

Year: 2005 Vol. 71 Ed. 5 - (5º)
Artigo Original
Pages: 576 to 581
 PDF PT
PDF PT  PDF EN
PDF ENVestibular folds configuration in vocal nodule
Author(s): Juliane Tuma1, Osíris Oliveira Camponês do Brasil2, Paulo Augusto de Lima Pontes3, Reinaldo Kasuo Yasaki4
Keywords: vocal nodule, vestibular folds, laryx, voice.
Abstract:
Vocal nodules are among the most common laryngopathies that cause vocal functional disorders. The voice production mechanism is complex and demand interations of diverse systems of the human body. The physiological role of the vocal folds as the glottic sound source is evident, however, there is no consensus regarding the vestibular folds´ participation/influence in phonation. Aim: To verify if there is difference in the bidimensional configuration of the vestibular folds among two distinct groups of women, one with the diagnosis of vocal nodules and other without both vocal alterations and vocal fold lesions. Study design: clinical with transversal cohort. Material and Method: Ninety six laryngeal images were evaluated, 48 from individuals without vocal complaints and 48 from patients with the diagnosis of vocal nodules. Angles were obtained and bilaterally measured in single frames of the vestibular folds during sustained phonation and those structures were morphologically classified as concave, linear or convex. Results: Among the 96 vestibular folds evaluated in each group, there was predominance of the concave form, followed by the linear and the convex ones. In the control group, there was a single convex vestibular fold, 27 were linear and 68 were concave folds. In the group of vocal nodules, 8 were convex, 15 were linear and 73 were concave folds. However, the differences among groups were not statistically significant as well as those among the angles, whose average measures were proven quite similar. Conclusion: In the female gender, the vestibular folds presented similar behaviour regarding the morphology in both patients with vocal nodules and women without vocal complaints.
![]()
INTRODUCTION
The human larynx is a cartilaginous muscle organ with specific functions. Anatomically, laryngeal cartilages are joined by joints and ligaments, providing anterior-posterior, lateral and inclining movement. The intrinsic membrane makes movements of precision, with tensional and postural adjustment of the vocal folds. Such muscles provide abduction, adduction and tension movements. Phylogenetically, the main function of the larynx is to take air for breathing, followed by lower airway protection during swallowing, elimination of secretions and foreign bodies and support in effort mechanisms, such as defecation and delivery 1. Another laryngeal function that is essential for humans is sound production through phonation, that is, voice production. Human voice results from the interaction of factors such as genetic, anatomical, personal characteristics, such as the personality, as well as social, economic and cultural factors, plus unique emotional aspects that are exclusive to each subject. However, phonation is an adapted function to the larynx. Consequently, the concept of normal voice is undefined and depends on a number of variables, and the term "adapted voice" should be preferably used.2
The mechanism of vocal production is complex and requires interaction of different body systems, from respiratory tract to central nervous system. The understanding of the vocal fold vibration mechanism requires specific anatomical knowledge. Vocal folds are multi-laminated structures with different mechanical properties in each layer, comprising muscle or mucosa. The vocal muscle corresponds to the body of the vocal fold and the mucosa may be divided into epithelium (stratified squamous) and lamina propria (subdivided into superficial intermediate and deep layers)3. The vocal fold vibration mechanism is originated from combined undulations from the horizontal, vertical and longitudinal directions, from aerodynamic and myoelastic forces (aerodynamic-myoelastic phonation theory), determining the glottic cycle with its opened and closed phases. In controlling frequency, there is variation in length of vocal folds and in variation of intensity, which is due to increase in subglottic pressure. In controlling vocal quality, there is modification of the whole vocal tract, with the involved resonance aspects. Thanks to the introduction of optical fibers in ENT clinical practice, this function became more easily assessable.
The vocal nodule is among the most common laryngeal affections and results in vocal function affections.4,5 The definition of vocal nodule is even more contradictory, which may be considered benign thickness of the mucosa of the vocal fold free margin normally located in the junction of the anterior third with the medium third, uni or bilaterally, whose main etiology is vocal abuse. However, we consider the definition of this entity as being: bilateral damage, symmetrical in location, but it may be asymmetrical in size, with presence of medium posterior triangular chink, directly related with poor use or excessive vocal use, and larynx of infantile or female pattern.6 In the female or infantile larynx, glottic proportion (GP), which is the index that expresses the correlation between the intercartilaginous and intermembranous parts of the glottis ranging at about 1.0 or below in women and in men, has the value of about 1.3. It explains the trend to formation of nodules in female and pediatric populations and the formation of granulomas in male population 7,8. In stroboscopic findings, normally we evidence incomplete glottic coaptation and histopathological and immunohistochemical findings of thickness of basal membrane, but without presenting vascular affections of vocal fold mucosa 9-12. Thus, the importance of vocal folds is evident for the formation of glottic sound source; however, as to participation in vestibular folds, there is still no consensus among authors. Vestibular folds are formed by muscle, connective and fatty tissues and glands. The latter perform a lubrication function of the laryngeal epithelium, but it is more numerous on the subepithelial layer. Anatomical studies of excised larynges in post-mortem dissection evidence the presence of three distinct muscle groups: posterior-lateral layer, with fibers towards the sagittal direction; anterior-lateral layer, annex to the thyroid cartilage, and the anterior-medial layer, formed by a group of spread fibers, located medially and dorsally to the laryngeal ventricle.13 During phonation, arytenoid cartilages are strongly pulled by the vestibular folds and at the same time, aryepiglottic folds are superiorly displaced, increasing the glottic space beyond the width of the laryngeal ventricle, resulting in higher amplitude of vocal fold vibration.14
The position of the vestibular folds close to the vocal folds means that shape and size could influence the airflow through the larynx, which would modify the vocal fold vibration and affect vocal acoustics. Through linear measurements used to define the size and shape of vestibular folds, it has been detected that they are farther from the vocal folds in male patients than in female patients. The angular measurements show no statistically significant difference between genders 15. Supraglottic activity refers to the positioning and location of structures that are immediately above the vocal folds. During the vocal production mechanism, this activity may be divided into two types: anterior-posterior and lateral-medial. The visibility of vocal folds is partially or completely affected by the presence of supraglottic activity: anterior-posterior compression is a result of the approximation of arytenoid cartilages to the petiole of the epiglottis and lateral-medial compression happens when there is adduction of vestibular folds. However, static activity or even the dynamics of the supraglottis is considered normal for the articulation function at the laryngeal level, making part of the linguistic/phonetic system without evidencing any laryngeal dysfunction. Both the anterior-posterior compression and the vestibular fold compression may be present in normal subjects with diagnosis of vocal nodule, in similar mean percentage. Thus, the clinical hypothesis that supraglottic hyperactivity is associated with increase in laryngeal tension, which consequently could contribute to the development of vocal nodules, cannot be confirmed. This activity would be a normal component of the laryngeal behavior. Thus, practical applicability of the results of values of relative measurements of anterior-posterior and median compression may be questioned.16-18
Vestibular folds have been recently classified according to their shape: concave, convex or linear, depending on the shape in studied subjects, presenting significant differences between the analyzed groups (normal voice and dysphonia), and such difference has also been observed when we compare male and female patients.19
OBJECTIVE
The purpose of the present study was to check whether there was difference in vestibular fold shape during phonation in groups of female subjects who had vocal nodules or no vocal complaint and vocal fold damage.
MATERIAL AND METHOD
The material analyzed by the present study came from recordings of laryngeal images obtained through videolaryngostroboscopy performed at Instituto da Laringe (Inlar), between March 2003 and January 2005. We analyzed 96 images of larynges of female subjects aged 15 to 70 years. We selected 48 images of subjects without vocal complaints and no vocal fold lesions and 48 of subjects with diagnosis of vocal nodule. Given that they were file images, no procedure was applied to the subjects of the present study.
In the routine of clinical service, videolaryngostroboscopy is performed under topical anesthesia with lidocaine 10% spray with the patient seating down and with open mouth, protracted tongue involved with gauze and maintained by digital pull. Each patient is instructed to breathe through the mouth, without effort and produce the sustained vowel /?/ at habitual intensity. In the studied cases, the telescope that had been used was Machida® 70o and conventional video system with microcamera Panasonic® KS 152. A computer AMD ATLON® XP 1600 1.6, with Windows® 2000 operational system was used to transfer the images. After digitalization of images, performed with the software ADOBE PREMIERE® with video board PINACLE® DC 1000, we choose only one frame of phonation. The beginning and the end of the production were discarded. The exclusion criteria were:
* Presence of anterior-posterior constriction, which prevented the location of the vestibular folds insertion;
* Performance of the test while the patients had nausea reflex;
* Permanence of secretion in the glottic region, preventing the definition of anatomical limits that are indispensable for the precise localization of the structures;
* Quality of appropriate image for definition of points.
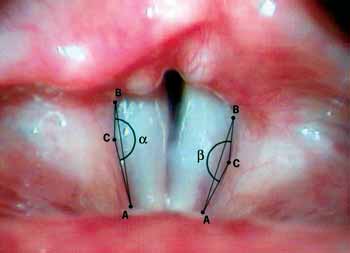
Images were analyzed in the computer and reference lines and points were defined:
ANTERIOR POINT (A): correspondents to anterior extremity of the vestibular fold free border in the anterior region;
POSTERIOR POINT (B): site where the vestibular fold free border ends in the posterior region;
AB LINE: junction of points A and B;
DISPLACEMENT POINT (C): point corresponding to largest vestibular fold free margin displacement in relation to line AB.
LINES AC AND BC: formed by the junction of points A and B with C;
When the free margin of the vestibular fold coincides in all it extension or is very close to line AB, point C is considered as belonging to line AB;
a = angle formed by the intersection of lines AC and BC on the right vestibular fold;
b = angle formed by the intersection of lines AC and BC on the left vestibular fold (Figure 1).
We made the angle measurements in levels, considering the angle directed to laryngeal lumen. For this measurement we used the tool "angle", from the program IMAGE TOOL 3.0. Two types of parameters were used:
a) Quantitative: numeric value of angles;
b) Qualitative: classification of vestibular folds as to shape:
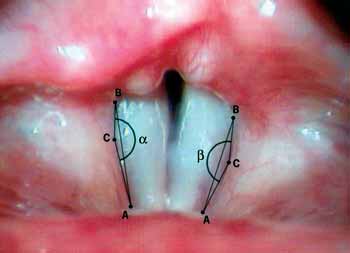
* Concave: point C lateral to AB;
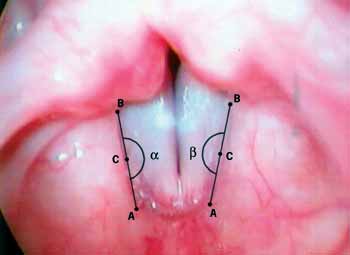
* Linear: point C coinciding or very close to AB;
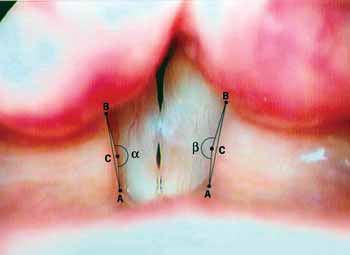
* Convex: point C medial to AB.
For the statistical analysis, we used:
T Student test for paired data, controlled by Levene test for equal variance and chi square test transformed by Fischer statistics.
RESULTS
The results are presented in Tables.
Figure 1. Reference points A, B and C, lines AB, AC and BC and angles ? and ?.
Figure 2. Vestibular folds of concave shape with reference points and lines for definition of alpha and beta angles.
Figure 3. Vestibular folds of linear shape with reference points and lines for definition of alpha and beta angles.
Figure 4. Vestibular folds of convex shape with reference points and lines for definition of alpha and beta angles.
DISCUSSION
Vocal nodule intrinsically means that there is effort at phonation20-23 . The reason for this study was to check whether the vestibular folds could indicate the presence of this effort at the supraglottic region by modifying the shape.
The statistical analysis of our results indicated that there is no statistically significant difference in configuration between the group of women without vocal complaint and the group of people with vocal nodules.
In view of this finding, we have to consider two hypotheses: the first one, that the effort involves the supraglottis without modifying the vestibular folds, and the second one, that the effort does not involve the supraglottis. Nemetz et al., using a qualitative analysis, comparatively studied subjects without vocal complaint and groups with different laryngeal affections in which some involved phonation efforts, such as unilateral vocal fold paralysis, and they found statistically significant differences in vestibular fold shape. In view of this information, we could then suppose that in our group of vocal nodule, given that there was no participation of the vestibular folds, there was no effort at the supraglottic level. This finding is in agreement with what was observed by the group at the University of Washington in two different articles 16,17 which concluded the same as we did concerning lateral constriction using a different method with laryngeal measurements in pixels; conversely, these authors observed the existence of anterior-posterior supraglottic constriction, that is, approximation between the epiglottis cartilage and the arytenoids. In our study, this aspect was not considered, given that by our method, we would require the appropriate conditions to identify the anterior and posterior ends of the vestibular folds, which was not possible when the other type of supraglottic constriction happened. In view of this, to perform quantitative measurements, there is the need to develop another technique to measure the angle formed by the vestibular fold displacement 19 without requiring the identification of the extreme points. We reinforce that we used the angle formed by the vestibular fold free margin to perform the comparative study, given that the measurement of the angle is independent from the distance in relation to the telescope, which does not happen with linear measurements in pixels. The comparative study with linear measurements was hindered because the different inter-subject laryngeal heights relative to laryngoscope resulted in different values for the same dimension. This technique of assessment of vestibular fold shape is not described in the consulted articles. Thus, the configuration of the vestibular folds did not indicate the presence of phonation effort involving these structures in the supraglottis, differently from the glottic region. In this region, the tension can be clinically evidenced by the action of the posterior cricoarytenoid muscle, which according to Pontes et al.6,8 would be responsible for the presence of posterior medium triangular chink that is used as criterion for the diagnosis of vocal nodules.
CONCLUSION
The results obtained showed that vestibular folds configuration does not affect the behavior of patients with vocal nodules or without vocal complaints.
REFERENCES
1. Imamura R, Tsuji DH, Sennes LU. Fisiologia da laringe. In: Campos CAH, Costa HO. Tratado de Otorrinolaringologia. São Paulo: Rocca; 2002. p. 743-50.
2. Behlau M, Azevedo R, Pontes PAL, Brasil, OOC. Disfonias funcionais. In: Behlau M. Voz: O livro do especialista. São Paulo: Revinter; 2001. p.248-70.
3. Gray SD. Basement membrane zone injury in vocal nodules. In: Gauffin, J, Hammarberg B. Vocal Fold Physiology. Stockholm, Sweden: Singular; 1991. p. 21-7.
4. Ford CN, Bless DM, Campos G, Leddy M. Anterior commissure microwebs associated with vocal nodules: detection, prevalence and significance. Laryngoscope 1994; 104: 1369-75.
5. Johns MM. Update on the etiology, diagnosis and treatment of vocal fold nodules, polyps and cysts. Curr Opin Otolaryngol Head and Neck Surg 2003; 11: 456-61.
6. Pontes PAL, Behlau M, Kyrillos L. Configuration et rapport glottique: un essai pour comprendre la fente glottique postérieure. Revue de Laryngologie 1994; 115: 261- 6.
7. Pontes PAL, De Biase N, Kyrillos L, Pontes AAL. Importance of glottic configuration in the development of posterior laryngeal granuloma. Ann Otol Rhinol Laryngol 2001; 110: 765-9.
8. Pontes PAL, Kyrillos L, Behlau M, De Biase N, Pontes AAL. Vocal nodules and laryngeal morphology. J Voice 2002; 16 (3): 408-14.
9. Colton RH, Woo P, Brewer DW, Griffin B, Casper J. Stroboscopic signs associated with benign lesions of the vocal folds. J Voice 1995; 9 (3): 312-25.
10. Dikkers FG, Nikkels PG. Benign lesions of the vocal folds: histopathology and phonotrauma. Ann Otol Rhinol Laryngol 1995; 104: 698-703.
11. Courey MS, Shohet JA, Scott MA, Ossof RH. Immunohistochemical characterization of benign laryngeal lesions. Ann Otol Rhinol Laryngol 1996; 105: 525-31.
12. Pontes PAL, De Biase N, Behlau M. Vascular characteristics of the vocal fold cover in control larynges and larynges with benign lesions. Phonoscope 1999; 2 (3): 129-35.
13. Reidenbach MM. The muscular tissue of the vestibular folds of the larynx. Eur Arch Otorhinolaryngol 1998; 225: 365-7.
14. Von Doersten PGET. Ventricular dysphonia: a profile of 40 cases. Laryngoscope 1992; 102: 1296-301.
15. Agarwal M, Scherer RC, Hollien H. The false vocal folds: shape and size in frontal view during phonation based on laminagraphic tracings. J Voice 2003; 17(2): 97-113.
16. Stager SV, Bielamovicz S, Gupta A, Marullo S, Regnell JR, Barkmeier MJ Supraglottic Activity: Evidence of vocal Hyperfunction or Laryngeal Articulation? J Speech Lang Hear Res 2000; 43: 229-38.
17. Stager SV, Bielamovicz S, Regnell JR, Gupta A, Barkmeier MJ. Quantification of static and dynamic supraglottic activity. J Speech Lang Hear Res 2001; 44 (6): 1245-56.
18. Behrman A, Dahl LD, Abramson AL, Schutte HK. Anterior-posterior and medial compression of the supraglottis: signs of nonorganic dysphonia or normal postures? J Voice 2003; 17 (3): 403-10.
19. Nemetz MA, Pontes PAL, Vieira VP, Yasaki RK. Configuração das pregas vestibulares à fonação em adultos com e sem disfonia. Rev Bras Otorrinolaringol 2005; 71(1): 6-12.
20. Koufman JA, Blalock PD. Classification and approach to patients with functional voice disorders. Ann Otol Rhinol Laryngol 1982; 91: 372-7.
21. Morrison MD, Rammage LA, Belisle GM, Pullan CB, Nichol H Muscular tension dysphonia. J Otolaryngol 1983; 12: 302-6.
22. Hilman RE, Holmberg EB, Perkell JS, Walsh M, Vaughan C. Phonatory function associated with hyperfunctionally related vocal fold lesions. J Voice 1990; 4: 52-63.
23. Jiang JJ, Diaz CE, Hanson DG. Finit element modeling of vocal fold vibration in normal phonation and hyperfunctional dysphonia: implications for the pathogenesis of vocal nodules. Ann Otol Rhinol Laryngol 1998; 107: 603-10.
Post-graduation under course, Program of Otorhinolaryngology and Head and Neck Surgery, Federal University of Sao Paulo - Escola Paulista de Medicina - UNIFESP - EPM. Otorhinolaryngologist.
Master and Ph.D. in Otorhinolaryngology and Head and Neck Surgery, Federal University of Sao Paulo - Escola Paulista de Medicina, Advisor Professor, Department of ORL-CCP, UNIFESP-EPM.
Professor, Full Professor, UNIFESP-EPM, Coordinator of the Post-graduation Program in Otorhinolaryngology and Head and Neck Surgery, UNIFESP-EPM.
Resident physician in Otorhinolaryngology, UNIFESP-EPM.
Federal University of Sao Paulo - Escola Paulista de Medicina (UNIFESP - EPM) INLAR (Instituto da Laringe).
Address correspondence to: Juliane Tuma Avenida - Av. 9 de Julho 915 Bela Vista São Paulo SP 01313-000.
The article was submitted by SGP on 13/May/2005 and approved on 28/Jun/2005.
Print: ![]()