

Year: 2002 Vol. 68 Ed. 3 - (22º)
Relato de Caso
Pages: 436 to 439
 PDF PT
PDF PT Leiomyoma of the paranasal sinuses. A case report and review of the literature
Author(s):
Marconi T. Fonseca (1),
Paulo A. K. Araújo (2),
Aureliano C. Barreiros (3)
Keywords: leiomyoma, nose, paranasal sinuses
Abstract:
Leiomyomas are rare tumors of the nasal cavity and paranasal sinuses. The diagnosis depends on histopatologic study and imunohystoquimic tests. The surgical excision of the tumor has been the appropriate treatment. Only 23 cases have been reported in literature. A new case is presented and the literature is reviewed.
![]()
INTRODUCTION
Leiomyoma is a benign tumor of smooth muscles, frequently located in the digestive tract and uterus, but it may be occasionally found on skin and subcutaneous tissue, and rarely in the paranasal sinuses or nose4, 5, 6, 8. Less than 1% of all cases of leiomyoma affect the neck and head region, and out of them, only 3% are in the nasal cavity and paranasal sinuses8.
According to most authors, the origin of the tumor is the smooth muscle of the blood vessel walls4, 6.
There are 23 cases of nasosinusal leiomyoma described in the literature in English since 1966. There is prevalence of tumor in females, normally manifested between the 4th and 6th decades of life and affecting especially the inferior turbinate and the nasal cavity.
The purpose of the present study was to describe a case of leiomyoma of left anterior ethmoid sinus and to review the literature.
CASE REPORT
A 29-year-old woman was seen by us at the Service of Otorhinolaryngology, Hospital Socor, presenting complaints of bilateral intermittent headache, treated with regular analgesics and related to pre-menstrual tension and tiredness. She did not report nasal obstruction, rhinorrhea or epistaxis. Past history of compensated allergic rhinitis.
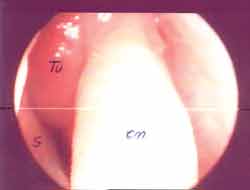
Anterior rhinoscopy was performed with 0o rigid endoscope and we detected bulging above and medially to the upper part of the left middle turbinate, where it touched the region, presenting the same aspect as the surrounding mucosa (Figure 1). The tumor extended medially up to the nasal septum.
Paranasal sinuses CT scan showed expansive lesion of left anterior ethmoid cell (agger nasi), which was bulged and filled with soft part density material, deviating the perpendicular ethmoid lamina to the right and obstructing the left frontal-nasal recess (Figures 2 and 3). Differential diagnosis was made with mucocele and other benign tumors, such as fibroma, neurofibroma, meningocele and adenoma.
Performed under general anesthesia and through nasosinusal endoscopic surgery, we excised the lesion. It was a smooth tumor measuring 2x5x5cm. The patient was discharged from hospital the next day and maintained nasal packing for the first 48 postoperative hours, which were uneventful.
Microscopically, we detected neoplasia that consisted of spindle cell elements, partially lined by respiratory epithelium and formed by elongated cells, no atypia, amidst connective stroma and rare mitoses. Immunohistochemistry revealed positive response to HHF-35 (muscle actin) and collagen IV. Histopathology findings were compatible with diagnosis of leiomyoma.
Seven months after the surgical procedure, the patient remains asymptomatic and presents normal anterior rhinoscopy (Figure 4).Table 1. Report of cases of nose and paranasal sinuses leiomyoma.
F: female / M: male
Figure 1.
Figure 2.
Figure 3.
DISCUSSION
These tumors are rare in the nasal cavity probably because of the scarcity of smooth muscle in the region2, 4, 6, 8, 9. A number of hypothesis have been proposed for the origin of leiomyoma in the nasal cavity. The most accepted one is that the tumor is formed from the smooth muscle of blood vessel walls4, 6. Other hypotheses are the presence of aberrant undifferentiated mesenchyma 1, 6, 8, 9, 11 or the origin from the hair follicle of pili erector muscle (in case of tumors located in the nasal vestibule)6.
Maesaka et al. (1966) were the first authors to describe a case of intranasal angioleiomyoma 3, 5, 7. Later, other 22 cases were documented, apart from the present case (Table 1).
Including our case, there were 16 female patients (66.6%) and 6 male patients (25%). In two other cases, there was no information about gender. Age of patients ranged from 5 to 77 years, mean age of 51.3 years, and only one case in child and the others in patients older than 29 years. The most affected regions were inferior turbinate (7), nasal cavity (5), paranasal sinuses (4), vestibule (3), middle turbinate (2), septum (2) and choana (1). Increased incidence of leiomyoma in inferior turbinate is a result of the abundance of vascular smooth muscle in the region6, 7. Clinical manifestations are varied, and the most common symptoms are nasal obstruction and epistaxis. Pain, including headache, is a frequent symptom in tumors that affect the nasal vestibule and paranasal sinuses.
Radiology techniques, such as CT scan and magnetic resonance imaging, do not aid diagnosis, but they are important to define extension of damage and treatment plan7.
Owing to the lack of specificity of clinical manifestations and radiological aspect, biopsy is necessary for diagnosis. Microscopically, they are tumors that consist of spindle cells with eosinophilic cytoplasm and cigar-shaped nucleolus. The nucleus has open chromatin with a small nucleolus. Cells are arranged in fascicles. Nuclear atypia is absent and mitoses are rare. Significant vascularization may be present and the abundant nasal mucosa irrigation, with many vessels, may create difficulties for the diagnosis by pathology. Immunohistochemistry analysis for specific muscle actin and desmin determine the diagnosis of smooth muscle neoplasia 7. Leiomyomas are divided into vascular and non-vascular. In the nasal cavity, the most frequent type is the vascular type, which presents as a solitary lesion of the subcutaneous layer. They are more frequently found in women than in men4, 8. The presence of enlarged nuclear atypia and mitosis figures suggest malignancy7, 9.
The treatment of choice for nasal leiomyoma is surgical excision because according to the literature there is no recurrence of a lesion that is completely removed. The surgical approach, be it nasosinusal endoscopic surgery or lateral rhinotomy access, will depend on tumor extension and location, as well as the need to better control bleeding 6, 7, 8, 9.
CLOSING REMARKS
We could conclude that nasal and paranasal sinuses leiomyomas are rare tumors that present nonspecific radiological findings and clinical manifestations. Diagnosis is made through tumor biopsy for histopathology and immunohistochemistry study. The treatment of choice is surgical, with total tumor excision.
REFERENCE
1. Barr GD, More IA, McCallum HM. Leiomyoma of the nasal septum. J Laryngol Otol 1990;104(11):891-3.
2. Fu YS, Perzin KH. No epithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx: and clinic pathologic study. IV. Smooth muscle tumors (leiomyoma, leiomyosarcoma). Cancer 1975;35(5):1300-8.
3. Hanna GS, Akosa AB, Ali MH. Vascular leiomyoma of the inferior turbinate-report of a case and review of literature. J Laryngol Otol 1988;102(12):1159-60.
4. Harcourt JP, Gallimore AP. Leiomyoma of the paranasal sinuses. J Laryngol Otol 1993;107(8):740-1.
5. Lijovetzky G, Zaarura S, Gay I. Leiomyoma of the nasal cavity. Report of a case. J Laryngol Otol 1985;99:197-200.
6. Llorente JL, Suarez C, Seco M, Garcia. A. Leiomyoma of the nasal septum: report of a case and review of the literature. J Laryngol Otol 1996;110(1):65-8.
7. MaCaffrey TV, McDonald TJ, Unni KK. Leiomyoma of the nasal cavity. Report of a case. J Laryngol Otol 1978; 92(9):817-9.
8. Melgarejo MP, Hellin MD, Sarroca CE. Angioleiomyoma of the inferior nasal turbinate. A case report and review of the literature. Acta Otorrinolaringol Esp 1997;48(7):571-3.
9. Tang SO, Tse CH. Leiomyoma of the nasal cavity. J Laryngol Otol 1988;102(9):831-3.
10. Trott MS, Gewirtz A, Lavertu P, Wood BG, Sebek BA. Sinonasal leiomyomas. Otolaryngol Heard Neck Surg 1994;111(5):660-4.
11. Van Ingen G, Stel HV, Tiwari RM. Atypical leiomyoma of the choana. J Laryngol Otol 1991;105(12):1065-7.
[1] Head of the Service of Otorhinolaryngology and Head and Neck Surgery, Hospital Socor.
[2] Joint Physician, Service of Otorhinolaryngology and Head and Neck Surgery, Hospital Socor.
[3] Physician, Specialization studies under course, Service of Otorhinolaryngology and Head and Neck Surgery, Hospital Socor.
Affiliation: Study conducted at Service of Otorhinolaryngology and Head and Neck Surgery, Hospital Socor - Belo Horizonte - Minas Gerais - Brazil.
Address correspondence to: Dr Marconi Teixeira Fonseca - Rua Juiz de Fora, 33 - Belo Horizonte - Minas Gerais - Brazil - CEP 30180-060 - Tel. (55 31)3330-3005 - Fax: (55 31) 3295-1941.- E-mail: otologica@uol.com.br

Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial