

Year: 2007 Vol. 73 Ed. 3 - (6º)
Artigo Original
Pages: 323 to 328
 PDF PT
PDF PT  PDF EN
PDF ENSecretory A immunoglobulin, total proteins and salivary flow in Recurrent Aphthous Ulceration
Author(s): Kennedy de Oliveira Martinez 1, Lauro Lúcio Mendes 2, José Bento Alves 3
Keywords: salivary immunoglobulin, saliva, recurrent aphthous ulceration.
Abstract:
Clinical and experimental study. Introduction. Of debatable etiology, Recurrent Aphthous Ulcerations (R.A.U), is most of the time considered an immunological deficiency. Aim: The aim of this paper is to review the literature and clinical investigations regarding IgA-s, total proteins salivary concentration and basal salivary flow of patients with R.A.U. during activity and quiescence. Methodology. Nephelometry was used to measure salivary IgA-s; Pyrogallol red was used for total salivary proteins and the gravimetrical analysis for salivary flow measurement. Results. Results demonstrated a significant increase in salivary IgA-s in active lesions in relation to quiescence. On the other hand, protein concentration rates were similar in both periods. Conclusion. Salivary IgA-s can be used as a parameter to study the immune status of the oral mucosa.
![]()
INTRODUCTION
Hipocrates (460-370 a.C.) was the one who, for the first time, employed the word "aphtha" (aphtodea)1, coming from the Greek word a p t e i n (ARTEIV), translated as "set fire"2. Until today, the etiology of recurrent aphthous ulcerations (RAU) remains unknown, although hints of its etiologic basis lay on genetic susceptibility, infectious agents and alterations in immune mechanics.
Now, the mouth mucosal protection system is well known, and gathers a large number of substances responsible for its homeostasis3.
The most important humoral mediator for mucosal immunity is secretory IgA4,5, for cooperating with a number of protection mechanisms6, for presenting greater resistance to the proteolytic degradation caused by other immuneglobulins7 and for being especially located in the digestive and respiratory tracts, which are in close contact with the environment8, preventing the uptake of a large amount of antigens and precluding an overload in the immune system9.
The secretory A immunoglobulins present in saliva are excellent indicators of the oral mucosa immune status10-12, nonetheless, clinical-laboratorial comparisons of recurrent aphthous ulcerations and the local protecting mechanisms involved indicate the need for further studies, having in mind the scarce number of papers published and contradictory results.
MATERIALS AND METHODS
The present investigation, approved by the Research Ethics Committee of the Federal University of Vales do Jequitinhonha e Mucuri Dentistry School, counted on the participation of twenty patients with prior history of recurrent aphthous ulcerations, seen in the department of Stomatology of the aforementioned institution. The patients were selected regardless of gender, age, race or socio-economical situation, who matched the inclusion criteria, such as no chronic systemic diseases, drug therapy in the week prior to the exam and recent dental treatment. All patients were informed on the procedures before entering the research project, and signed an informed consent form.
In order to obtain a sample of total saliva, the patients were instructed as not to eat or drink (except water) for one hour and mouth hygiene at least two hours before the procedure. Mouth washing with pure water was carried out right before harvesting the samples (between 8 and 10 am). Sampling time was never above 15 minutes.
Total spontaneous saliva that collected on the oral cavity floor was harvested with disposable sterilized Pasteur-type pipettes. After harvesting, 1.5ml of each sample was placed in coded Eppendorf tubes and centrifuged afterwards, in order to reduce bubble and foam, and stored in a refrigerated system (freezer at -20ºC). All patients participated in two times during the research. The first was when they had active aphthous lesion, and the second was when they did not have the lesion (quiescent period).
Biochemical Analysis
Nefphelometry was used in order to quantitatively assess salivary IgAs (Behring Nephelometer II, Behring, USA) with calibrators and reagents supplied by the manufacturer. In order to assess total proteins, we used the Pyrogallol red (Sensiprotò) and reading carried out by a semi-automatic analyzer (550 Express from CIBA - Corningò).
After harvesting, we carried out spontaneous salivary flow measures (flow at rest) at the times of active lesion and at quiescence. During this evaluation, all patients remained seated and relaxed, with their heads down and lips slightly open in such a way as to let saliva drool passively over the lower lip and be collected in a graduated beaker of known weight. 5 minutes was taken for each sampling. Salivary flow was determined by gravimetric analysis13,14.
Statistical Analysis
Comparisons were made between male and female patients for each one of the time points (with and without aphtha) in relation to the variables' measures: salivary flow, salivary IgA-s and total salivary proteins concentration, using the Kruskal-Wallis test. This test compares two or more independent samples in relation to a variable of interest.
Aiming at comparing samples (at the time points with and without aphthae) by gender, in relation to the variables' measures: salivary flow rate, IgA-s and total salivary proteins concentration (regardless of gender in relation to salivary flow and salivary IgA-s), we used the Wilcoxon non-parametric test of paired samples.
All results were considered significant for a significance likelihood below 5% (p<0.05) thus, yielding at least 95% of confidence in the conclusions presented.
RESULTS
Of the selected patients, 12 (60%) were females and 8 (40%) were males, within an age range between 07 and 54 years, with a prevalence in the 3rd decade of life (from 21 to 30 years). As related to age, there were no significant differences (p> 0.05) gender wise; in other words, the ages of these two groups of patients were similar.
The lesions varied between 1 and 4mm in diameter and prevailed on the tongue, gingival-labial notch and upper lip, with an average number of 2 (two) lesions per patient.
Predisposing factors reported were: stress, food, gastrointestinal disorders, menstrual cycle, family history and in some it was not possible to notice any association with predisposing factors (no apparent cause).
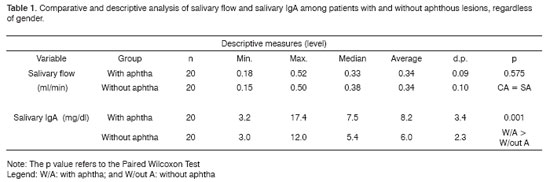
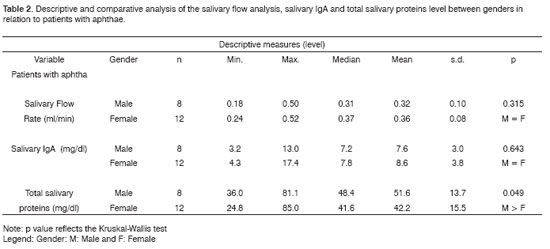
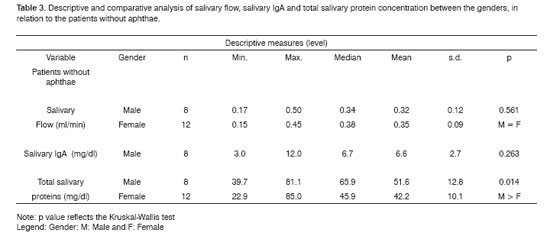
Results regarding patients' salivary flow and IgA-s level evaluations at the time points with and without aphtha, regardless of gender, are presented on (Table 1). Notice that there were no statistically significant difference between salivary flow mean values of the patients at the two time points - active lesion and quiescence. As to total protein values at the two time points, gender-related, we noticed that for males the values were statistically higher (Table 2). On the other hand, the total proteins concentration was different considering the two time points (activity and quiescence) in recurrent aphthous ulcerations (Table 3). The levels of salivary IgA-s in the results proved to be significantly increased at the time of activities of this lesion, when compared to results at quiescent periods (Table 3).
DISCUSSION
The word "aphtha" has been used both by health care professionals as by laymen in order to call any oral lesion characterized by pain similar to those caused by a burn2.
In this investigation, the term recurrent aphthous ulcerations (RAU) was employed in order to avoid confusions with other similar entities.
The diagnosis of RAU is purely clinical, considering its semiologic and evolution characteristics15. The histopathology of these ulcerations does not show specificity, it was used mainly to rule out the non-aphthous lesions7, since it represents the histopathology of a non-specific inflammatory process16.
Recurrent aphthous ulcerations are usually classified as: major, minor and herpetiform, according to their clinical manifestations such as number of lesions, location and severity17. In our series, the most prevalent type was the minor, with onset average time of 5 days.
Spontaneous saliva was preferred over the stimulated flow, since there are already data in the literature about the "flow at rest", and because it is more reliable to represent the physiology of oral secretions without the interference of external factors.
Despite the small amount, organic substances are molecules responsible for a major part of the saliva's biologic functions18; they are part of the immune system and may, to some extent, operate independently of the general immune system4.
Secretory immunoglobulin A (IgA -s) is an important parameter to assess the autoimmune status of the mucosa, with the advantage of being measurable by non-invasive methods and without patient discomfort19,20. This is the major class of immunoglobulin found in mucous secretions, and is responsible for a barrier against a number of infectious, environmental allergens and carcinogenic substances19, and it also aids in many inborn protection mechanisms8.
IgA represents the second most abundant immunoglobulin in the human serum and prevails in the saliva in its dimeric form (IgA-s) which better resists proteolysis in environments such as the mouth21.
IgA deficiency is the most common immune humoral defect in humans, and for the most part, causes gastrointestinal and respiratory infections22,23.
If immunity has some regulating effect on the development of recurrent ulcers, what is expected is that IgA-s be the immunoglobulin that provides protection, considering its role in other body parts.
In this study, we aimed at investigating IgA-s concentrations and that of total proteins found in the total spontaneous saliva and check to see if they differ during the times of quiescence and exacerbation of recurrent aphthae.
As a means to check salivary flow variations, which could influence IgA-s and total protein levels, we used total saliva at rest flow check. Our results showed that there were no statistically significant differences between flow measures at the times of active lesion and acquiescence (table 1). Similar results were obtained from patients with RAU when compared to individuals without prior history of such lesions24.
We also did not see statistically significant differences between total protein concentrations in patients with and without aphthae.
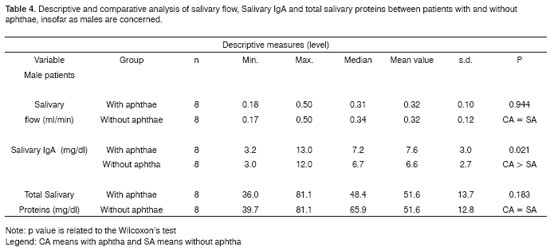
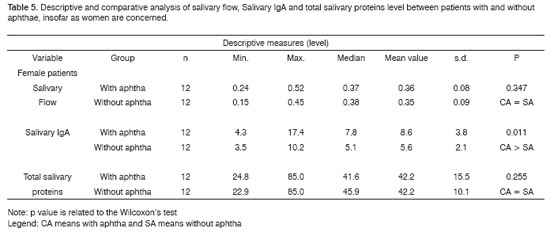
Now, total protein concentrations did not vary when the patients were compared with and without lesions (Table 3). Spontaneous and stimulated total saliva flow sample analyses showed that salivary flow was lower and total protein concentrations were higher in women when compared to men13. in the present investigation, when we compared total proteins we found higher concentrations (p < 0.05) at the two time points (With and Without aphthae) in men. On the other hand, salivary flow mean values did not present significant difference between genders (according to Table 2). It is interesting to notice that, although men presented higher concentrations of total proteins when compared to women, we noticed that both for men and women, total protein concentrations were similar for both time points: with and without aphthae. There were no statistically significant differences (p>0.05) between these two time endpoints (Tables 4 and 5).
As to the salivary IgA-s values, there was a statistically significant difference (p<0.05) in the values, noticeably higher during lesion exacerbation when compared to inter-crisis periods (without lesions), as described on Table 1. Moreover, Table 3 corroborates these results, that is, both for males and females; the salivary flow variable in patients with and without aphthae does not differ statistically, while salivary IgA-s levels were statistically higher in patients with aphthae. These data are similar to those found in individuals with aphtha and those without prior history of this lesion25,26.
A study carried out on salivary IgA-s levels in patients with RAU at the times of incipient and acute lesion, regression and complete cure, showed an increase in IgA-s at the acute period, and its reduction in periods of regression and cure, and for the women in the group, very discrepant results were noticed, in some of them salivary IgA-s levels were influenced by menstrual cycle and in others there were no such association27. This leads to this unreliable correlation between IgA-s salivary levels and the menstrual period, even in those with association between the menstrual cycle and recurrent aphthous ulcerations28. Our series had only one woman (of the 12 females in the group) who reported having aphthous ulcerations at the time of menstruation.
CONCLUSION
Our results suggest a strong correlation between IgA-s and the lesion mechanisms in recurrent aphthous ulcerations, and this may be used as a parameter to assess the mucosal immune status.
REFERENCES
1. Tommasi AF. Ulceração aftosa recorrente, um estudo sobre hereditariedade realizado com 151 famílias. Ass Curandi em Odontologia 1975;2(2):32-4.
2. Pedersen A, Madsen HO, Vestergaard B, Ryder LP. Varicella - zoster virus DNA in recurrent aphthous ulcers. Scand J Dent Res 1993;101(1):311-3.
3. Nidr - Nacional Institute of Dental Research. Saliva: A promising diagnostic and monitoring toal. JADA - J Am Dent Assoc 1974;125(1):867-8.
4. Vetvik H, Grewal HMS, Haugen IL, Ahren C, Haneberg B. Mucosal antibodies can be measured in air-dried samples of saliva and feces. J Immunol Methods 1998;215(1):163-72.
5. Segal AL, Katcher AH, Brightman VJ, Miller MF. Recurrent herps labialis, recurrent aphthous ulcers and the menstrual cycle. J Dent Res 1979;53(4):797-803.
6. Brandtzaeg P. Molecular and cellular aspects of the secretory immunoglobulin system. APMIS - Acta Pathol Microbiol Immunol Scand 1995;103(1):1-19.
7. Stanley HR. Aphthous Lesions. Oral Surg Oral Med Oral Pathol 1972;33(3):407-16.
8. Lamm ME, Nedrud JG, Kaetzel CS, Mazanec MB. IgA and mucosal defense. APMIS - Acta Pathol Microbiol Immunol Scand 1995;103(4):241-6.
9. Slavkin HC. Protecting the mouth against microbial infections. J Am Dent Assoc 1998;129(7):1025-30.
10. Smith OJ, King JV, Gilbert JV, Taubman MA. Structural integrity of infant salivary immunoglobulin A (IgA) in IgA 1 protease - rich environments. Oral Microbiol Immunol 1998;13(5):278-85.
11. Hucklebridge F, Clow A, Evans P. the relationship between salivary secretory immunoglobulin A and cortisol: neuroendocrine response to awakening and the diurnal cycle. Int J Psychoplysiol 1998;31(1):69-76.
12. Externest D, Meckelein B, Schmidt MA, Frey A. Correlations between antibody immune responses at different mucosal effector sits are controlled by antigen tipe and dosage. Elsevier Science 2000;68(7):3830-9.
13. Banderas - Tarabay J A, Begner MG, Garnuño AS, Cortez EM. Flujo y concentración de proteínas en saliva total humana. Salud Publica Mex 1997;39(5):1-17.
14. Bretz WA, Valle EV, Jacobson JJ, Marchi F, Mendes S, Nor JE, Cançado MF. Unstimulated salivary flow rates of Young children. Oral Surg Oral Med Oral Pathol 2001;21(5):541-5.
15. Békourian F. I'utilisation du zinc dans I'aphtose buccale. ActualOdontostomatol (Paris) 1995;189(1):73-85.
16. Cawson RA. Oral ulceration - clinical aspects. Oral Surg Oral Med Oral Pathol 1972;33(6):912-21.
17. Cawson RA, Odelle EW. Diseases of the Oral mucosa: Non-infective estomatites. In: Essentials of Oral Pathology and Oral Medicine. 6th ed. Toronto: Churchill Livingstone; 1998. p. 183-7.
18. Sreebny LM, Banoczy J, Baum BJ, Edgar WM. Saliva: its role in health and disease. Int Dent J 1992;42(4):291-331.
19. Kilian M, Reinholdt J, Lomholt T, Poulsen K, Frandsen EV. Biological significance of IgA1 proteases in bacterial colonization and pathogenesis: critical evaluation of experimental evidence. APMIS - Acta Pathol Microbiol Immunol Scand 1996;104(5):321-38.
20. Hucklebridge F, Lambert S, Clow A, Warburton DM, Evans PD, Sherwood N. Modulation of secretory immunoglobulin A in saliva; response to manipulation of mood. Biol Psychol 2000;53(1):25-35.
21. Miletic ID, Schiffman SS, Miletic VD, Miller EAS. Salivary IgA secretion rate in Young and elderly persons. Physiol Behav 1996;60(1):243-8.
22. Truedsson L, Baskin B, Pan Q, Rabbani H, Vorechovsky I, Smith CI. Genetics of IgA deficiency. Acta Pathol Microbiol Immunol Scand 1995;103(12):833-72.
23. Voltz JM, Mole C, Aubin F, Gibey R, Faivre B, Seilles E, Humbert P. Immunoglobulines a serigues et salivaires dans la Lermatite Atopique: etudi prospective et comparative temoins - Malades. Ann Dermatol Venereol 1998;125(2):100-4
24. Ben-Aryed H, Malberger E, Gutman D, Szargel R, Anavi Y. Salivary IgA and serum IgG and IgA in recurrent aphthous stomatitis. Oral Surg Oral Med Oral Pathol 1976;42(6):746-52.
25. Sistig S, Vucicevic-Boras V, Lukac J, Kusic Z. Salivary IgA and IgG subclasses in oral mucosal diseases. Oral Disease 2002;8 (6):282-6.
26. Brozovic S, Vucicevic, Boras V, Bukovic D. Serum IgA, IgG, IgM and salivary IgA in recurrent aphthous ulceration. Coll Anthropology 2001;25(2):633-7.
27. Kakizawa T, Nona H, Omori K. The Evaluation of secretory IgA in human saliva. Bull Tokyo Dent Coll 1973;14(3):125-39.
28. Seidel BM, Schulze B, Kiess W, Vogtmann C, Borte M. Determination of secretory IgA and albumin in saliva of newborn infants. Biol Neonate 2000;78(3):186-90.
1 M.S. Professor of Morphologic Sciences - University of Uberaba.
2 PhD. Professor. Department of Restorative Dentistry - Dentistry School - UFMG.
3 PhD. Research, Postgraduate Programs and Extension Programs Dean - University of Uberaba.
Universidade de Uberaba, Uberaba MG.
Mailing Address: Dr. José Bento Alves - Av. Nenê Sabino 1801 Bairro Universitário Uberaba MG 38055-500.
Paper submitted to the ABORL-CCF SGP (Management Publications System) on May 5th, 2006 and accepted for publication on August 2nd, 2006. cod. 1900.
Print: ![]()