

Year: 2004 Vol. 70 Ed. 3 - (19º)
Relato de Caso
Pages: 416 to 418
 PDF PT
PDF PT Pleomorphic adenoma of the nasal septum: a case report
Author(s):
Mauren P. Rocha 1,
Andréa M. Campagnolo 1,
Vanessa S. Macedo 1,
Fabiana B. Scarton 2,
Henrique P. Rocha 3,
Gabriel Kuhl 4
Keywords: pleomorphic adenoma, nasal cavity, mixed tumour
Abstract:
Nasal tumours are very rare. The neoplasms most frequently seen in the nasal cavity are epithelial papillomas, angiomas, transitional cells carcinoma, pavement carcinoma and adenocarcinoma. The pleomorphic adenoma belongs to the group of tumours less commonly observed in the nasal cavity, and is the most common head and neck benign glandular tumour. The typical clinical presentation of the nasal pleomorphic adenoma is of unilateral nasal obstruction, epistaxis and a painless mass in the nasal cavity. The authors reported an adenoma pleomorphic case that highlights itself by its unusual nasal presentation in the nasal septum of a 45-year-old male patient who was submitted to surgical treatment, and discuss the clinical findings, diagnostic criteria, treatment, prognosis and literature review.
![]()
INTRODUCTION
Nasal neoplasms are normally very rare. The most commonly observed tumors in nasal cavity are epithelial papilloma, angioma, transitional cell carcinoma, pavement carcinoma, and adenocarcinoma. Pleomorphic adenoma belongs to the groups of tumors that is less frequent in the nasal fossa, and it is a glandular benign tumor more commonly originated in the head and neck 1, 2.
Being the nose the site for many different pathologies, differential diagnosis is extremely important, and it should be made distinctly: in children, with dermoid cyst, encephaloceles, and nasal glioma; in adolescents, with juvenile angiofibroma; and in adults, with destructive tumors such as inverted papilloma, plasmocytoma, oncocytoma, fibrous histiocytoma, esthesioneuroblastoma, neuroendocrine tumors, minor salivary glands benign tumors and others 1.
We observed a case of nasal septum pleomorphic adenoma in a male patient aged 69 years and we decided to report it owing to the rarity of the clinical presentation of this location.
LITERATURE REVIEW
Pleomorphic adenoma or nasal septum mixed tumor was described for the first time in 1929 by Denker and Kahler. Next, by Stevenson, in 1932, and Weidlen, in 19361,3. Compagno and Wong, by means of studying the files of the Institute of Pathology of the American Air Force identified 40 cases of nasal cavity pleomorphic adenoma in the period between 1949 and 1974 4. It normally affects major salivary glands and rarely the nasal cavity, pharynx, larynx, trachea or lachrymal glands 5. It is presented in decreasing order of frequency in the parotid gland, submandibular gland and palate 1.
Most intranasal pleomorphic adenomas occur between the 3rd and 6th decades of life, and are normally detected in women 5. As to the origin of nasal septum pleomorphic adenoma, there are many theories about it: it would originate from embryological debris of vomer-nasal organ or Jacobson organ, a 6mm long canal with epithelial lining in the cartilaginous portion of the septum, close to the nasopalatine orifice, that normally disappears early and may persist in some adults (Stevenson, 1932); another theory would be that it originated from aberrant cells of the lining epithelium of the nasal septum (Ersner and Saltzaman, 1944); or it would originate from the ectopic salivary glandular tissue (Evans and Cruicksbank, 1970)1.
CASE REPORT
A.C.A., 69-year-old male black-descendent patient, came to the service of Otorhinolaryngology and Head and Neck Surgery, Hospital de Clínicas de Porto Alegre, complaining of repetitive massive epistaxis for approximately 1 year, requiring blood transfusion. He referred intermittent dyspnea and dysphonia for about 1 year, and nasal obstruction on the right. He did not report dysphagia and otological abnormalities. No further ENT complaints.
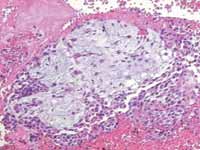
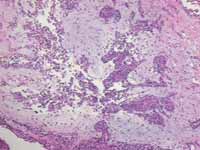
The ENT examination showed by anterior rhinoscopy a mass that obstructed the nasal vestibule, on the right, with polypoid aspect and well vascularized. Paranasal sinuses CT scan showed expansive lesion with density of soft parts, with heterogeneous impregnation of IV contrast, located in the right nasal fossa that extended up to the paranasal sinuses, right orbit, frontal sinus, sphenoid sinus, ethmoidal cell and right maxillary sinus. There was marked deviation to the left and erosion of nasal bone septum. We observed bone remodeling and erosion of medial wall on the right side maxillary sinus, medial wall of the right orbit, and ethmoidal cells on the right. There was obstruction of ostium-meatal unit on the left, with small thickness of mucous recover on the left maxillary sinus. We conducted biopsy of the lesion that diagnosed benign mixed tumor (pleomorphic adenoma). In September 2000, he was submitted to exeresis of the lesion, which occupied the right nasal fossa, and we removed the base of the tumor from the posterior-superior portion of the septum. The clinical pathological analysis showed innumerous fragments that were both irregular and bosselated with dark and elastic tissue, weighing 40g total, with diagnosis of ulcerated pleomorphic adenoma (Figure 1).
Postoperatively, he did not present any complications. The patient is still under ambulatory follow-up, without evidence of recurrence after 1 year and 8 months post-surgery.
Figure 1. Histological sections of nasal pleomorphic adenoma stained with HE, 50X.
DISCUSSION
We reported a case of nasal septum pleomorphic adenoma with an extremely rare location for this benign neoplasm and whose clinical presentation was repetitive epistaxis.
Nasal tumors are divided into two categories: the first one is represented by neoplasm of neural origin such as glioma, meningioma, olfactory neuroblastoma and neurilenoma; and the other non-neural category comprises pleomorphic adenoma, osteochondroma, chondrosarcoma, leiomyosarcoma, cystic hemangiopericytoma, adenoid carcinoma and oncocytoma 1,6.
According to Spiro et al., 11.8% of minor salivary gland tumors are benign and only 1% of the tumors are seen in the nasal cavity and nasopharynx 7. The most frequent location of pleomorphic adenoma in the nasal cavity is the quadrangular cartilage of nasal septum, and next, the nasal external wall, especially the turbinate 1.
The typical clinical presentation of patients with nasal septum pleomorphic adenoma is unilateral nasal obstruction, epistaxis and non-painful mass of nasal cavity 5.
Pleomorphic adenoma presents as a polypoid mass, smooth, lobulated, firm and encapsulated 5. For clinical pathologic diagnosis of mixed tumor, it is necessary to have two cell types: one of epithelial and the other of myoepithelial cells, and the other of stroma with fibroid, mixoid, chondroid, vascular or mixochondroid characteristics 1.
Treatment is surgical, conservative or radical, depending on the progression characteristics of the tumor 1. Distance metastases and tendency to malignant transformation are rare 8. CT scan is useful to determine the lesion limits directed to therapeutic choice. Expansive lesions are compatible with slow growth neoplasm, whereas aggressive bone destruction is a marker of malignancy 9.
Recurrence of pleomorphic adenoma is higher in components whose histological analysis is detected with greater mixoid content, which contrarily to neoplasm glands, is rare in nasal location 1, 5.
CLOSING REMARKS
The rarity of pleomorphic adenoma in this location and the success of surgical treatment motivated us to prepare this case report. It is a benign neoplasm that should be part of the differential diagnosis of nasal tumors associated with epistaxis and nasal obstruction.
REFERENCES
1. Felix J, Tonon S, Saddy J, Meirelles R, Felix F. Adenoma pleomórfico do septo nasal: relato de caso e revisão de literatura. RBORL 2000; 66:276-9.
2. Freeman S, Kennedy K, Parker G, Tatum A. Metastasizing pleomorphic adenoma of the nasal septum. Arch. Otolaryngol Head Neck Surg 1990; 166:1331-3.
3. Ersner M, Salzman M. A mixed tumour of the nasal septum: report of a case. Laryngoscope 1994; 54:287-96.
4. Compagno J, Wong R. Intranasal mixed tumours (pleomorphic adenoma). A clinicopathologic study of 40 cases. Am J Clin Pathol 1977; 68:213-8.
5. Motoori K, Takano H, Nakano K, Yamamoto S, Ueda T, Ikeda M. Pleomorphic adenoma of the nasal septum: MR features. American Journal of Neuroradiology 2000; 21:1948-50.
6. Valdezate L, Arguelles M. Adenoma pleomorfo (tumor mixto) en el septum nasal. An Otorrinolaringol Ibero Am 1994; 21:265-73.
7. Spiro R, Koss L, Hadju S, et al. Tumours f minor salivary origin. A clinicopathologic study of 492 cases. Cancer 1973; 31:117-29.
8. Golz A, Bem-Arie Y, Fradis M. Pleomorphic nasoseptal adenoma. J Otolaryngol 1997; 26(6):399-401.
9. Prager D, Buchalter W, Weiss M, Jacobs M. Pleomorphic adenoma of the nasal cavity. Ann Otol Rhinol Laryngol 1991; 100:600.
1 Resident physicians in Otorhinolaryngology, Hospital de Clínicas de Porto Alegre.
2 Ph.D. studies under course, Fundação Faculdade Federal de Ciências Médicas de Porto Alegre.
3 Ph.D. studies under course, Medical School, Universidade Federal do Rio Grande do Sul.
4 Assistant Professor, Department of Ophthalmology and Otorhinolaryngology, Medical School, Universidade Federal do Rio Grande do Sul.
Affiliation: Service of Otorhinolaryngology and Head and Neck Surgery, Hospital de Clínicas de Porto Alegre.
Address correspondence to: Mauren Péres Rocha. Rua Correa Lima, 720 apto. 306 Bairro Santa Teresa Porto Alegre RS 90850-250
Tel (55 51) 3232-5274 - Fax: (55 51) 3346-9573 E-mail: mprocha@terra.com.br
Presented at 36º Congresso Brasileiro de Otorrinolaringologia, November 18 to 23, 2002, in Florianópolis, Brazil.
Print: ![]()