variables
Potential confounders were considered: gender, age, race, diagnosis of arterial hypertension (yes/no), time since the diagnosis of hypertension, diagnosis of diabetes (yes/no), time since the diagnosis of diabetes, CKD stage (1/2/3/4), duration of CKD, and duration of treatment.
The outcome hearing impairment was determined as as the pure-tone average of audiometric hearing thresholds at 500, 1,000, 2,000 and 4,000 Hz > 25 dB; all audiometric hearing thresholds, classification of negative TEOAEs, and parameters of ABR were analyzed.
Statistical analyses
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS), release 19.0. Nonparametric variables are expressed as the median (minimum-maximum). The chi-squared test was used to examine categorical variables. Comparisons between groups were performed with Dunn's test.
The categorical outcomes (hearing loss and negative TEOAEs) were compared by multivariable logistic regression analysis, which was used to calculate adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for associations with CKD treatment. The numerical outcomes (audiometric hearing thresholds and ABR parameters) were compared by linear regression with a gamma response, corrected by the effect of age and the presence of hypertension. p-values < 0.05 were considered to be statistically significant.
Ethics
This study was approved by the Ethics Committee of the Faculdade de Medicina de Botucatu, under Protocol No. 157/2007.
RESULTS
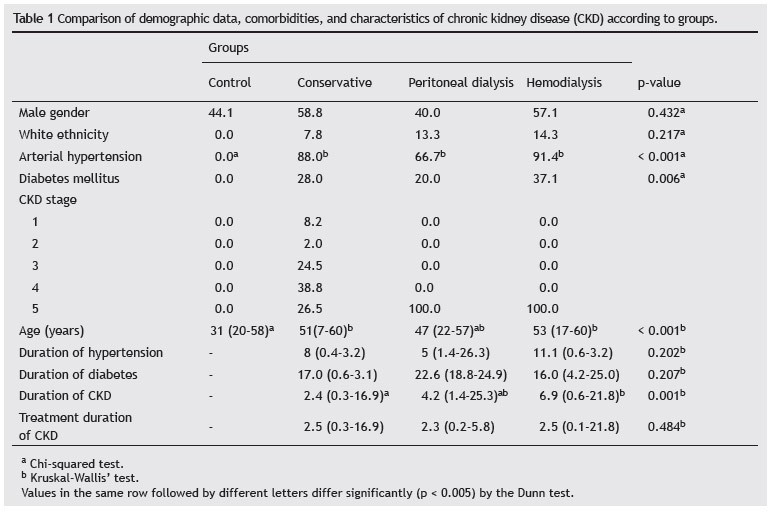
The characteristics of patients, comorbidities, CKD stage, and other data of the disease, stratified by treatment, were listed in Table 1. A statistical difference was observed in arterial hypertension, older patients, and duration of CKD.
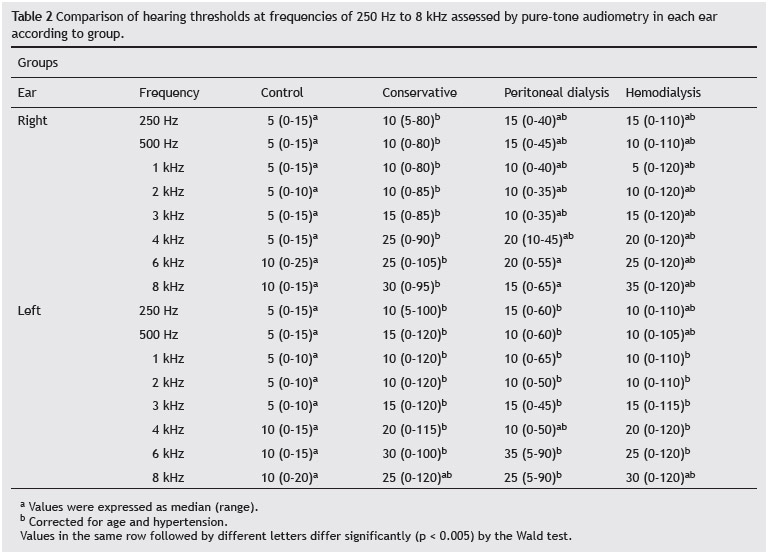
No differences were observed in the percentage of hearing loss between the various types of treatment (p > 0.05). Corrections for hypertension and age were not necessary in this case, since the types of treatment were homogeneous. However, in other comparisons, this correction was necessary (Tables 2 and 3).
The conservative group had worse hearing thresholds when compared to the control group in all frequencies tested. In contrast, no significant difference was observed between the other treatments (Table 2).The percentage of negative TEOAEs did not differ significantly among the groups (p > 0.05).
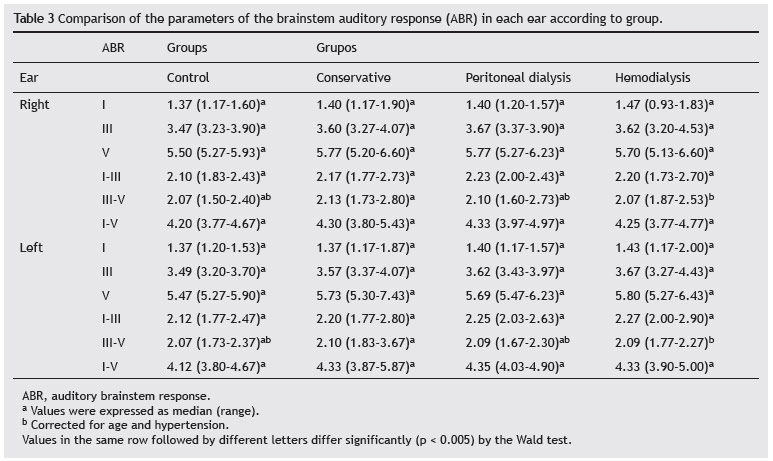
In the ABR, the conservative group had bilateral symmetric increased III-V interval compared to the hemodialysis group, with a statistically significant difference (Table 3).
DISCUSSION
The present study was motivated by the inconclusive literature findings regarding the effect of the type of CKD treatment - conservative, peritoneal dialysis, and hemodialysis - on auditory acuity, and by the possible correlations of arterial hypertension and diabetes,12,13 which are frequently associated with CKD and hearing loss.
To this end, certain criteria were adopted to reduce the interference of other factors with auditory alterations. Subjects older than 60 years were excluded, since 25% of individuals in this age range show alterations in auditory tests due to age.8 Individuals submitted to previous kidney transplantation were excluded due to the use of immunosuppressive drugs pre- and post-transplantation, which may exert an ototoxic effect.5,14 Additionally, transplantation is usually the treatment of last resort, and thus patients have been submitted to other treatments, hindering the analysis of their effects.
Arterial hypertension and diabetes mellitus are the main causes or consequences of CKD,1 and therefore were maintained in the study and considered in the data analysis.
Possible changes in hearing assessment have been described by some authors soon after dialysis; these findings could be attributed to the drugs used or to the ionic concentrations of sensory cells.15,16 However, most studies did not demonstrate a significant effect of a single dialysis session on hearing.15-18 For this reason, and because patients are usually tired and stressed after a dialysis session, subjects were not evaluated at this time.
When the type of CKD treatment was considered, the subgroups were found to be similarly affected by hearing loss, as also reported by Mancini et al.19 and by Nikolopoulos et al.20 However, the results show that audiometry findings of the conservative group were significantly worse than those of the control group. The authors believe that the conservative therapy may cause accumulation of toxic substances in the bloodstream, since these substances are not efficiently eliminated by the kidneys or by dialysis, consequently impairing auditory functions.
The peritoneal dialysis group was least affected by negative TEOAEs, and the hemodialysis group was the most affected, although the difference was not significant, as also reported by Ozturan & Lam15 and by Naderpour et al.21
Although hemodialysis may be a more aggressive method regarding the cochlea by possibly causing ionic changes in the cell membrane,19,20,22,23 this finding was not observed in the present study when using TEOAEs.
In the ABR, the conservative group differed from the hemodialysis group, with an increased III-V interval, suggesting injury in central portions of the brainstem auditory pathway.24
CONCLUSION
The conservative treatment group presented worse hearing threshold and abnormal ABR, reinforcing that patients undergoing treatment for chronic renal disease need a complete hearing assessment for better understanding of the disease and its effects on the auditory system.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
REFERENCES
1. Romão Junior JE. Chronic kidney disease: definition, epidemiology, and classification. J Bras Nefrol. 2004;26:1-3.
2. Alport AC. Hereditary familial congenital haemorrhagic nephritis. BMJ. 1927;1:504-6.
3. Gatland D, Tucker B, Chalstrey S, Keene M, Baker L. Hearing loss in chronic renal failure-hearing threshold changes following haemodialysis. JR Soc Med. 1999;84:587-9.
4. Zeigelboim BS, Mangabeira-Albernaz PL, Fukuda Y. High frequency audiometry and chronic renal failure. Acta Otolaryngol. 2001;121:245-8.
5. Gafter U, Shvili Y, Levi J, Talmi Y, Zohar Y. Brainstem auditory evoked responses in chronic renal failure and the effect of hemodialysis. Nephron. 1989;53:2-5.
6. Komsuoglu SS, Mehta R, Jones LA, Harding GF. Brainstem auditory potentials in chronic renal failure and maintenance hemodialysis. Neurology. 1985;35:419-23.
7. Antonelli AR, Bonfioli F, Garrubba V, Ghisellini M, Lamoretti MP, Nicolai P, et al Audiological findings in elderly patients with chronic renal failure. Acta Otolaryngol. 1991;476:54-68.
8. Thodi C, Thodis E, Danielides V, Pasadakis P, Vargemezis V. Hearing in renal failure. Nephron Dial Transplant. 2006;21:3023-30.
9. Sousa LCA, Piza MR, Alvarenga KF. Cóser PL. Otoacoustic emissions: hearing electrophysiology and otoacoustic emissions, principles and clinical applications. São Paulo: Novo Conceito; 2008. p. 110-29.
10. Katz J. Auditory brainstem response (ABR): Neurodiagnosis and applications intraoperative. Handbook of clinical audiology. 4th edition. São Paulo: Manole; 1999. p. 349-71.
11. Hood L. The normal auditory brainstem response. In: Clinical applications of the auditory brainstem response. San Diego: Singular; 1998. p. 126-44.
12. Lin C, Hsu HT, Lin YS, Weng SF. Increased risk of getting sudden sensorineural hearing loss in patients with chronic kidney disease: A population-based cohort study. Laryngoscope. 2013;123:767-73.
13. Vilayur E, Gopinath B, Harris DC, Burlutsky G, McMahon CM, Mitchell P. The association between reduced GFR and hearing loss: a cross-sectional population-based tudy. Am J Kidney Dis. 2010;56:661-9.
14. Bains KS, Chopra H, Sandhu JS, Aulakh BS. Cochlear function in chronic kidney disease and renal transplantation: a longitudinal study. Transplant Proc. 2007;39:1465-8.
15. Ozturan O, Lam S. The effect of hemodialysis on hearing using pure-tone audiometry and distortion-product otoacoustic emissions. ORL J Otorhinolaryngol Relat Spec.1998;60:303-13.
16. Serbetçioglu MB, Erdogan S, Sifil A. Effects of a single session of hemodialysis on hearing abilities. Acta Otolaryngol. 2001;121:836-8.
17. Rossini M, Stefano D, Febbo A, Paolo D, Bascini M. Brainstem auditory responses (BAERs) in patients. Electroencephalogr Clin Neurophysiol. 1984;57:507-14.
18. Gierek T, Markowski J, Kokot F, Paluch J, Wiecek A, Klimek D. Electrophysiological examinations (ABR and DPOAE) of hearing organ in hemodialysed patients suffering from chronic renal failure. Otolaryngol Pol. 2002;56:189-94.
19. Mancini M, Dello Strologo L, Bianchi P, Tiere L, Rizonni G. Sensorineural hearing loss in patients reaching chronic renal failure in childhood. Pediatr Nephrol. 1996;10:38-40.
20. Nikolopoulos TP, Kandiloros DC, Segas SV, Nomicos PN, Ferekidis EA, Michelis KE, et al. Auditory function in young patients with chronic renal failure. Clin Otolaryngol. 1997;22:222-5.
21. Naderpour M, Mortazavi F, Jabbari-Moghaddam Y, Sharifi-Moghaddam MH. Auditory brain stem response and otoacoustic emission results in children with end-stage renal disease. Int J Pediatr Otorhinolaryngol. 2011;75:704-7.
22. Johnson DW, Wathen RL, Mathog RH. Effects of hemodialysis on hearing threshold. ORL J Otorhinolaryngol Relat Spec.1976;38:129-39.
23. Erkoç MF, Bulut S, Imamoğlu H, Gümüş C, Kayataş M. CT assessment of bone remodeling in the otic capsule in chronic renal failure: association with hearing loss. AJR Am J Roentgenol. 2013;200:396-9.
24. Jakić M, Mihaljević D, Zibar L, Jakić M, Kotromanović Z, Roguljić H. Sensorineural hearing loss in hemodialysis patients. Coll Antropol. 2010;34:165-71.
1. Department of Ophthalmology, Otolaryngology, Head and Neck Surgery, Faculdade de Medicina de Botucatu, Universidade Estadual de São Paulo (UNESP), São Paulo, SP, Brazil
2. Department of Clinical Medicine, Faculdade de Medicina de Botucatu, Universidade Estadual de São Paulo (UNESP), São Paulo, SP, Brazil
Corresponding author.
P.S. Lopez
E-mail: priscilasuman@gmail.com
Received 20 May 2013.
Accepted 1 October 2013.
Print: ![]()