

Year: 2004 Vol. 70 Ed. 6 - (18º)
Relato de Caso
Pages: 819 to 822
 PDF PT
PDF PT  PDF EN
PDF ENVERTIGO AS ISOLATED MANIFESTATION OF CENTRAL NERVOUS SYSTEM DEMYELINATION - CASE REPORT AND LITERATURE REVIEW
Author(s): Washington Luís C. Almeida , Milton Pamponet da C. Moura , Wilder Alves , Luís Ricardo L. Martin , Márcio Silva de Carvalho , Keylla Cavalcante Alves.
Keywords: Key words: vertigo, demyelination, tomography.
Abstract:
Summary
The vertigo is a symptom responsible for a great number of visits to the physician's office in general. Therefore appropriate knowledge about its possible etiology and physyopathology is extremely important. We presented here a case that illustrate the various etiologies for the vertigo and the importance of the complete evaluation of the patient, always given emphasis on the clinical finds and complains.
![]()
Introduction
Vertigo may be defined as sensation of rotation dizziness or one in which spatial displacement sensation is also included. This symptom has high prevalence worldwide, especially in the elderly population, either isolated or associated with other signs and symptoms, amounting to a significant number of visits to medical offices of different specialties, especially neurologists, cardiologists and otorhinolaryngologists 1, 2.
The etiology of vertigo may be uni or multifactorial, and it may involve different organs and system responsible for body balance, including the proprioceptive system, the visual system and the vestibular system itself 2.
Concerning the vestibular system, it may be involved both in the peripheral portion, comprising the semicircular canals, utriculus-sacculus and vestibular nerve, as well as the central portion that involves the cerebellopontine angle, vestibular nuclei of the brainstem, and their cerebral cortex representation. In both situations there may be impairment by local factors (infections, traumas, tumors), such as systemic factors (arterial blood system, diabetes mellitus, degenerative demyelinating diseases) 3. Among the different causes, degenerative demyelinating diseases respond to a small percentage of vertigo cases, requiring for its diagnosis complete clinical history and well-conducted physical examination, in addition to more specific complementary exams that investigate the central nervous system 4.
Symptomatology related to balance disorders can be simply body instability in space or be associated with symptoms such as nausea, vomiting and cold sudoresis. Vertigo episodes may have varied duration and intensity, ranging from seconds to days.
We report the case of a patient that was admitted to the hospital with vertigo associated with hearing loss and mild tinnitus, whose careful investigation revealed that it was a case of degenerative demyelinating disease of undefined etiology. Based on this report, we would like to attract the attention of Otorhinolaryngologists to the possibility of facing central nervous system cases in their offices whose first manifestations are vertigo episodes, associated or not with other auditory system signs and symptoms.
Literature Review
Central nervous system alterations associated with vertigo symptomatology, isolated or not, have been well documented in the world literature. These alterations may involve a series of diseases: vascular, tumor, degenerative demyelinating 3. Similarly, transient neurological symptoms resulting from central nervous system affections may manifest as vertigo or body instability in space.
Despite the higher incidence of cases of vertigo that have their origin in the peripheral portion of the vestibular system, the cases of central origin may constitute real diagnostic dilemmas, requiring etiological investigation with complementary tests such as Brainstem Evoked Response Audiometry (BERA) and Magnetic Resonance Imaging (MRI), which can more properly assess the central nervous system 2. In such cases, the role of MRI is as the most indicated diagnostic procedure for the identification of anatomical alterations of the central nervous system that may be responsible for vertigo episodes, rarely isolated or associated with other signs or symptoms 5.
Other types of studies, such as vectoelectronystagmography and BERA are not specific and may reveal normal results even in the presence of abnormal central nervous system 6.
Posterior insula, central sulcus and inferior parietal lobule (including intraparietal sulcus) have been considered as components of the vestibular cortex, responsible for maintaining body balance in space, based in studies of human brain mapping and experiments in inferior primates. These same regions receive complementary visual, optokinetic and proprioceptive afferent projections 6.
As to etiology of vestibular disorders and their relationship with degenerative demyelinating disorders from the central nervous system, MRI is a highly sensitive test and the exam of choice when there is suspicion of such affections. Among the main causes of degenerative-demyelinating diseases of the CNS we can include multiple sclerosis, lateral amyotrophic sclerosis, and leukoencephalopathies 4.
The onset of these syndromes with initial manifestation of vertigo, associated or not with sensorineural hearing loss and tinnitus, is quite rare 4. However, there are no quantitative data about their real incidence, which justifies and recommends the assessment by MRI in patients with this symptomatology. Thus, in cases in which affections involving the vestibular system in its peripheral portion have been studied and were excluded, and in which, through conduction of complementary tests, systemic affections that trigger these syndromes showed normal results and were equally excluded, MRI investigation has to be conducted.
Case Report
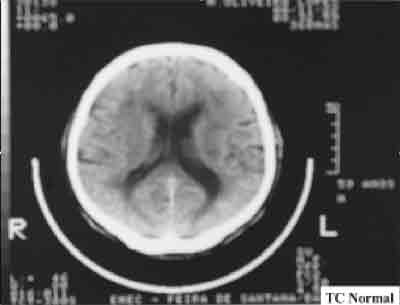
M.O.L. male patient, aged 62 years, was admitted to our center in August/01 complaining of associated hearing loss and tinnitus on the right ear for about 3 months. He reported vertigo associated with episode of syncope, which required hospital admissions, with no significant diagnosis. He presented ataxic gait. No other ENT complaints. He reported high arterial blood pressure under clinical control. Did not report the use of ototoxic drugs. There was no history of systemic affections. ENT examination and the other general physical examinations were normal. We ordered pure tone audiometry and immittanciometry that revealed mild hearing loss in high frequencies on the right, with acoustic reflexes and no other abnormalities. We ordered otoneurological assessment that showed normal results for spontaneous and semi-spontaneous nystagmus, pendulum reflex, optokinetic nystagmus, decreasing pendulum rotation and caloric tests. We also ordered biochemical assessment that showed normal results for sodium, potassium and calcium serum levels, lipid levels, proteins, glucose curve and 3-hour insulinemia, VDRL, and thyroid hormones (T3 / T4 / TSH). Hematological assessment performed by complete blood count, prothrombin time and activated thromboplastin partial time was within the normal range. He was referred to neurological assessment, which included head CT scan with no significant findings (Figure 1).
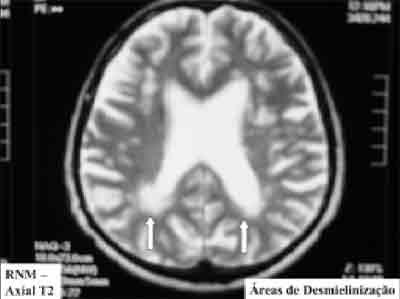
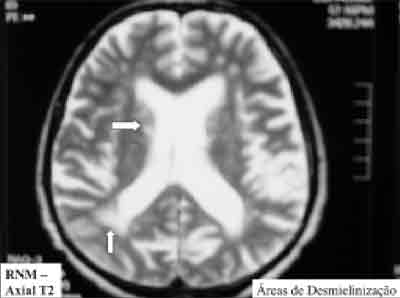
The patient came back with the same complaints and reported increase in intensity and frequency of vertigo episodes, which were nearly disabling. In view of the clinical presentation, we decided to conduct BERA that showed alteration in absolute latency times between waves I and V and also in absolute latency of waves I and II and waves III and V. We proceeded with head and inner ear MRI. Inner ear MRI did not show any abnormalities, but head MRI revealed areas of CNS demyelination, especially in peri-ventricular region, which proved to be well limited, hyperattenuating areas especially in windows T2 and FLAIR (Figures 2 and 3). Based on this new finding, we referred the patient to a new neurological evaluation with diagnostic suspicion of demyelinating syndrome, which was confirmed as the source of vertigo episodes of the patient, considering that all the other exams and tests were negative.
Discussion
The reported case showed the diagnostic difficulties that vestibular disorders may present, in addition to the importance of well-conducted clinical history and physical examination and the relevance of MRI in the final diagnosis.
In cases of permanent vertigo, in which patients have constant complaints, referring maintenance or even worsening of clinical picture despite clinical and/or behavioral management approaches attempted, with exclusion of peripheral vestibular system affections, it is mandatory to investigate the affections that may impair the CNS of the patient 7. In our investigation, MRI played an important role, given that among the available imaging exams it is the one that best portrays the central nervous system cortex, which may reveal tumor, either congenital or degenerative-demyelinating 8. We can also make use of neurophysiological exams such as BERA, which can be affected or not. In our case, the patient presented vertigo and progressive worsening associated with sensorineural hearing loss and tinnitus, which had been present for 3 months. During the investigation he had normal CT can and neurological assessment, conducted by a specialized neurologist. Despite this assessment, he still manifested vertigo episodes and we ordered BERA which showed results within the normal range, confirming what was above mentioned that such exams may be normal even in the presence of CNS affection. Only MRI revealed the abnormalities responsible for the patient's manifestations, showing area of demyelination in just-ventricular cortical area of the CNS, at sections made after gadolinium paramagnetic contrast, in windows T2 and FLAIR 9. Thus, it demonstrates the importance of this test in the investigation of CNS diseases that may manifest as vertigo episodes. We would like to emphasize the importance of ENT examination in conducting patients that come to our offices with complaints of vertigo, associated or not with tinnitus and hearing loss, excluding peripheral causes responsible for such symptoms, through comprehensive anamnesis and clinical examination and request of complementary tests, as necessary. We would like to emphasize the possibility that patients with these alterations of CNS present simply the complaint of vertigo or tinnitus, looking for support of an ENT physician first of all. Thus, the ENT physician should be attentive to all those possibilities and try to exhaust all clinical and complementary tests in an attempt to come to diagnostic confirmation.
Closing Remarks
Degenerative-demyelinating syndromes as isolated causes of vertigo symptoms are rare and their diagnosis requires high level of suspicion and ordering of the right complementary tests. Clinical suspicion stems from comprehensive clinical history and physical examination, together with complementary tests involving the peripheral vestibular system. Despite the low frequency of these syndromes in the office of the Otorhinolaryngologist, this fact does not make it less important to know the possibilities of manifestations and the correct diagnosis, referring the patient to the appropriate treatment with the neurologist.
MRI has a key role in diagnostic investigation, showing affections caused by CNS demyelination and their location, and it should always be considered as an extremely useful diagnostic tool to be used if the complaints of the patients persist and the remaining assessment and tests present results within the normal range.
References
1- Clanet,M ; Bonafe,A ; Esteve-Fraysse,MJ ; Fraysse,B. Vertigo in non-vascular diseases of the central nervous system. Rev Prat Feb 1994 ; 44(3) : 328-335.
2- Jager,L ; Strupp,M ; Brandt,T ; Reiser,M. Imaging of the labyrinth and vestibular nerve. Clinical significance for differential diagnosis of vestibular diseases. DerNervenarzt Jun 1997 ; 68(6) : 443-458.
3- Gnanamuthu,C. Transient neurological symptoms. Narrowing the vast field of causes. Postgrad Med Apr 1990 ; 87(5) : 99-102.
4- Schweri,T ; Greusing,BG. Acute vestibular deficit with initial deafness as the first manifestation of late onset multiple sclerosis. HNO Jul 1996 ; 44(7) : 397-399.
5- Mark,AS ; Seltzer,S ; Nelson-Drake,J ; Chapman,JC ; Fitzgerald,DC ; Gulya,AJ. Labyrinthine enhancement on gadolinium-enhanced magnetic resonance imaging in sudden deafness and vertigo: correlation with audiologic and electronystagmographic studies. Ann Otol Rhinol Laryngol Jun 1992 ; 101(6) : 459-464.
6- Suzuki,M ; Kitano,H ; Ito,R ; Kitanishi,T ; Yazawa,Y ; Ogawa,T ; Shiin,A ; Kitajima,K. Cortical and subcortical vestibular response to caloric stimulation detected by functional magnetic resonance imaging. Brain Res Cogn Brain Res Dec 2001 ; 12(3) : 441-449.
7- Schaefer,PW. Diffusion-weighted imaging as a problem-solving tool in the evaluation of patients with acute stroke-like syndromes. Top Magn Reson Imaging Oct 2000 ; 11(5) : 300-309.
8- Aufricht,CA ; Tenner,W ; Stiglbauer,R ; Rosenmayr,F. Transient cerebellopontine demyelinization revealed by MRI in acute cerebellar ataxia. Pediatr Radiol 1990 ; 20(8): 602-603.
9- Tan,TY ; Teh,HS. Contrast-enhanced magnetic resonance imaging of the internal auditory canals and posterior fossa. Ann Acad Med Singapore Mar 1998 ; 27(2) : 168-172.
Figure 1. Normal CT scan, axial section.
Figure 2. Axial T2 MRI section showing areas of demyelination.
Figure 3. Axial T2 MRI section showing areas of demyelination.
* Otorhinolaryngologist, Hospital Otorrinos; Ph.D. in Otorhinolaryngology, Medical School, USP.
** Otorhinolaryngologist, Hospital Otorrinos.
*** Otorhinolaryngologist; Trainee in F.E.S.S, S.B.O.R.L., Hospital Otorrinos.
**** Resident Physician in Otorhinolaryngology, Hospital Otorrinos.
***** Resident Physician in Otorhinolaryngology, Hospital Otorrinos.
****** Resident Physician in Otorhinolaryngology, Hospital Otorrinos.
Study conducted at Hospital Otorrinos - Ear, nose and throat disease, Head and Neck Surgery - Feira de Santana - Bahia - Brazil
Address correspondence to: Washington Luís de Cerqueira Almeida
Rua Barão de Cotegipe, 1141 - Bairro Centro - Feira de Santana / Bahia / Brazil
CEP : 44025-030 - Tel: (55 75) 623-4455 Fax: (55 75) 223-4117
E-mail : otorrinos@uol.com.br
Print: ![]()