

Year: 2002 Vol. 68 Ed. 3 - (2º)
Editorial
Pages: 299 to 302
 PDF PT
PDF PT Microendoscopic surgery of the paranasal sinuses - basic concepts
Author(s): Dr. Aldo Stamm*
Keywords: -
![]()
INTRODUCTION
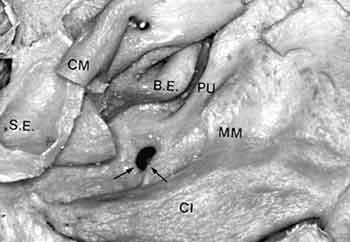
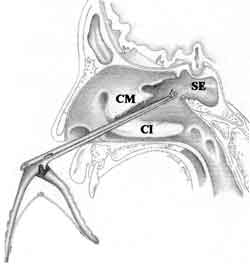
The so-called ostio-meatal complex or unit, the anatomical region limited by the inferior and middle conchae, is a set of structures in which the following are classically included: ethmoidal bulla, unciform process, infundibulum, semilunar hiatus (superior and inferior), drainage ostia, anterior ethmoidal cells (agger nasi) and Haller cells1. In the present study, the author has also included the meatal aspect of the middle concha and frontal recess2, 3 (Chart 1, Figure 1). The importance of this complex is that practically all paranasal sinuses communicate with the nasal cavity through it, and in situations such as viral, allergic, fungal and bacterial diseases and nasal septum deviations, there may be compression of the ostio-meatal structure favoring the development of sinus pathology.
Preoperative Examination
Prognostic parameters are important for the preoperative examination and they can be seen in Table 1, including clinical history data, findings of the endoscopic examination (flexible or rigid) and imaging technique data. Computed tomography scan (CT scan), especially at coronal section, identifies and assesses middle meatus and inferior meatus of the paranasal sinuses. Axial projections are useful to check the correlation between orbital wall of the ethmoidal sinus and orbit, location of optical nerves and internal carotid artery4. CT scan with sagittal reconstruction enables the analysis of the frontal recess at the anterior portion of ethmoidal bulla and the relation of anterior ethmoid and the orbit and skull base.
General indications of nasosinusal surgery
The main objectives of surgical treatment are restoration of ventilation and drainage of paranasal sinuses1, 2, 5, 6. The main surgical indications are:
· Inflammatory and/or infectious disease (polyposis, fungi, etc.);
· Complications;
· Rhinosinusitis non-responsive to appropriate clinical treatment.
It is important for the patients to be aware of the type of nasosinusal surgery they are going to undergo, as well as their implications.
Surgical Procedures
Surgical treatment, when indicated, using operative microscope and/or endoscope includes minimal surgical procedures and more aggressive approaches, depending on the extension of the disease.
The main surgical procedures for diseases related to the ostio-meatal complex are listed in Table II.
Conservative or little-invasive surgery: operative intervention that tries to reduce mucosa contact areas at the level of paranasal sinuses drainage region7. Among the procedures, we include removal of unciform process, ethmoidal bulla (bullotomy), meatal aspect of middle concha and sectorial septoplasty.
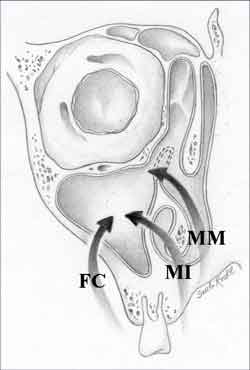
Middle, lower, anterior or combined antrostomy: these are surgical accesses to the maxillary sinus. Anterior antrostomy may be limited to canine fossa punch with endoscope-guided trochar (Figure 2). Middle antrostomy (wide opening) is normally performed in cases of polyposis, fungal disease and sinusitis with affection of mucoperiosteum. Ostioplasty, that is, expansion of the main drainage canal of the maxillary sinus, is used in cases of recurrent sinusitis, for example.
Partial Ethmoidectomy: it refers to the removal of ethmoidal cells, especially the anterior ones, with preservation of the mucoperiosteum of the orbital wall and skull base, also preserving the middle concha.
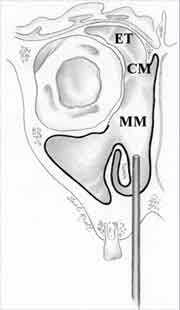
Total Ethmoidectomy: anterior and posterior ethmoidectomy with preservation of mucoperiosteum on the ethmoidal sinus walls (orbit, anterior skull base). Normally indicated in chronic rhinosinusitis and/or polyposis that compromise the whole ethmoidal sinus. Middle conchoplasty is frequently performed in that type of intervention (Figure 3).
Radical Ethmoidectomy: it is normally applied in recurrent grade V polyposis 2, 3, it implies removal of anterior and posterior ethmoidal cells together with the mucosa, trying to preserve the periosteum of the ethmoid orbital wall, skull base, especially at the level of frontal recess. The maxillary sinus mucoperiosteum is normally preserved. We can still remove the middle concha, preserving its attachment (Figure 4).
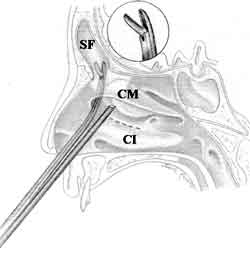
Frontal recess and sinus surgery: it is still a controversial procedure, especially because of the possible complications such as postoperative stenosis caused by anomalous scaring, granulation tissue and osteogenesis 8, 9. For simple secretion drainage, the frontal sinus may be probed with Ritter palpator. In intrasinusal affections, the opening should be widened by the frontal recess, anteriorly to the ethmoid bulla (technique of integral ethmoid bulla). For intrasinusal procedures, the techniques proposed by Draf (I, II and III)8 (Figure 5) can be used. If the frontal recess is small and difficult to be located, external sinus trepanation can be associated to irrigation and endoscopic control.
Sphenoid Sinus: endonasal surgery can be performed through three approaches. Direct transnasal access, applied to restricted diseases of the sphenoid sinus; transethmoidal, combined with direct access. Transseptal approach is rarely used in cases of rhinosinusitis.
Re-operations: as a result of loss of anatomical repairs, they are normally high risk surgeries and the critical areas involved are orbit, ethmoid fovea, lamina cribrosa and posterior-lateral wall of the sphenoid sinus10.
Figure 1.
Figure 2.
Figure 3.
Figure 4.
Figure 5.
Figure 6.
Postoperative Care
Postoperative care (Table 1) is as important as operative intervention. The imaging techniques should be ordered in case of poor evolution or in the presence of complications, such as for example, damage of orbit and its content, optical nerve, anterior skull base, cerebral tissues and vessels and bleeding9, 11.
Closing Remarks
Surgeries at the level of the ostio-meatal complex can contribute to the treatment of many nasosinusal pathologies, but if the muco-ciliary system is affected, the operative intervention may not be beneficial. The removal of ethmoidal sinus mucosa has been described in such cases12,13,14.
The results of nasosinusal micro endoscopic surgery are directly correlated to prognostic preoperative and transoperative factors and postoperative control2 (Table 1).
REFERENCES
1. Kennedy DW. Functional endoscopic sinus surgery. Theory, technique and patency. Arch Otolaryngol 1985;111:576.
2. Stamm A. Microcirurgia Naso-Sinusal. Rio de Janeiro: Revinter; 1995. p. 436.
3. Stamm A.Microendoscopic Surgery of the paranasal Sinuses. In: Stamm A, Draf W (eds.). Microendoscopic Surgery of the paranasal Sinuses and the Skull Base. Heildelberg, Springer, 2000. p.201-36.
4. Klossek JM, Fontanel JP, Ferrie JC. Explorations radiologiques des cavités sinusiennes et nasales. Enc med chirur 1993;20:422-A-10.
5. Stammberger H, Posawetz W. Functional endoscopic sinus surgery. Concepts, indications and results of Messerklinger technique. Eur arch otol rhinol laryngol 1990;247:263.
6. Wigand ME. Endoscopic surgery of the paranasal sinuses and anterior skull base. New York: Thieme; 1990.
7. Setliff RC, Parsons DS. The "hummer": new instrumentation for functional endoscopic sinus surgery. Am J Rhinol 1994;8:275.
8. Draf W. Endonasal micro-endoscopic frontal sinus surgery. The Fulda concept. Oper Tech Otolaryngol Head Neck Surg 1991;2:234-40.
9. Stankiewicz JA. Complications in endoscopic sinus surgery. Otolaryngol Clin N Amer 1989;22:749.
10. Lofchy NM, Bumsted RM. Revision and open sinus surgery. In: Otolaryngology Head & Neck Surgery, Cummings CW et al. (eds.). St. Louis.
11. Lawson W. The intranasal ethmoidectomy: an experience with 1,077 procedures, Laryngoscope 1991;101:367.
12. Rouvier P, Vandeventer G, El Khoury J. Les résultat à long terme (sur 5 ans) de l'ethmoidectomie dans la polypose nasale invalidante. J Fr Orl 1991;40:102-5.
13. Jankowski R, Pigret D, Decroocq F. Comparison of functional results after ethmoidectomy and nasalization for diffuse and severe nasal polyposis. Acta Otolaryngol (Stockh.) 1997;117:118.
14. Klossek JM, Peloquin L, Firedman WH et al. Diffuse nasal polyposis: postoperative long term results after endoscopic sinus surgery. Otolaryngol Head Neck Surg 1997;117:355-61.

Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial