

Year: 2002 Vol. 68 Ed. 6 - (6º)
Artigos Originais
Pages: 811 to 814
Vocal fold module in children: diagnostic difficulties
Author(s):
N. De Biase 1,
P. Pontes 2,
L. Kyrillos 3,
J. Lourenço 4,
J. Bertti 4
Keywords: dysphonia, vocal fold, vocal nodule
Abstract:
The clinical diagnosis of vocal alterations is increasingly more accurate with development of technology and further studies in Laringology. However, diagnosis of vocal fold nodular lesions, particularly in children, is, sometimes, possible only during surgery. Aim: This paper aims at comparing clinical hypotheses and surgical findings in children with dysphonia and vocal fold nodule who underwent surgery. Study design: Chart review. Material and Method In a retrospective study, 29 records of patients aged 4-15 years, with "vocal module", and submitted to larynx microsurgery were analyzed. The clinical hypotheses were divided into three groups: vocal nodule, minimal structural alterations (MSA) and unspecific thickening. Based on these hypotheses, we made comparisons with surgical findings. Results: Fifty-nine nodular lesions in 58 vocal folds were evaluated. In the vocal nodule group, out of 8 initial hypotheses, 6 were confirmed (75%) and 1 showed thickening and 1 showed MSA. In 35 initial hypotheses of MSA, 26 were confirmed (74%), 5 switched to the vocal nodule group, and 4 to the thickening group. Out of 16 of the initial thickening group, 11 were confirmed (68%), 2 moved to the vocal nodule group and 2 to MAS group. Conclusion: Based on our material, we could conclude that clinical assessment of children with vocal fold nodule provided correct results in most cases.
![]()
INTRODUCTION
Voice is the most important means of communication for human beings; it has personal characteristics but it should always sound agreeable to the listener. The vocal fold lesions occur normally in one of the fold layers1, most of them in the recovering layer, and the most frequent lesions are vocal nodules, cysts and polyps2, 3, 4. These abnormalities modify the vocal quality and normally generate fatigue during phonation.
Vocal nodules are characterized as the presence of bilateral nodular lesions that consist of thickness of mucosa, forming a protuberance slightly below the free margin of the vocal folds, present at varied sizes, which can also be asymmetrical2, 3. It is the most frequent lesion5, 6, normally caused by vocal abuse3, 5, in subjects who present anatomical predisposition evidenced by reduced glottic proportion7.
Epidermoid cysts are abnormalities of the mucosa tunica and belong to the group of alterations named minimal structural alterations (MSA) of the vocal folds8. MSA range from simple anatomical variations up to minor congenital malformations. The clinical impact, if present, is restricted to phonation and dysphonia is consequently related to direct use of voice and the severity of the problem presented by the subject9.
Epidermoid cysts are normally located on the superficial layer of lamina propria 7, 10, 11, frequently connected with elastic or collagen fibers of the vocal ligament2, 10. Cysts can present an opening that enables spontaneous output of its content, called fistulated cysts2. They should be differentiated from pouch vocal sulcus 2, 3, 8, 10, 12 that present greater and permanent opening, with a profound depression on the vocal fold, creating a cavity inside it; this cavity, of variable deepness, is recovered by mucosa and in those cases, the vocal folds are voluminous and can present an inflammatory process frequently associated with secondary lesions, caused by pouch trauma during phonation.
MSA can present a characteristic aspect2-5, 8, 11-13 enabling the diagnosis of type of lesion9. Thus, the clinical diagnosis of vocal abnormalities is getting even more precise, thanks to the advance in technology and the studies in laryngoscopy. However, many times, the definition between vocal nodule and MSA or type of lesion is made only during surgical inspection, because cysts and pouches can present similar aspects to nodules, especially when they cause contralateral thickness6.
The pediatric larynx differs from the adult one especially concerning position, consistency and shape6, 14. Glottic proportion (GP) has values below those found in female voices, which make the children more prone to posterior opening of triangular chinks; these chinks, especially the middle posterior triangular chink, are found as part of the clinical picture of vocal nodules (Figures 1 a and 1b). In children, middle posterior or posterior triangular chinks are findings that follow low values of GP, and can be observed in cases of cysts, especially if there is no compensation tension7 (Figures 2 a and 2b). Since therapy for dysphonia depends on precise diagnosis, conducted by otorhinolaryngological clinical examination with laryngoscopy, it is important to value these other aspects that follow nodular formations.
Thus, the objective of the present study was to check the agreement between initial and final diagnoses based on clinical cases of dysphonic children that required vocal folds surgical intervention, that is, to check clinical and surgical diagnoses, since the latter is more detailed and possibly more precise.
MATERIAL AND METHOD
In as retrospective study, we analyzed 29 medical charts whose patients ages ranged from 4 to 15 years, who had vocal fold nodules and were submitted to laryngeal microsurgery. The clinical hypotheses were grouped into vocal nodule, minimal structural alterations (MSA) and non-specific thickness. Based on these clinical hypotheses, we studied the agreement with surgical findings.
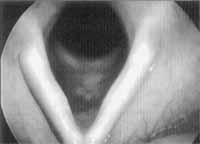
Figure 1a. Laryngeal telelaryngoscopy in a child with Vocal Nodules. Inspiration: presence of nodule on the middle 1/3 of the membranous portion of both vocal folds, of fibrotic aspect; small aperture angle.
Figure 1b. Laryngeal telelaryngoscopy in a child with Vocal Nodules. Phonation: middle posterior triangular chink and mild vestibular constriction.
Figure 2a. Laryngeal telelaryngoscopy in a child with minimum structural alteration. Inspiration: observe the sulcus in the stria minor bilateral, lower lip edema; large aperture angle.
Figure 2b. Laryngeal telelaryngoscopy in a child with minimum structural alteration. Phonation: posterior triangular chink and anterior-posterior constriction of the vestibule.
RESULTS
We observed 59 nodular abnormalities out of a total of 58 vocal folds (Tables 1, 2 and 3). For the vocal nodule group, of the 8 initial hypotheses, 6 were confirmed (75%) and one was defined as MSA and contralateral thickness, out of a total of 4 patients (Table 1). Out of the total of 35 with initial hypothesis of MSA, 26 were confirmed (74%), 5 were defined as vocal nodule and 4, as thickness (Table 2). Out of the 16 in the thickness group, 11 were confirmed (68%), 2 went to the vocal nodule group, with identification of nodular contralateral damage in one of them during the microsurgical inspection, and 2 were defined as MSA (Table 3).Table 1. Occurrence of surgical diagnosis in each vocal fold with clinical diagnosis of vocal nodule (n=4)
* 3 patients
Table 2. Occurrence of surgical diagnosis in each vocal fold with clinical diagnosis of minimum structural alteration (n=35)
* 5 patients
Table 3. Occurrence of surgical diagnosis in each vocal fold with clinical diagnosis of thickness (n=16)
* 2 patients
DISCUSSION
Thanks to the advance in technology and the studies in the area of laryngology, clinical diagnosis of vocal abnormalities has become more precise. However, especially considering MSA, the diagnosis is not always clear 6, 9 and in some cases it is only confirmed by inspection during surgery or by clinical pathology analysis. Treatment is planned for each patient based on initial diagnosis, be it vocal rehabilitation, surgery or clinical medication approach. Thus, the result will depend on the precision of the diagnosis to guide the speech therapy, since during microsurgical act it is already possible to explore and identify the lesions. For this reason, surgical diagnosis is safer, and in many occasions it is more precise in identifying MSA than clinical pathology analysis, which are normally performed in small amounts of material and without the possibility of a macroscopic examination.
The results have shown that there is not a unanimous agreement on clinical and surgical diagnoses, despite the agreement rates were quite high in most of the cases. In general, the diagnosis in pediatric patients is more difficult. The approach is more difficult because the examination involves sensations that are not pleasant, requiring cooperation and understanding to perform a laryngoscopy, which is not always the case. In many occasions, it is not possible to use the telescope, which enables more detailed visualization of the vocal folds, and the assessment has to be made with flexible optical fiber, normally because of the dimensions of the oral cavity and poor collaboration of the child. Even so, most clinical diagnoses were confirmed in the surgical act. The identification of the lesion is also more difficult because it requires the identification of posterior or middle posterior triangular chink in children with MSA, especially when there is no compensation tension (Figures 2 a and 2b). The latter, when found in adults, indicates the diagnosis of vocal nodules7. Vasculodysgenesia, when present, should be valued because they are strong indicators of MSA13.
There is another important aspect that should be kept in mind. The cases studied were surgically treated, which indicates a possibility of unsatisfactory results with conservative methods, or owing to its severity, surgical approach was decided. Thus, it is important to consider that the cases in which patients presented good results with conservative treatment were not included here, and by inference, we can conclude that the rate of success is greater than what we found. The number of cases of MSA is greater than of vocal nodules, because MSA respond less satisfactorily to voice therapy than nodules and require microsurgical treatment. Conversely, even though the studies considered that vocal nodule is the most frequent affection4, 5 it responds quite well to speech and voice therapy and there are few cases of surgical indication. In fact, when we have a case that does not respond satisfactorily to voice therapy, the possibility of another diagnosis, normally MSA, should be considered.
We obtained a general agreement rate greater than 70% considering the initial clinical and surgical diagnoses; we can state that treatments in which the three initial diagnoses are involved should be directed to them owing to the great percentage of agreement, even considering the major difficulties of performing laryngoscopy in children.
CONCLUSION
Based on the material analyzed here, we concluded that clinical assessment in children with vocal nodules provided correct diagnoses in most of the cases.
REFERENCES
1. Hirano M. Phonosurgical anatomy of the larynx. In: Ford CN & Bless DM. Phonosurgery: assesment and surgical management of voice disorders. New York: Raven Press; 1991. p.25-41.
2. Behlau M & Pontes P. Exame laringológico. In: ______. Avaliação e tratamento das disfonias. São Paulo: Lovise; 1995. p. 143-66.
3. Bouchayer M & Cornut G. Microsurgery for benign lesions of the vocal folds. Ear, Nose Throat J 1988;67:446-66.
4. Forrest LA. Treatment of benign cysts and tumors of the larynx. Otolaryngol Head Neck Surg 1995;3:149-54.
5. Gould WJ, Rubin JS, Yanagisawa E. Benign vocal fold pathology through the eyes of the laryngologist. In: Rubin JS, Sataloff RT, Korovin GS, Gould WJ. Diagnosis and treatment of voice disorders. New York: Igaku-shoin 995; 1995. p.137-51.
6. Hersan R & Behlau M. Behavioral Management of Pediatric Dysphonia. In: Rosen C & Murry T. Voice Disorders and Phonosurgery II. Otolaryngol. Clin North Am 2000;33(5):1097-110.
7. Pontes P, Kyrillos L, Behlau M, De Biase N, Pontes A. Vocal Nodules and laryngeal morphology. J Voice (submited)
8. Pontes P, Behlau M, Gonçalves I. Alterações estruturais mínimas da laringe (AEM): considerações básicas. ACTA AWHO XIII 1994 ;(1):2-6.
9. Pontes P, Gonçalves MI, Behlau M. Vocal fold cover minor structural alterations: Diagnostic Errors. Phonoscope 1999;2(4):175-185.
10. Hirano M, Yoshida T, Hirade Y, Sanada T. Improved surgical technique for epidermoid cysts of the vocal fold. Ann Otol Rhinol Laryngol 1989;98:791-5.
11. Mondey LA, Cornut G, Bouchayer M, Roch JB. Epidermoid cysts of vocal cords. Ann Otol Rhinol Laryngol 1983;92:124-7.
12. Bouchayer M & Cornut G. Le sulcus glottidis: essai de clarification nosologique et étio-pathogénice. Revue Laryngol 1987;(suppl):391-2.
13. Pontes PAL, De Biase NG, Behlau M. Vascular characteristics of the vocal fold cover in control larynges and larynges with benign lesions. Phonoscope 1999;2(3):129-35.
14. Vallancien B. Disfonia funcional da infância. In: Launay C & Borel-Maisonny S. Distúrbios da Linguagem, da Fala e da Voz na Infância. São Paulo: Roca; 1986. p. 340-61.
1 Ph.D., Assistant Professor, Department of Basic Sciences, School of Speech and Language Pathology and Audiology, Pontifícia Universidade Católica de São Paulo SP.
2 Faculty Professor of Otorhinolaryngology, Federal University of São Paulo Escola Paulista de Medicina, São Paulo SP.
3 Ph.D., Assistant Professor, Department of Speech and Voice, School of Speech and Language Pathology and Audiology, Pontifícia Universidade Católica de São Paulo SP.
4 Speech and Voice Therapist, Specialist in Vocal Rehabilitation.
INLAR Instituto da Laringe São Paulo SP
R. Dr. Diogo de Faria, 171 Vila Clementino 04037-000
Tel (55 11) 5549.2188 E-mail: nbiase@terra.com.br or ppontes@inlar.com.br
Study presented at II Congresso Triológico de Otorrinolaringologia, in Goiânia, 2001.
Article submitted on March 26, 2002. Article accepted on June 6, 2002






Print: ![]()