

Year: 2003 Vol. 69 Ed. 3 - (21º)
Relato de Caso
Pages: 432 to 434
 PDF PT
PDF PT Primary synovial sarcoma of the oropharinx: a case report
Author(s):
Hugo Meister 1,
Thaís C. Miranda 2,
Manuel G. G. Nóbrega 2
Keywords: synovial sarcoma, neoplasia, head and neck
Abstract:
Primary synovial sarcoma of the head and neck is a rare tumor. Fewer than 90 cases having been reported in the literature. This report presents an addicional case of synovial sarcoma involving the oropharinx in a young man. Microscopically the tumor showed a biphasic pattern of pseudo-ephitelial cells and a spindle cell element with fibrosarcomatous and epithelial appearance. A proper diagnosis was done after routine pathological and immunohistochemical studies of the ressected tumors.
![]()
INTRODUCTION
Synovial sarcoma (SS) is a primary malignant neoplasm of soft tissues. Most of these tumors develop in the neighborhood of large joints, being that 60 to 70% of the cases affect the lower extremities, especially close to the knee 1.
Other locations are rare, such as abdominal wall and head and neck regions 1.
There are about 90 cases of head and neck SS described in the literature 2.
The histogenesis of SS is still controversial. Despite its name, it may affect sites in which there is no synovial tissue 5. It is believed that the tumor can originate from original mesenchymal tissue or specialized arthrogenic tissue 4.
The purpose of the present study was to present an additional case of SS of the head and neck region.
CASE REPORT
A male 19-year-old patient came for medical care complaining of sore throat. Clinical examination revealed increase in the upper pole of the left tonsil. The general status of the patient was good and there were no cervical lymph nodes upon palpation. Lab routine tests were within the normal ranges. Despite medication with antibiotics an anti-inflammatory drugs, the lesion developed with quick and progressive growth. Since there was suspicion of neoplasm, the patient underwent tonsillectomy.
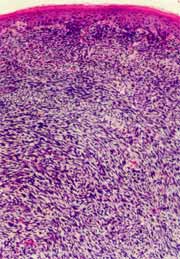
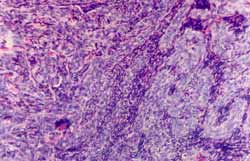
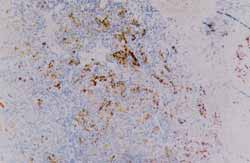
The surgical specimen was submitted to clinical pathology and it consisted of a whitish tumor mass of irregular surface, granulous and bleeding, measuring 3 x 3 x 2 cm at the largest diameters. The material was processed according to the regular techniques and histology study, with routine preparations of hematoxyllin-eosin staining, which revealed malignant neoplasm with biphasic growth, fibrosarcomatous (Figure 1) and epithelial aspect, with pseudoglandular structures (Figure 2). Upon the investigation with immunohistochemical analysis, epithelial cells were positive to cytokeratin (Figure 3) and the epithelial membrane antigen (EMA) and positive spindle cells to vimetin and focally to cytokeratin. There was no expression of S-100 protein.
Figure 1. Fibrosarcomatous dissemination of subepithelial squamous mucosa. HE staining 100x.
Figure 2. Fibrosarcomatous spindle cell proliferation with pseudoglandular epithelial structures. HE staining 100x.
Figure 3. Positive immunereaction to cytokeratin of pseudoglandular epithelial structures. Avidin - Biotin - Peroxidase, 40x.
DISCUSSION
SS rarely affects the region of the head and neck. It was described for the first time in this location by Jernstron in 19545.
It is estimated that 3 to 10% of SS affect the head and neck 2, 6-9. Out of 345 cases of SS reviewed by Enzinger and Weiss, 31 had this location 1, being that the most frequently affected areas were parapharynx 6, 19 and hypopharynx 7, 10, 11.
Other locations described comprised the tonsil 10, 11, tongue base 6, 11, 12, nasopharynx 4, palate 13, larynx 7, 8 and oral mucosa 2, 14, 15.
Less than 10% of the neoplasm affects the joint 1. Some authors consider SS of the head and neck only as tumors originated from the non-articular tissues 8.
Therefore, the diagnosis is made not necessarily if the tumor is close to a joint 13. Salisbury and Isaacson4, using monoclonal epithelial specific antibodies observed that despite histology similarities, epithelial cells of SS predominantly contain cytokeratins, whereas normal synovial cells contain exclusively vimetin. Such findings conformed the proposition that SS would not originate from the normal synovial tissue 1, but rather from the ordinary mesenchymal tissue or arthrogenic specialized tissue 4, which represents the expression of versatility of the mesenchymal tissue 5.
Enzinger and Weiss1 classified them in 4 groups based on microscopy morphology: biphasic, spindle cell monophasic, epithelial monophasic and little differentiated. Typically, the tumor has a biphasic pattern 8, 9, 11, 15, with the fibrosarcomatous and epithelial spindle cell component with pseudoglandular structures. The spindle cell monophasic pattern can be mistaken by other sarcomas, among which fibrosarcoma, leiomyosarcoma and malignant schwanoma.
Upon immunohistochemical study, SS co-expresses mesenchymal markers (vimetin) and epithelial markers (cytokeratin, EMA). Positive reactions to vimetin occur only in spindle cells. It has been described that there may be positive response to S-100 protein.
Similarly to extremity SS, the neoplasm affects especially young people 8, 9, 15, and male subjects 10, 15.
In the head and neck region, SS can have an indolent course. It normally presents slow and non-painful growth and non-specific symptoms. The most frequent clinical manifestations is the presence of a non-painful cervical nodule 2, 10. Depending on the location, there may be compressive symptoms.
Micro-calcifications, size smaller than 4 cm, early age, biphasic tumor growth pattern and small tumor extension are associated with better prognosis 6, 9, 10. Metastases occur in 10 to 15% of the cases 8, especially by hematogenic route 6, 10.
The treatment includes wide surgical exeresis, with free margins and adjuvant or neoadjuvant radiotherapy. There are no data concerning the efficacy of chemotherapy in such types of tumors 2, 6, 8-12.
Five-year survival ranges from 40 to 50% 6, 8, 10 and 10-year survival is 10 to 30% 9. Local tumor recurrences are normally present in 30 to 50% of the cases 9.
CLOSING REMARKS
Tonsillary hypertrophy is a frequent occurrence in ENT visits. For this reason, there is the risk of oversimplifying the etiological diagnosis, considering first inflammatory processes. Unilateral affection, resistance to conventional treatment and progressive growth are important data for suspicion of neoplastic disease. Low frequency of SS of the head and neck prevents us from considering this diagnosis in the first clinical examination.
REFERENCES
1. Enzinger FM, Weiss SW. Soft tissue tumors. 3rd ed. St. Louis: Mosby; 1995. p.757-86.
2. Doval DC, Kannan V, Mukherjee G, Shenoy AM, Shariff MH, Bapsy PP. Synovial sarcoma of the neck. Eur Arch Otorhinolaryngol 1997;254(5): 246-50.
3. O'Keefe LJ, Ramsden RT, Birzgalis AR. Primary synovial sarcoma of tha middle ear. J Laryngol Otol 1993;107(11): 1070-2.
4. Salisbury JR, Isaacson PG. Synovial Sarcoma: an Immunohistochemical Study. Journal of Pathology 1985;147: 49-57.
5. Jersnstrom P. Synovial Sarcoma of the pharynx. Report of a Case. Am J Clin Pathol 1954;24: 957-61.
6. Carrillo R, Rodriguez-Peralto JL, Batsakis JG. Synovial sarcomas of the head and neck. Ann Otol Rhinol Laryngol 1992;101(4): 367-70.
7. Dei Tos AP, Dal Cin P, Sciot R, Furlanetto A, Da Mostro MC, Giannini C, Rinaldo A, Ferlito A. Synovial sarcoma of the larynx ans hypopharynx. Ann Otol Rhinol Laryngol 1998;107(12): 1080-5.
8. Gimenez F, Vera JM, Ibarra F, Perez F, Carbonell R, Lozano I. Cervical synovial sarcoma: a case report. Acta Otorrinolaringol Esp 1996;47(1): 79-81.
9. Herrero Laso JL, Varela Duran J. Oropharyngeal synovial sarcoma. Report of one case. An Otorrinolaringol Ibero Am 1998;25(4): 353-9.
10. Bukachevsky RP, Pincus RL, Shechtman FG, Sarti E, Chodoch P. Synovial sarcoma of the head and neck. Head Neck 1992;14(1): 44-8.
11. Engelhardt J, Leafsteddt SW. Synovial sarcoma of tonsila and tongue base. South Med J 1983;76(2): 243-4.
12. Holtz F, Magielski JE. Synovial sarcomas of the tongue base. The seventh reported case. Arch Otolaryngol 1985;111(4): 271-2.
13. Massarelli G, Tanda F, Salis B. Synovial sarcoma of the soft palate: report a case. Hum Pathol 1978;9(3): 341-5.
14. Amble FR, Olsen KD, Nascimento AC, Foote RL. Head and neck synovial cell sarcoma. Otolaryngol Head Neck Surg 1992;107(5): 631-7.
15. Araújo VC, Monteiro DC. Oral Synovial Sarcoma: Report of a Case. J Oral Maxillofac Surg 1989;47(9): 1001-3.
1 Assistant Professor, Discipline of Clinical Pathology, Medical School, State University of Maringá.
2 Undergraduate, Medical School, State University of Maringá.
Address correspondence to: Dr. Hugo Meister - Rua Néo Alves Martins 3377, 3º andar, sala 302 Maringá, PR 87013-060 - E-mail: lapam@onda.com.br
Article submitted on May 23, 2002. Article accepted on July 04, 2002.
Print: ![]()