

Year: 2004 Vol. 70 Ed. 6 - (22º)
Relato de Caso
Pages: 837 to 840
 PDF PT
PDF PT  PDF EN
PDF ENMultiple exophytic osteomas of craniofacial bones not associated with Gardner's Syndrome: a case report
Author(s): Ernesto Nascimento Filho , Maria T. Seixas , Alessandra Mazzoni , Luc L. M. Weckx
Keywords: Key words: exophytic osteomas, exostosis, Gardner's Syndrome.
Abstract:
Summary
Exophytic osteomas are mature bone protuberances requiring to be carefully differentiated from other lesions. The authors present a male, 44 year-old patient's report presenting multiple exophytic osteomas located in both sides of the vestibulomaxilar, premolar and molar regions non-associated with Gardner's Syndrome.
![]()
INTRODUCTION
Exostosis and tori are well known by anthropologists and the first article was published by Fox (1814)1. Exostosis, osteomas and tori are bone nodular protuberances whose precise designation depends on the anatomical location 2.
Exostoses are benign bone growth of facial skeleton that occur along the maxilla and mandible regions and are frequently located in the pre-molar and molar regions 3.
Torus palatinus and mandibularis are the two most common intra-oral growths; palatinus torus is a nodular bone mass that occurs along the midline of hard palate and mandibularis torus is a bone protuberance located on the lingual aspect of the mandible, normally in the region of canine and pre-molars 2. The histological characteristic of tori and other types of exostoses are identical, that is, described as hyperplastic bone, comprising mature trabecular and cortical bone 4.
Osteomas are bone lesions with different onset and slow growth that may be divided into: (1) cranial and mandibular exophytic osteomas (or eburnean exostoses); (2) paranasal sinuses, facial bones and orbit osteomas (orbital cavity osteoma); (3) exostoses or bone islands, (4) long bone superficial osteomas (justacortical) 5,6.
CASE REPORT
C. E. P. J., male 44-year-old patient, born and coming from Sao Paulo, was referred to the division of Stomathology, HSP, Escola Paulista de Medicina (UNIFESP), complaining of gum enlargement in both sides of lower pre-molar and molar regions.
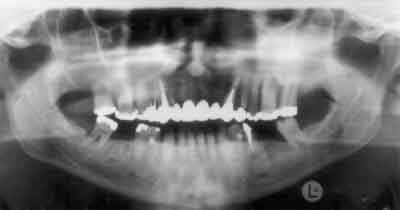
Clinical examination showed that it was a nervous patient that reported history of included permanent and supranumeric teeth. Even though the patient presented well-restored dentition, there was wear of occlusal aspect of pre-molars and molars, with excessive occlusal forces and thick masseter muscle on both sides. Bone multiple protuberances were evident in the vestibule-maxilla region on both sides (Figure 1). The approximate diameter of bone lesions ranged from 0.5 to 2.0cm; radiological study detected radiopaque images, hiding details of the teeth and maxillary sinus (Figure 2).
Oral findings were suggestive of the diagnosis of Gardner's syndrome. Owing to the likelihood of Gardner's syndrome be associated with intestinal tumors, we decided to investigate this condition and the patient was submitted to gastroenterological assessment. We also sent a blood sample to the discipline of clinical genetics for analysis. Gastrointestinal endoscopy and colonoscopy were within the normal range, with no polyps detected. Hetero-duplex analysis of cholopolyposis adenomatous gene (CPA) codified area, located in chromosome 5q21, did not identify any abnormality. Thus, suggestive management recommended surgical removal of bone anomalies and regularization of maxillary margins. Clinical pathology indicated the diagnosis of exophytic osteoma (Figures 3 and 4). The patient was referred to physical therapy for muscle hyperfunction. He was fitted with Michigan stabilizing splint to correct mastication parafunction.
DISCUSSION
The etiology of exostosis has been investigated by different authors, but no consensus has been reached so far. The most widely accepted hypotheses are: nutritional disorders, heredity, mastication hyperfunction, and environmental factors 2,4,7-9.
The highest prevalence was found in the adult age groups, aged 60 years or more (21.7%), when compared to the group aged 13 to 19 years (7.8%). The other age groups of 20 to 29 years, 30 to 39 years, 40 to 49 years and 50 to 59 years demonstrated similar frequency 8.
As to gender, there is higher prevalence in male subjects 8.
Exostoses are nodular protuberances of mature maxilla and mandible bones. If single and located in the palate or lingual aspect of the mandible they are called tori9.
Multiple exostoses classically occur as a series of discreet increase in bone volume along the vestibular view of maxillary and mandibular arches; it is clinically suggested that they occur less frequently than tori5.
Radiographically, they present in the maxilla as a well-delimited radiopaque mass, many times hiding details of the teeth and maxillary sinus9; in the mandible they simulate mandible lesions such as bone deformity, osteomyelitis and Gardner's syndrome; but anamnesis and appropriate laboratory tests can easily provide the definite diagnosis 10.
Vestibule-alveolar bone thickness found is on average 1mm for frontal and pre-molar teeth, 2mm for upper molars, and 2-3mm for lower molars 11.
The mucosa that recovers the bone protuberance is normally superficial and has normal appearance, but if exposed to trauma, it may become whitish and ulcerated 12.
The term exostosis is used to designate lesions that grow exophytically on the bone surface, referring, thus, to a growth pattern.
Osteomas present well-defined clinical, radiological and histological characteristics 10. Thus, it is important to have precise diagnosis, differentiating exophytic osteomas, osteochondromas, organized subperiosteal hematoma, mature ossifying fibroma that causes expansion of cortical lamina and periosteal osteosarcoma or chondrosarcoma 5.
Gardner's syndrome is a hereditary dominant autosomal disorder with estimated prevalence of 1 in 14,00013. It consists of multiple polyposis of large intestine, bone osteomas, including long bones, head and mandible, multiple epidermal or cutaneous sebaceous cysts, particularly on the scalp and dorsal region, with occasional frequency of dermoid tumors and included permanent and supranumeric teeth14.
Most patients with Gardner's syndrome do not show complete clinical picture of the disease: the term binary for Gardner's syndrome has been applied to subjects that have 2 or 3 of the aspects traditionally described 13,15.
Bone lesions in Gardner's syndrome are not real neoplasms. Moreover, the presence of osteoblastoma analog areas, predominantly seen in sino-orbital sporadic osteoma, is not an aspect of bone lesions in Gardner's syndrome6.
Colon and rectum digestive endoscopy for detection of intestinal polyps and genetic analysis were subsequently used to exclude Gardner's syndrome in this patient. Even so, this case showed the important role researchers have to use oral care in excluding systemic diseases with oral manifestations.
To conclude, the term exophytic osteoma would be better employed than exostosis, commonly used in the literature, given that it indicates only growth pattern of bone surface and not the histopathological aspects.
REFERENCES
1. Fox J. The natural history and diseases of the teeth. London; 1814.
2. Jainkittivong A, Langlais RP. Buccal and palatal exostoses: prevalence and concurrence with tori. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 90 (1): 48-53.
3. Czuszak CA, Tolson GE 4th; Kudryk VL, Hanson BS, Billman MA. Development of an exostosis following a free gingival graft: case report. J Periodontol 1996; 67 (3): 250-3.
4. Regezi JA, Sciubba JJ. Oral pathology: clinico-pathologic correlations. Philadelphia: WB Saunders Co 1989; p.386-7.
5. Chaudry SI, Tappuni AR, Challacombe SJ. Multiple maxillary and mandibular exostoses associated with multiple dermatofibromas: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 89 (3): 319-22.
6. Dorfman HD, Czerniak B. Bone tumors 1997; p. 1087-8.
7. Matthews GP. Mandibular and palatine tori their etiology. J Dent Res 1933; 13:245.
8. Pynn BR, Kurys-Kos NS, Walker DA, Mayhall JT. Tori mandibularis: a case report and review of literature. J Can Dent Assoc 1995; 61 (12): 1057-9.
9. Seah YH. Torus palatinus and torus mandibularis: a review of the literature. Aust Dent J 1995; 40 (5): 318-21.
10. Siegel WM, Pappas JR. Development of exostoses following skin graft vestibuloplasty: report of a case. J Oral Maxillofac Surg 1986; 44 (6): 483-4.
11. Horning GM, Cohen ME, Neils TA. Buccal alveolar exostoses: prevalence characteristics and evidence for buttressing bone formation. J Periodontol 2000; 71 (6): 1032-42.
12. Pack AR, Gaudie WM, Jennings AM. Bony exostosis as a sequela to free gingival grafting: two case reports. J Periodontol 1991; 62 (4): 269-71.
13. Halling F, Merten HA, Lepsien G, Honig JF. Clinical and radiological findings in Gardner's syndrome: a case report and follow-up study. Dentomaxillofac Radiol 1992; 21:93-8.
14. Shafer WG, Hine MH, Levy BM. Tratado de patologia bucal. 4ª Ed. Editora Guanabara Koogan; 1987. p. 154-6.
15. Pierce ER, Weisbold T, Mckusick VA. Gardner's syndrome; formal genetics and statistical analysis of a large Canadian kindred. Clin Genet 1970; 1: 65-80.
Figure 1. Multiple maxillary bone protuberances.
Figure 2. Panoramic x-ray showing radiopaque images hiding details of teeth and maxillary sinus.
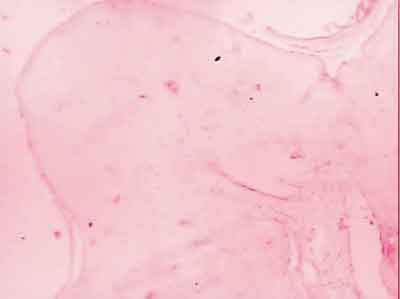
Figure 3. HE 40x photomicrography. Exophytic osteoma. In smaller magnification, we can see the presence of exophytic lesion, forming a bone tissue bulging.
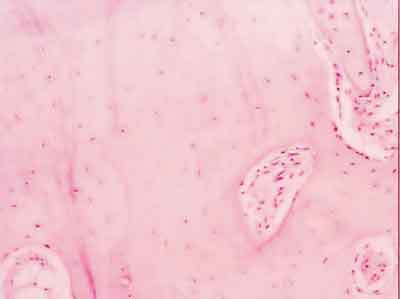
Figure 4. HE 100x photomicrography. Exophytic osteoma. Eburnean exostosis. Detail in larger magnification of previous image showing typical lamellar bone.

Print: ![]()