

Year: 2004 Vol. 70 Ed. 2 - (15º)
Relato de Caso
Pages: 250 to 253
 PDF PT
PDF PT Tinnitus in a patient with dolichomegabasilar: a case report
Author(s):
Fransérgio E. M. Cavallari 1,
Maria Cristina L. C. Feres 2,
Miriam L Isac 3,
José A. A. Oliveira 4
Keywords: tinnitus, dolichomegabasilar, vascular compression
Abstract:
Tinnitus may appear as a symptom in a large number of pathologies, like congenital, infectious, neoplastical, neurological, traumatic, metabolical, vascular or mixed. It is presented with variable intensity, and, in its most severe form, may even undergo patient into suicide. Therefore, the differential diagnosis must be done carefully, based on different kinds of complementary tests like pure tone audiometry, imitanciometry, auditory brainstem responses and nuclear magnetic resonance. In this article, we show a case of tinnitus secondary to a rare anatomic alteration of the basilar artery, named dolichomegabasilar, leading to compression of the eighth cranial nerve, to emphasize the importance of the complementary tests on investigation and management of the tinnitus patient.
![]()
INTRODUCTION
Tinnitus can be defined as the perception of noise without detection of corresponding sound source, which can be uni or bilateral 1. It may come from different origins and with variable intensity, and in severe forms it may be highly disabling and even lead to the extreme of suicide attempt 2. It is normally perceived by the patient, reason why it is named subjective. In occasions in which observers can detect it, it is called objective.
Many lesions or diseases can lead to manifestation of tinnitus, such as congenital, infectious, neoplastic, neurological, traumatic, metabolic, mixed and vascular diseases 3.
For the differential diagnosis of tinnitus, in addition to history and physical examination that identify or exclude the diseases listed above, we should make use of complementary tests such as pure tone audiometry and immittanciometry, and especially in cases in which the patient complains of asymmetry or the results of the tests indicate it, we should conduct Brainstem Evoked Responses Audiometry - BERA. If there are any alterations, imaging exams are required, being that Magnetic Resonance Imaging (MRI) is the most appropriate one for this investigation.
BERA is very important to differentiate central from peripheral hearing loss and to detect brainstem tumors and acoustic neurinoma 4.
The purpose of the present report was to show the case of a patient with unilateral tinnitus submitted to the methods of investigation described above, leading to findings of a rare anatomical abnormality which had already been described as triggering factor of vestibular-cochlear symptoms.
CASE REPORT
V.M.A., 66-year-old male subject, born in Ribeirão Preto-SP, came to the Service of Otorhinolaryngology, Hospital das Clínicas, Medical School, Ribeirão Preto, referred from the Ambulatory of Headache of the same hospital. He had been followed up there with complaints of migraine without aura and tinnitus for 6 years. He reported continuous tinnitus on the left, insidious onset, without accompanying factors, which worsened with headache.
He had not reported hearing loss when tinnitus started, but at the time we saw him, he reported mild bilateral hearing loss, more marked on the left. He did not refer dizziness.
He had never undergone tinnitus treatment. He had already taken different types of analgesics for headache treatment.
At the first visit, we used chlorpromazine 25 mg/day and amitriptillin 25 mg BID.
He did not refer systemic hypertension, diabetes mellitus or any type of heart disorder.
Physical examination revealed normal bilateral otoscopy, no spontaneous or semi-spontaneous nystagmus, with normal vestibular and cranial nerve examination.
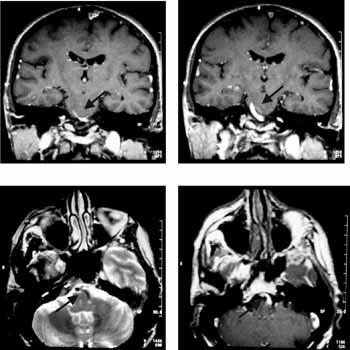
The patient was submitted to pure tone audiometry (Chart 1), in which we detected mild to moderate sensorineural hearing loss and normal results in low frequencies. Later, he was submitted to BERA (Chart 3), which revealed widening of wave I-III interval on the left. In view of this result, we ordered head MRI emphasizing the 8th cranial nerve, which showed basilar artery ectasia on the left (dolichomegabasilar), causing compression of the nerve (Figure 1).
The patient was managed with chlonazepan 2.5 mg/ml, 5 drops a day, instructed to use hearing masking, and was referred to the Service of Neurosurgery to check the possibility of undergoing surgical treatment. After careful assessment, the Service of Neurosurgery ruled out the occurrence of aneurysm formation and maintained the diagnosis of benign anatomical anomaly, excluding the possibility of surgery. The patient is currently being followed up and has good clinical control of the symptom.
DISCUSSION
Unilateral tinnitus is a symptom that attracts much attention from Otorhinolaryngologists since it is a signal that is possibly retrocochlear and strongly related with tumors, such as 8th nerve neurinoma. Normally, there are no findings in the physical examination, and complementary investigations are always required.
Patients with tinnitus present disorders associated with slowing of interpeak latencies of waves 0-I and I-V in ABR, on the affected side, showing significant reduction of amplitude of waves I and III, and sometimes of wave V. The exam allows us to indirectly check the disorder caused by tinnitus. In studies conducted by Lavernhe-Lemaire and Beutter (1989 and 1997)4, it was observed that patients with ipsilateral latency wave I-V greater than contralateral latency meant that symptoms would have central origin, whereas in patients with tinnitus of peripheral origin, ipsilateral latency I-V was lower than contralateral latency I-V. These affections were showed regardless of type or frequency of tinnitus. Finally, we can say that alterations to waves I and II, in special, are strongly suggestive of efferent systems' involvement.
In cases similarly to the one described here, based on BERA data, we should perform imaging exams to locate the nervous system problem, being that MRI is the most appropriate one; if there is suspicion of vascular lesion as tinnitus source, we should perform Angio-MRI.
Dolichomegabasilar is a generally asymptomatic rare affection, which can cause a wide range of symptoms 5, 6. There have been descriptions of cases of sudden deafness, tinnitus, vertigo, trigeminal neuralgia, facial palsy or spasms. They are rare cases, but it is essential to have differential diagnosis, since symptoms are refractory to clinical treatment in most of the cases. Diagnosis is conducted through MRI or Angio-MRI 5, 7. Treatment may be surgical, which is a precise indication in cases of aneurysm formation. Cases of vascular decompression of 8th nerve and partial section of the nerve to relieve the symptoms have already been described 8.
In the reported case, the importance of careful assessment was evident, leading to differentiation through BERA of retrocochlear unilateral pathology of well-defined cause after imaging tests. Even though it was not a surgical case, it is important to know the cause of tinnitus and to inform the patient, so that the physician can provide the right instruction to follow up the case.
Figure 1.
CLOSING REMARKS
This clinical case illustrates the diversity of causes that can generate tinnitus as a symptom. Even a characteristically retrocochlear case can originate from a pathology that is an anatomical benign variation from normal pattern. It is extremely important that professionals that manage this type of patients be aware of the fact that tinnitus is not a disease, but rather a symptom, and that the underlying disease should be exhaustedly investigated for better management of the cases.Chart 1. Pure Tone Audiometry.
Chart 2. Percentage Speech Recognition Index.
Chart 3. BERA Results.
REFERENCES
1. Schulman A. Introduction: Definition and Classification of Tinnitus. In Kitahara M. (ed): Tinnitus - Pathophysiology and Management. New York: Ikagu-Shoin; 1988, p. 1-6.
2. Hallam RS, Rachman S, Hinchecliff R. Psychological aspects of tinnitus. In Rachman R. (ed). Contributions to Medical Psychology. Oxford: Pergamon Press; 1984. p.31-4.
3. Seidman MD, Jacobson GP. Update on tinnitus. Otolaryngol Clin North Am 1996; 29(3): 455-65.
4. Lemaire MC, Beutter P. Brainstem Auditory Evoked Responses in Patients with Tinnitus. Audiology 1995; 34: 287-300.
5. Otterstedde CR, Tischendorf M, Reisser C. Megadolichobasilar artery as the etiology in sensorineural deafness in differential sudden deafness diagnosis: HNO 1999; 47(5): 494-6.
6. Guiral H, Risco J, Ferrer F. Otoneurological manifestations of basilar dolichoectasia - a report of six cases: Acta Otorrinolaringol Esp 1997; 48(5): 337-40.
7. Benecke JE Jr, Hitselberger WE. Vertigo caused by basilar artery compression of the VIII nerve: Laryngoscope 1988; 98 (8 pt 1): 807-9.
8. Meyerhoff WL, Mickey BE. Vascular decompression of the cochlear nerve: Laryngoscope 1988; 98: 602-4.
1 Resident Physician, Discipline of Otorhinolaryngology.
2 Ph.D., Professor, Discipline of Otorhinolaryngology, coordinator of the Ambulatory of Hearing Assessment and Rehabilitation.
3 Assistant Physician, Discipline of Otorhinolaryngology, responsible for the Laboratory of Hearing Electrophysiology.
4 Full Professor, Head of the Discipline of Otorhinolaryngology.
Affiliation: Medical School, Ribeirão Preto, University of Sao Paulo.
Address correspondence to: Av. Bandeirantes, 3900 12º andar Ribeirão Preto SP14090-900.
Fax (55 16)602-2860 - E-mail: mariacristina@roo.fmrp.usp.br

Print: ![]()