

Year: 2010 Vol. 76 Ed. 5 - (22º)
Artigo Original
Pages: 663 to 666
 PDF PT
PDF PT  PDF EN
PDF ENProfile of audiometric thresholds and tympanometric curve of elderly patients
Author(s): Tatiana Marques Guerra1, Lucimar Pires Estevanovic2, Marcela de Ávila Meira Cavalcante3, Rafaela Carolina Lopez Silva4, Izabel Cristina Campolina Miranda5, Victor Gandra Quintas6
Keywords: hearing loss, aged, speech, sensorineural, hearing.
Abstract:
Aim: to analyze the audiological profile of elderly patients seen in a clinic from an audiology school clinic in the city of Belo Horizonte. Methods: we studied all the charts from the patients who underwent audiologic assessment from April of 2004 and August of 2007 in an audiology clinic in the city of Belo Horizonte. Results: We studied the 313 audiological tests from patients 60 years of age or over. The results from the audiological evaluations as to the type of hearing loss were: auditory thresholds within normal standards - 22.28%; sensorineural hearing loss - 60.62%; mixed hearing loss - 14.70%, conductive hearing loss - 2.40%. The level varied between normal and profound. As to the tympanometry, 83.22% had the type A curve, and the other types of curves obtained made up a total of 16.3%. The percentage of individuals who did not undergo the test was 0.48%. 1.76% of the patients who had unilateral hearing loss and 98.24% had bilateral hearing loss. Conclusions: we found a greater prevalence of sensorineural hearing loss, and the degree of the loss varied from mild to profound, with a prevalence of the moderate degree.
![]()
INTRODUCTION
Hearing loss is the partial or total hearing disability, which can be associated with birth, acquired diseases, use of ototoxic drugs or aging. This change can affect any age range. Children with hearing loss can have development difficulties, while elderly patients have natural hearing loss with aging, called presbycusis1-2.
Quality of life improvement, improvement in health conditions and chronic and infectious diseases control made people live longer. However, the effects of aging on the sensorial capacities did not change, causing diseases stemming from this aging, which is the case of the hearing loss which affects the elderly2.
Hearing loss is one of the sensorial deficits which has the most impact on the lives of people; because it impairs the person's capacity to effectively engage in communication. Thus, there is a reduction on speech intelligibility, impairing verbal communication, interfering in receiving information, forming and expressing one's ideas. Moreover, there is patient isolation, reduced socialization and intolerance to moderate to high-intensity sounds1-3.
Presbycusis is the natural aging of the human ear, in other words, a hearing disorder associated to cochlea degeneration, which affects mainly the base of it, impairing hearing perception in the high frequencies as age increases1-4.
The main symptoms the elderly have associated with presbycusis are: difficulties in participating in talks or speaking on the phone; understanding words; locating a sound source; hearing alarms, the telephone, doorbell, approaching vehicles; and there is the need to raise the volumes of TV or radio1-2,5.
Presbycusis is defined as sensorineural hearing loss, which varies between mild to profound in the low as well as the high frequencies, having a gradual and progressive onset, symmetrical, descending and bilateral for high frequency sounds (3 to 8KHz), often times followed by difficulties in speech recognition6-10.
According to what has been previously reported, presbycusis has a downwards characteristic, being so described by the classification criterion of the hearing loss level of an American study11. However; in the present study, we will approach the classification criterion of a Brazilian study10.
The elderly's audiologic evaluation must involve subjective and objective exams in order to define his/her audiologic thresholds. Thus, some factors must be observed, such as understanding and the execution of the orders given to the patient in order to obtain an accurate result on the functional use of hearing and understanding. There must be certainty on the orders given to the patient and to check whether or not they are being understood, because the linguistic implications are directly related to the degree of hearing loss, which can vary between mild to severe12-13.
The audiologic findings described in the literature show the prevalence of type A tympanometric curves, which configuration represents normality or sensorineural alteration, such as presbycusis, for instance14.
Once established that the elderly Brazilian population in recent years has been growing faster than the other age ranges15, it is necessary to better study and investigate this population in order to provide them with better quality of life.
Thus, based on the literature investigated, this study aims at tracing the audiological profile, according to the hearing threshold and the type of tympanometric curve of elderly patients who underwent auditory evaluation in an audiology clinic.
MATERIALS AND METHODS
The present study was carried out after being approved by the Ethics Committee of the teaching institution where it was held, under protocol #O 0107.0.213.000-07. Thus, we surveyed the data according to the charts of the hearing exams, carried out in the institution by the undergraduate students, under the guidance of the speech and hearing professor in charge, between August of 2004 and August of 2007, adding up to a total of 313 hearing assessments and 626 ears.
All the assessments were done using the following equipment: Midimate 622 audiometer and the AZ7 immittance meter device, in order to evaluate the hearing threshold and to study the type of tympanometric curve, respectively.
The minimum age found was 60 years and the maximum was 94 years, with a mean age of 69.82 years. This age was selected in order to have a better sample homogeneity, as well as a complying with the greater demand from the department where the study was carried out.
According to the classification criterion utilized16, the frequencies of 0.25, 0.5, 1 and 2 KHz were considered low frequencies; and 3, 4, 6 and 8 KHz were considered high frequencies, and the type and degree of hearing loss were analyzed from the mean values of each one of them. Thus, since we had 626 ears, there were a total of 1252 events, since each type of frequency (highs and lows) was analyzed separately.
For immittance measuring we used the classification criteria of the tympanometric curves17, which classifies type A curve as the one with pressure between +50 and -70 daPa with compliance between 0.3 and 1.3 ml; As type curve - pressure between +50 and -70 daPa with compliance below 0.3 ml; type Ad curve - pressure between +50 and -70 daPa with compliance above 1.3 ml; type C curve - pressure below -70 daPa with compliance between 0.3 and 1.3 ml; type B curve - there is no maximum compliance peak.
The present study was carried out through statistical bases which characterize its intrinsic quality: sensitivity and specificity. The findings were described by analysis of frequency and occurrence, by means of descriptive graphics and tables.
RESULTS
In most of the individuals (a little more than 60%) there were hearing thresholds of low frequency higher than the auditory threshold in the high frequencies, characterizing a descending type of curve.
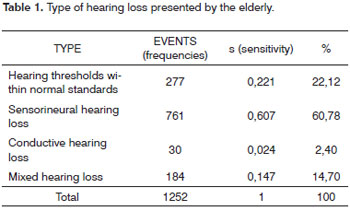
As to the type of hearing loss, the results from the statistical analysis revealed that 60.78% of the population investigated had sensorineural hearing loss; 14.70% had mixed hearing loss; 2.40% had conductive hearing loss and 22.12% of the individuals had hearing thresholds within normal standards (Table 1).
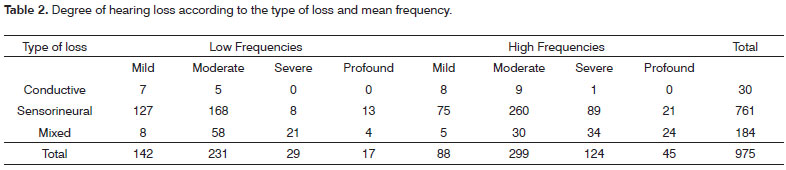
As to the degree of hearing loss, we noticed they were from mild to profound, and the most prevalent one was the moderate degree (Table 2).
Of the 77.88% of the elderly with hearing loss, 1.76% was unilateral and 98.24% were bilateral.
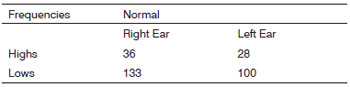
As to the audiometric configurations of sensorineural hearing losses, we can see that 61.66% of the individuals had audiologic configuration suggesting presbycusis, in other words, bilateral, symmetrical and descending, of grade varying between mild to severe. On the chart that follows, we depict the auditory thresholds within normal parameters.
Chart. Hearing thresholds within normal standards in the high and low frequencies.
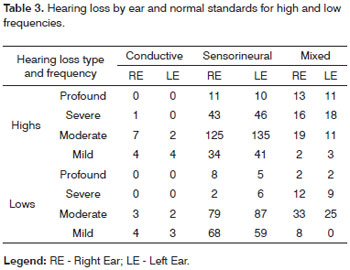
On Table 3 we have the types and degrees of auditory hearing loss per ear in the low and high frequencies.
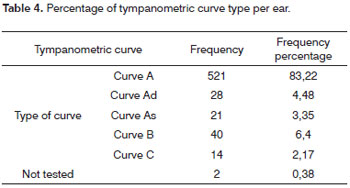
On Table 4 we notice the immittance values found in the population investigated. The type A tympanometric curve was present in 83.22% of the ears (521); while 16.3% (102) had the remaining types of tympanometric curves ("AD, AS, B, C") and 0.48% of the ears (03) did not undergo immittance measuring.
DISCUSSION
The higher quality of life, the improvements in health conditions and the control of chronic and infectious diseases cause a growth in the elderly population. However, the effects of the aging process on the sensorial capacities did not change, causing diseases which stem from this aging, as is the case of the hearing loss which happens to elderly, called presbycusis, which has as characteristics: bilateral, symmetrical, descending and progressive hearing loss1-13,18-20.
According to the bibliography found, we noticed that the percentage of sensorineural hearing loss present in elderly individuals matches those in the present study. One study1 describes that 260 elderly were surveyed, when 64.23% had sensorineural hearing loss. Among the 331 individuals above 60 years seen in another study14, 81% had sensorineural hearing loss. These results corroborate the findings of the present paper.
Through the protocols checked, among the elderly with hearing loss, 98.24% were bilateral, which is confirmed by the literature consulted - where there is a prevalence of hearing loss in both ears of the population studied1,13-15,18-20.
Observing the data as to the type of tympanometric curves, we noticed that 83.22% of the ears studied had type A curve. In another study14 the authors found 78.85% of Type A curve in the elderly, being, therefore, very close values.
In relation to the audiometric configuration, 61.66% of the individuals studied had hearing loss with characteristics of presbycusis, in other words, bilateral, from mild to severe, descending, matching findings in the literature - where we find that presbycusis is characterized by sensorineural, symmetrical, descending and bilateral hearing loss for high frequency sounds (3 to 8 KHz) followed by the speech recognition difficulties1,6-10;13-15,18-21.
It is important to stress that presbycusis represents the natural order of things, it is part of human life and happens in accordance with the aging process1-10; nonetheless, many elderly individuals may live well with this loss, depending on its degree and, even in the more severe cases, there are means which enable an improvement in the quality of life of this population.
CONCLUSION
After doing this study, with elderly seen in a teaching clinic, we noticed a greater prevalence of sensorineural hearing loss, and the degree of loss varied from mild to profound, with a greater prevalence of the moderate type. Still, the high frequencies proved to be the ones more involved when compared to the low ones, in most of the individuals, characterizing descending audiometric curves, typical of presbycusis. It is also worth stressing that the most frequently found tympanometric curve was the Type A.
Therefore, we studied the hearing profile of elderly patients in a given population, thus enabling a bird's eye view on the quality of life of the people in the age range hereby investigated, and we report on a greater prevalence of sensorineural hearing loss varying from mild to profound, with a higher prevalence of the moderate degree.
REFERENCES
1. Amaral LCG, Sena APRC. Perfil Audiológico dos Pacientes da Terceira Idade Atendidos no Núcleo de Atenção Médica Integrada da Universidade de Fortaleza. Fono Atual. 2004;7(27):58-64.
2. Soncine F, Costa MJ, Oliveira TMT. Perfil Audiológico de Indivíduos na faixa etária entre 50 e 60 anos. Fono Atual. 2004;7(28):21-9.
3. Baraldi GS, Almeida LC, Borges ACC. Evolução da perda auditiva no decorrer do envelhecimento. Braz J Otorhinolaryngol. 2007;73(1):64-70.
4. Sousa MGC, Russo ICP. Audição e percepção da perda auditiva em idosos. Rev Soc Bras Fonoaudiol. 2009;14(2):241-6.
5. Calais LL, Borges ACLC, Baraldi GS, Almeida LC. Queixas e preocupações otológicas e as dificuldades de comunicação de indivíduos idosos. Rev Soc Bras Fonoaudiol. 2008;13(1):12-9.
6. Marques ACO, Koziowski L, Marques JM. Reabilitação auditiva no Idoso. Rev Bras Otorrinolaringol. 2004;70(6):1-7.
7. Neves VT, Feitosa AMG. Envelhecimento do Processamento Temporal Auditivo. Psic Teor e Pesq. 2002;18(3):1-15.
8. Almeida EOC, Costa CB, Oliveira SRT. Umeoka MTH. Audiometria Tonal e Emissões Otoacústicas-Produtos de Distorção em Pacientes Tratados com Cisplatina. Arq Int Otorrinolaringol. 2006;10(3):1-7.
9. Kwitko A. Avaliação da Perda Auditiva Ocupacional e da Presbiacusia: Uma Aplicação da Análise de Componentes Principais. Acta Awho. 1997;16(2):54-65.
10. Russo ICP. Distúrbios da audição: A presbiacusia. In: Russo ICP, Ribeiro A. Intervenção fonoaudiológica na terceira idade. Rio de Janeiro: Revinter; 1999. p. 51-79.
11. Lloyd LL, Kaplan H. Audiometric interpretation: a manual of basic audiometry: Press, 1978.
12. Veras RP, Mattos LC. Audiologia do Envelhecimento: Revisão da Literatura e Perspectivas Atuais. Braz J Otorhinolaryngol. 2007;73(1):128-34.
14. Jurca APK, Pinheiro FCC, Martins KC, Herrera LF, Colleone LM, Saes SO. Estudo do Perfil Audiológico de Pacientes com Idade Acima de 60 anos. Salusvita. 2002;21(1):51-8.
15. Scheffer JC, Fialho IM, Scholze AS. Itinerários de cura e cuidado de idosos com perda auditiva. Saúde Soc. São Paulo. 2009;18(3):537-48.
16. Monmensoh-Santos TM, Russo ICP, Bahilo-Neves CS, Botelho DL, F. Martins-Dias FA, Rodrugues FL, et. Al. Estudo Comparativo dos Critérios Utilizados na Classificação do Grau de Perda Auditiva. Anais do IX Congresso Brasileiro de Fonoaudiologia. Vitória (ES), 2001.
17. Jerger J. Clinical experience with impedance audiometry. Arch Otolaryng. 1970.
18. Vitale RF, Andrade F, Quintanilha R. O Papel do Fator da Necrose Tumoral Alfa no Processo de Erosão Óssea Presente no Colesteatoma Adquirido da Orelha Média. Braz J Otorhinolaryngol. 2007;73(1):123-7.
19. Ruschel CV, Carvalho CR, Guarinello AC. A Eficiência de um Programa de Reabilitação Audiológica em Idosos com Presbiacusia em seus Familiares. Rev Soc Brás Fonoaudiol. 2007;12(2):95-8.
20. Costa KRS. Estudo de Avaliações Audiológicas de Sujeitos Atendidos numa Clínica Universitária. Fono Atual. 2002;6(20):31-8.
21. Fuess VLR, Cerchiari DP. Estudo da Hipertensão Arterial Sistêmica e do Diabetes Mellitus como Fatores Agravantes da Presbiacusia. Arq Int Otorrinolaringol. 2003;7(2)116-21.
1. Speech and Hearing Therapist; Audiologist - Pontifícia Universidade Católica de Minas Gerais.
2. Speech and Hearing Therapist; Audiologist - Pontifícia Universidade Católica de Minas Gerais.
3. Speech and Hearing Therapy Student - Pontifícia Universidade Católica de Minas Gerais.
4. MSc in Speech and Hearing Therapy - Pontifícia Universidade Católica de São Paulo; Assistant Professor of Speech and Hearing Therapy - Pontifícia Universidade Católica de Minas Gerais.
5. PhD in Linguistics - Federal University of Minas Gerais; Full Professor of Speech and Hearing Therapy - Pontifícia Universidade Católica de Minas Gerais.
6. Speech and Hearing Therapist; MSc in Human Communication Disorders - Federal University of Santa Maria - RS.
Pontifícia Universidade Católica de Minas Gerais
Send correspondence to:
Tatiana Marques Guerra
Rua Lavras 935
Belo Horizonte MG 32.330-010
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on November 24, 2009
and accepted on June 25, 2010. cod. 6795
Print: ![]()