

Year: 2010 Vol. 76 Ed. 1 - (5º)
Artigo Original
Pages: 25 to 28
 PDF PT
PDF PT  PDF EN
PDF ENCytokine profile in subjects with Cystic Fibrosis and nasal polyposis compared to patients with no nasal disorders
Author(s): Flávio Barbosa Nunes1, Mirian Cabral Moreira de Castro2, Tacimara Moreira da Silva3, Ricardo Nascimento Araújo4, Helena Maria Gonçalves Becker5, Paulo Fernando Tormin Borges Crosara6, Roberto Eustáquio Santos Guimarães7
Keywords: cytokines, cystic fibrosis, nasal polyps.
Abstract:
Although the cytokine profile in nasal polyposis is well documented, little is known about cytokines associated to cystic fibrosis. Aim: Assess the expression of cytokines IL¬4, IL¬5, IL¬6, IL¬8, GM¬-CSF and IFN¬-y, analyzed through RTPCR, in the polyps of patients with cystic fibrosis. Materials and Methods: A cross-sectional, prospective study was carried out with 24 patients, 13 of whom had cystic fibrosis and nasal polyposis (Cystic Fibrosis Group) and 11 had normal otorhinolaryngological exams (Control Group). The average age was 21 years (3¬57); 12 participants were males and 12 were females. The cytokine profile was studied in mucosal fragments (Control Group) or nasal polyps (Cystic Fibrosis Group) through RT¬PCR. Transcriptions were studied for cytokines IL¬4, IL¬5, IL¬6, IL¬8, IFN¬y and GM¬CSF, adjusted for the ߬-actin value. Results: Interleukins 5, 6, 8 and GM¬CSF were similar in both groups (p>0.05). There were lower values of IFN-y¬ (p=0.03) and a strong tendency toward an increase in IL¬4 (p=0.06) in the Cystic Fibrosis Group. Conclusion: Inflammatory and structural cells may produce messenger RNA for IL¬4, blocking the production of other cytokines such as IFN-y, suggesting the participation of this mechanism in the formation of polyps in cystic fibrosis.
![]()
INTRODUCTION
Nasal polyposis (NP) is a chronic inflammatory disease that involves the nasal mucosa. It is characterized by the presence of multiple grayish nasal polyps located bilaterally and originating from the middle meatus1,2. NP involves 0.5% of the population; eosinophilic nasal polyposis (ENP) accounts for 85% of the cases, while non-eosinophilic nasal polyposis (NENP) accounts for the remaining 15%1,2.
Diseases with concurrent NENP include mucoviscidosis or cystic fibrosis (CF). This is a congenital autosomal recessive disease found in 1 of every 2,500 individuals. Patients experience exocrine gland dysfunction, chronic pulmonary obstruction, and pancreas failure. Polyps are present in 20% of the patients3,4.
Various pathogenic mechanisms have been proposed to explain its development, among which are allergy and inflammation. Although the genesis of allergic rhinitis is IgE-specific, its prevalence is of only 1.5% of the patients with polyposis, and similar levels of immunoglobulin E were observed in polyps of both allergic and non-allergic patients5.
The inflammatory micro-environment, cytokines, adhesion molecules, and ion transportation have been recently studied to clarify the pathogenesis of nasal polyps6.
More specifically, eosinophils and mediators such as interleukins 4 (IL-4), 5 (IL-5), 6 (IL-6), 8 (IL-8), granulocytemacrophage colony-stimulating factors (GM-CSF) and interferon gamma (IFN-γ), were given special attention after elevated values were observed in patients with ENP1.
Unfortunately, few papers have looked into NP and the role of cytokines in CF.
Therefore, this study aims to analyze the expression of messenger ribonucleic acid (mRNA) for IL-4, IL-5, IL-6, IL-8, GM-CSF, and INF-γ in patients with cystic fibrosis and control subjects through reverse transcription polymerase chain reaction (RT-PCR).
MATERIALS AND METHOD
This is a cross-sectional study done on 13 patients with NP and 124 patients with CF. Six (46.15%) of the 13 patients were males and seven (53.85%) were females with mean age of 22.45 years (6-57).
The following criteria was used to enroll and exclude subjects from the study.
Enrollment criteria
Diagnosis of CF based on two dosages of electrolytes in sweat with sodium and chlorine levels above 60mEq/l.
Patients with CF and NP.
Exclusion criteria
Upper or lower airway infection, use of topical or systemic glucocorticoids or antihistamines within 30 days of the study.
The control group was made up of 13 individuals who looked for our service to undergo ENT surgery. Nasal examination did not show any alterations for these subjects, and allergies were ruled out after dermal puncture tests7; none of them was taking topical/systemic glucocorticoids or antihistamines. Two patients were excluded due to immediate postoperative acute sinusitis. From the remaining eleven, five (45.45%) were females, six (54.54%) were males, with a mean age of 17.7 years (3-43).
The study was carried out from December, 2003 through December of 2004, and was approved by the Ethics in Research Committee of the University of Minas Gerais Medical School Hospital, under protocol # nº. 209/03. All the patients signed the post-informed consent form to participate in this study.
The cytokine profile was analyzed looking at mucosa fragments from the middle turbinate (control group) and polyp specimens (cystic fibrosis group) to collect mRNA for further analysis using RT-PCR.
Polyp fragments from the CF group were collected at the ENT outpatient ward using an EXPLORENT® forceps (Karl Storz, Miami, Florida, USA) and a Storz 30º, 4.0 mm endoscope (Karl Storz, Miami, FL, USA).
Normal nasal mucosa fragments from control group patients were collected in the middle turbinate using an EXPLORENT® forceps (Karl Storz, Miami, FL, USA) and a Storz 30º, 4.0 mm endoscope (Karl Storz, Miami, FL, USA) during ENT surgical procedures. Patients were under general anesthesia and the collected specimens were sent for further testing using RT-PCR.
Transcriptions for cytokines IL-4, IL-5, IL-6, IL-8, GM-CSF, and INF-γ were analyzed and adjusted by the β-actin coefficient8. After cooling the samples to -80°, RNA extraction was done using reagent Trizol® (Invitron Corporation, Carlsbad, California, USA) in accordance with the manufacturer's recommendations. RNA concentration in the samples was quantified in a spectrophotometer for the wavelength of 260 nm and integrity was assessed through denaturating gel electrophoresis using 0.8% agarose8. Deoxyribonucleic acid (DNA) was synthesized from 1.25µg of total RNA using random hexamer initiators (Promega Corporation, Madison, WI, USA) and reverse transcriptase system SuperScript II (Invitron Corporation, Carlsbad, CA, USA) as recommended by the manufacturers. PCR products were analyzed through silver-stained 8% polyacrylamide gel electrophoresis. The gels were photographed and results analyzed through densitometry using device Alpha-Digidoc 1201 TM (AlphaInotech, San Leandro, CA, USA). The resulting PCR bands for each sample were analyzed through densitometry using program AlphaEaseFC release 3.3.0 (AlphaInotech, San Leandro, CA, USA).
ANOVA (analysis of variance) parametric tests and Student's T-test were used in the statistical analysis to com pare two mean values and 5% was adopted as statistical significance level.
RESULTS
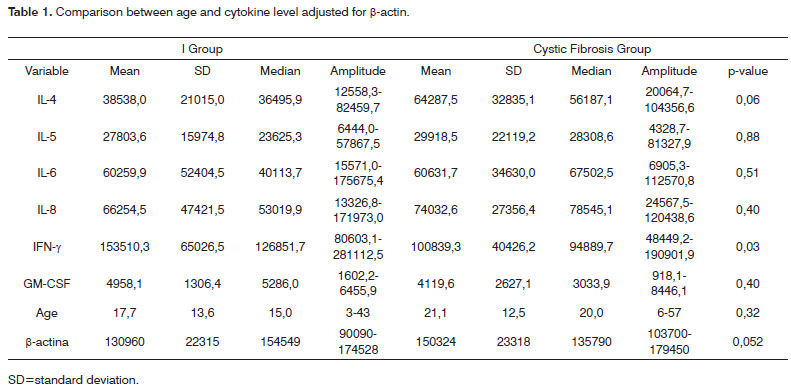
Table 1 shows that no statistically significant differences were found when IL-5, IL-6, IL-8 and GM-CSF values were compared between groups (p>0.05).
Table 1 also shows higher values for IL-4 (p=0.06) strongly tending to statistical significance and low values for INF-γ (p=0.03) in the cystic fibrosis group when compared to the control group.
DISCUSSION
Cytokines are secreted by inflammatory cells (lymphocytes, eosinophils, and neutrophils) and constituting cells (mastocytes, fibroblasts, epithelial cells, and macrophages) 9. They regulate biologic processes such as growth, cell activation, chemotaxis, inflammation, immunity, tissue repair, fibrosis, and morphogenesis10. The profile of cytokines and inflammatory cells in ENP is well documented in the literature; conversely, very little is known on the pathogenesis of NP and cytokines in CF patients.
Interleukin 8 is the main cytokine related to NP in CF patients. Various authors have observed increased levels of IL-8 and neutrophils when comparing such patients to subjects with ENP11. The main sources of IL-8 are neutrophils and their byproducts such as elastase, oxidants, and IL-812,13.
Sobol et al.12 looked at individuals with chronic sinusitis and CF and compared them to healthy subjects and showed that nasal disease in CF consists of a neutrophilic infiltrate with increased levels of IL-8, similarly to what is found in patients with lung disorders12.
It is worth mentioning that, similarly to what was found in this study, Noah et al.14 and Black et al.15 showed that increased IL-8 levels are consequent acute associated bacterial infection. In the absence of infection - infection being one of the exclusion criterion in this study - both nasal and lung secretions showed normal IL-8 levels14,15.
The respiratory epithelium impacts polyp inflammatory mediation, mainly in ENP, through the production of cytokines such as IL-6 and GM-CSF16,17. Thus, differently from Bernstein et al.6 and Mulloi et al.16 in which large epithelial lesions and consequent increases in GM-CSF and IL-6 were respectively shown, for nasal polyps this study showed a wide range of normal values for such cytokines, suggesting greater epithelium integrity on NP in CF patients and a lesser participation of IL-6 and GM-CSF in this micro inflammatory environment.
Eosinophils had genetic expression for IL-5 in patients with ENP10,18,19.
According to Jankowski et al.20, eosinophils, even at lower levels as found in NP CF subjects, play an important role in inflammation in the development of polyps20.
As indicated on Table 1, no increases were seen on IL-5 as similarly found by Clayes et al.4 and Sobol et al.12. These results suggest that if eosinophils have an important role in NP associated with CF, different mechanisms exist for eosinophilia and are independent from IL-5.
Interestingly enough, as seen on Table 1, we found that increased levels of IL-4 tended towards statistical significance and low levels of INF-γ in the cystic fibrosis group.
Similarly as found in our study, Clayes et al.4 and Dellacono et al.21 showed lower levels of INF-γ in patients with CF and nasal polyposis when compared to subjects with eosinophilic polyps. INF-γ was increased in CF patients only in acute sinusitis events12.
In contrast, we could not find papers in the literature showing altered IL-4 values in patients with nasal polyposis and cystic fibrosis.
Bacterial lipopolysaccharides (LPS) bind to the receptor of CD4+ T-cells (T-helper 2 cells) and stimulate the production of IL-4, leading to increased IgE values22-24. By its turn, INF-γ introduces an opposite effect through stimulation of T-helper 1 cells (Th1) and by blocking the production of IgE and T-helper 2 cells (Th2), principally IL-4 and IL-524.
Originally defined as an antiviral agent, INF-γ plays an important role in stimulating bactericide action by macrophages, antigen presentation through MHC (major histocompatibility complex) molecules, and leukocyte-endothelium interaction25,26. It suppression leads to bacterial proliferation due to the absence of intracellular clearance or by epithelial ionic alterations25,26.
Thus, reductions on INF-γ levels as observed in this study would explain the presence of bacteria or bacterial LPS in the intracellular realm. These bacteria would stimulate the production of IL-4 by Th2 cells. The outcome would be intense inflammation with increased levels of eosinophilic cationic protein (ECP), total IgE, led by increased levels of IL-4 and reduced levels of INF-γ23,24.
Therefore, Staphylococcus aureus, Pseudomonas aeruginosa or bacterial LPS could induce eosinophilic inflammation and the synthesis of polyclonal IgE, elevating total IgE levels led by increased IL-4 levels and reduced levels of INF-γ23,24. Enteroxin would thus modify nasal polyposis through the IgE released by mastocytes and would act as an alternative mechanism to allergy24.
CONCLUSION
The expression of mRNA for interleukins 5, 6, 8, and GM-CSF analyzed through RT-PCR was similar among the control and cystic fibrosis groups. Low INF-γ levels and tendency to increased IL-4 levels were found in the group with cystic fibrosis.
REFERENCES
1. Pawanka R. Nasal polyposis: na update. Curr Opin Allergy Clin Immunol. 2003;3(1):1-6.
2. Rinia AB, Kostamo K, Ebbens FA, Van Drunen CM, Fokkens WJ. Nasal polyposis: a cellular-based approach to answering questions. Allergy. 2007;62:348-58.
3. Beju D, Meek WD, Kramer JC. The ultrastructure of the nasal polyps in patients with and without cystic fibrosis. J Submicrosc Cytol Pathol. 2004;36(2):155-65.
4. Claeys S, Van Hoecke H, Holtappels G, Gevaert P, De Belder T, Verhasselt B, et al. Nasal polyps in patients with and without cystic fibrosis: a differentiation by innate markers and inflammatory mediators. Clin Exp Allergy. 2005;35:467-72.
5. Settipane GA. Epidemiology of nasal polyps. Allergy and Asthma Proc. 1996;17(5):231-6.
6. Bernstein JM, Gorfien J, Noble B, Yankaskas J. Nasal polyposis: immunohistochemistry and bioeletrical findings (a hypothesis for the development of nasal polyps). J Allergy Clin Immunol. 1997;99(2):165-75.
7. Douglass JA, O'Hehir RE. Diagnosis, treatment and prevention of allergic disease: the basics. Med J Aust. 2006;185(4):228-33.
8. Bryan D, Walker KB, Ferguson M, Thorpe R. Cytokine gene expression in a murine wound healing model. Cytokine. 2005;31(6):429-38.
9. Miller CH, Pudiak DR, Hatem F, Looney RJ. Accumulation of interferon gamma-producing TH1 helper T cells in nasal polyps. Otolaryngol Head Neck Surg. 1994;111(1):51-8.
10. Becker HMG, Guimarães RES, Nascimento E, Becker C, Gonçalves DU,Crossara PFTB. Perfil de citocinas e tipificação de HLA em pacientes com polipose nasossinual tolerantes e intolerantes a aspirina. Rev Bras Otorrinolaringol. 2003;69(3):296-02.
11. Bergoin C, Gosset P, Lamblin C, Bolard F, Turck D, Tonnel AB, et al. Cell and cytokine profile in nasal secretions in cystic fibrosis. J Cyst Fibros. 2002;1(3):110-5.
12. Sobol SE, Christodoulopoulos P, Manoukian JJ, Hauber HP, Frenkiel S, Desrosiers M, et al. Cytokine profile of chronic sinusitis in patients with cystic fibrosis. Arch Otolaryngol Head Neck Surg. 2002;128:1295-8.
13. Armstrong DS, Grimwood K, Carlin JB, Carzino R, Gutierrez JP, Hull J, et al. Lower airway inflammation in infants and young children with cystic fibrosis. Am J Respir Crit Care Med. 1997;156(4 Pt 1):1197-204.
14. Noah TL, Black HR, Cheng PW, Wood RE, Leigh MW. Nasal and bronchoalveolar lavage fluid cytokines in early cystic fibrosis. J Infect Dis. 1997;175(3):638-47.
15. Black RH, Yankaskas JR, Johnson LG, Noah TL.Interleukin-8 production by cystic fibrosis nasal epithelial cells after tumor necrosis factor - a and respiratory syncytial virus stimulation. Am J Respir Cell Mol Biol. 1998;19(2):210-5.
16. Mulloi J, Xaubet A, Gaya A, Roca-Ferrer J, Lopez E, Fernandez JC, et al. Cytokine gene expression and release from epithelial cells. A comparison study between healthy nasal mucosa and nasal polyps. Clin Exp Allergy. 1995;25(7):607-15.
17. Bernstein JM, Gorfien J, Noble B. Role of allergy in nasal polyposis: a review. Otolaryngol Head Neck Surg. 1995;113(6):724-32.
18. Castro MCM, Assunção E, Castro MM, Araújo RN, Guimarães RE, Nunes FB. Efeito da mitomicina C em polipose nasossinusal eosinofílica, in vivo: dosagem de IL5 e GM-CSF, RT-PCR. Brazilian Journal Otorhinolaryngol. 2006;72(1):38-42.
19. Kramer MF, Ostertag P, Pfrogner E, Rasp G. Nasal interleukin-5, immunoglobulin E, eosinophilic cationic protein, and soluble intercellular adhesion molecule-1 in chronic sinusitis, allergic rhinitis, and nasal polyposis. Laryngoscope. 2000;110:1056-62.
20. Jankowski R, Bouchoua F, Coffinet L,Vignaud JM. Clinical factors influencing the eosinophil infiltration of nasal polyps. Rhinology. 2002;40:173-8.
21. Dellacono FR, Roselle E, Denis L, Leonard G, Kreutzer D. Interferon gamma expression in human nasal polyps. Laryngoscope. 1997;107(5):626-30.
22. Voegels RL, Santoro P, Butugan O, Formigoni LG. Nasal polyposis and allergy: is there a correlation? Am J Rhinol. 2001;5(1):9-14.
23. European position paper on rhinosinusitis and nasal polyps. Rhinology Suppl. 2005;18:1-88.
24. Moqbel R. Eosinophils, cytokines, and allergic inflammation. Ann N Y Acad Sci. 1994;725:223-33.
25. Boehm U, Klamp T, Groot M, Howard JC. Cellular responses to interferon-gamma. Annu Rev Immunol. 1997;15:749-95.
26. Galietta LJ, Folli C, Marchetti C, Romano L, Carpani D, Conese M, et al. Modification of transepithelial ion transport in human cultured bronchial epithelial cells by interferon-gamma. Am J Physiol Lung Cell Mol Physiol. 2000;278(6):L1186-94.
1. PhD in Medicine, HFMG; Substitute Professor, Department of Ophthalmology and Otorhinolaryngology, UFMG.
2. MSc in General Surgery, UFMG Medical School; Advisor, Medical Residency Service, UFMG University Hospital and Santa Casa de Misericórdia Hospital - MG.
3. MSc in General Surgery, UFMG Medical School; MD, ENT, General Surgeon, Medical Officer at the Minas Gerais Military Police.
4. PhD in Parasitology, UFMG; Adjunct Professor, Department of Parasitology, Federal University of Minas Gerais.
5. PhD in Ophthalmology and Otorhinolaryngology, UFMG; Adjunct Professor, Department of Otorhinolaryngology and Ophthalmology, UFMG Medical School.
6. PhD in Ophthalmology and Otorhinolaryngology, UFMG; Adjunct Professor, Department of Otorhinolaryngology and Ophthalmology, UFMG Medical School.
7. PhD in Medicine; Professor, USP Medical School at Ribeirão Preto; Adjunct Professor, Department of Otorhinolaryngology and Ophthalmology, UFMG
Medical School.
Paper submitted to the BJORL-SGP (Publishing Management System - Brazilian Journal of Otorhinolaryngology) on February 26, 2009;
and accepted on May 26, 2009. cod. 6293
Print: ![]()