

Year: 2003 Vol. 69 Ed. 3 - (19º)
Relato de Caso
Pages: 421 to 425
 PDF PT
PDF PT A late diagnose of malformation of ear tube: case report and review of literature
Author(s):
Eliézia H. L. Alvarenga 1,
Fabiana N. R. Maia 2,
Márcia A. Souza 3,
Oswaldo L. M. Cruz 4
Keywords: secretory otitis media, AIDS, malformation
Abstract:
The malformation of the ear tube is a rare condition usually diagnosed in children with recurrent otitis or deafness. There are no reports available in the medical: literature attempting to this congenital malformation in older, patients. The authors report a case of an old man with unilateral secretory otitis media and malformation of ear tube.
![]()
Introduction
The diagnosis of unilateral secretory otitis media (SOM) in adults requires careful investigation in order to rule out diseases of the nasopharynx, especially tumors. A common manifestation of nasopharyngeal neoplasm in adults is unilateral secretory otitis media and it is less frequent as bilateral diagnosis 1, its incidence ranges from zero 2 to 1.5% 3. Therefore, nasal endoscopy is an essential part of the assessment of these patients, enabling the analysis of the canal cavity and rhinopharynx.
Differential diagnosis of the rhinopharynx disease that provides secretory otitis media includes a wide range of affections (Table 1), and they can have similar normal mucosa presentation in the endoscopy, reason why the clinical pathology is essential to identify the affections of the mucosa 4. Therefore, biopsy and computed tomography of the nasopharynx are important resources in the diagnosis of unilateral secretory otitis media in adults.
In Brazil, there has been an increase in the number of AIDS cases in the elderly and the proportion of affected subjects between the years of 1991 and 2000, especially in women 5. The contamination route of heterosexual transmission is significantly more important. Currently, owing to the increase in the number of HIV-infected cases, secretory otitis media can lead us to the hypothesis of lymphoid hyperplasia of the nasopharynx, since a decrease in CD4 and an increase in CD8 can induce to the growth of adenoid tissue and sometimes auditory tube obstruction 6, 7.
In elderly patients with AIDS, there are frequent neoplasms associated with HIV infections, such as Kaposi's sarcoma and non-Hodgkin lymphomas 8. Kaplan et al.9 noticed that ¾ of the solid tumors in AIDS patients occurred in the elderly.
Auditory tube malformations normally have early manifestations, even though the review of both Brazilian and international literature for the past 25 years did not find any study presenting isolated auditory tube malformation, regardless of the age range. Therefore, we would like to highlight how rare our case is: unilateral SOM in an elderly patient with AIDS for one year, after upper airway infection, with no history of previous otitis media, no nasopharynx surgical intervention (adenoidectomy), in which we observed and confirmed auditory tube malformation.
CASE REPORT
A.F., male patient aged 72 years, born in Portugal. The patient referred hearing loss and tinnitus on the left for 4 months. He reported that it all started with a complicated cold, leading to acute otitis media that was treated by the infectologist with conventional antibiotic. No nasal complaints. History of pulmonary tuberculosis for 1 year when the diagnosis of AIDS was made. He does not refer previous episodes of otitis media or ENT surgery.
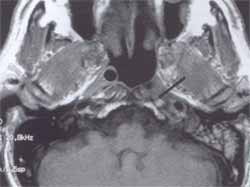
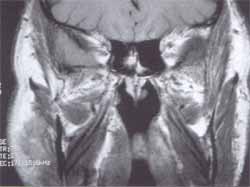
Upon ENT examination, the left tympanic membrane was retracted and opacified by vascular striae, anterior rhinoscopy and oroscopy within the normal range. We conducted nasofibroscopy and detected absence of torus tubarius and orifice on the left (Figures 3 and 4). The hearing assessment detected unilateral conductive hearing loss on the left, tympanometry curve B, bilateral absent stapedial reflexes. We administered clinical treatment for secretory otitis media with corticoids. We ordered magnetic resonance imaging (MRI) of the nasopharynx owing to absence of torus tubarius on the left, and it did not evidence membranous path of the auditory tube, but there was the probable presence of the lateral portion (bone portion) of the auditory tube (Figures 1 and 2).
We did not succeed with clinical treatment and indicated tympanotomy and long duration ventilation tube placement, leading to remission of symptoms immediately after the surgery. Two months after the surgery, the patient presented left otorrhea through the tube, despite all care and treatment with otologic drops that contained antibiotics and corticoids. Four months of follow-up and there was continuous otorrhea and extrusion of the ventilation tube. We started treating with systemic antibiotics and corticoids, and the patient presented improvement of otorrhea and hearing. Six months postoperative, the patient maintained tympanic perforation at the tympanometry site with dry middle ear.
Figure 1. Magnetic resonance imaging of paranasal sinuses (axial section).
Figure 2. Magnetic resonance imaging of paranasal sinuses (coronal section).
Figure 3. Torus tubarius agenesis and left auditory tube shown by nasofibroscopy.
Figure 4. Right torus tubarius shown by nasofibroscopy.
DISCUSSION
HIV infection is frequently diagnosed in the elderly only after marked investigation and exclusion of other diseases, delaying the diagnosis of infection during months (AIDS). In such case, the diagnosis of AIDS was only defined after the clinical presentation of pulmonary tuberculosis.
Despite the similarity of the opportunistic diseases in infected elderly, these patients normally present poor prognosis when they have such infections. It is assumed that the prognosis is poorer because they have less functional reserve; the elderly presents physiological decline of the immune function, especially of T cells, greater viral load during serum conversion, previous exposure to the agent and treatment (generating resistant forms) and intolerance to drugs 10, 11.
Dempster and Simpson12 questioned the cost-benefit of the nasopharynx biopsy in the routine study of adults that presented secretory otitis media in the presence of clinically normal nasopharynx. However, differently from other neoplasm such as angiofibroma and lateral recess of the nasopharynx (Rosenmüller fosset), not always they are clinically present, even in the presence of metastatic disease. An extended biopsy of the rhinopharynx is recommended. The positive biopsy, is unquestionably, low, but failure to make he diagnosis of cancer implies severe complications.
The normal appearance of the nasopharynx mucosa is not necessarily a reliable indicator of absence of malignancy since submucous tumors can exist, such as those described by Lee et al13, who concluded that deep biopsy of the nasopharynx should be made in adult patients with unilateral secretory otitis, preventing lack of diagnosis or late diagnosis of neoplasm.
Yung and Arasaratnam14 observed 11 of 53 (20%) patients with SOM who presented endoscopic evidence of inflammation of the nasal lateral wall and confirmed that 51% of the patients had evidence of inflammation of the torus tubarius, in a period of 15 to 27 months of follow-up after placement of ventilation tube. The occurrence of SOM after extrusion of ventilation tube was detected in 19 out of 31 patients (61%) and 4 of 22 patients (18%) still maintained the ventilation tube and presented persistence of otorrhea. In addition, they did not observe endoscopic differences in the nasopharynx and lateral wall of the nose between the groups with and without recurrence of secretory otitis media, and over 50% of all patients had previous history of tympanotomy and placement of ventilation tubes. They concluded that simply placing ventilation tubes in SOM in adults is a procedure that yields limited results, whereas in children 70% of the cases are solved after the primary placement of the ventilation tube and 20% after the placement of the second ventilation tube. Yung and Arasaratnam14 observed an association between secretory otitis media and atopy. In a sample with 53 patients, 23 (43%) had history of atopy and 30 (57%) had positive skin test.
The results of the treatment of secretory otitis media in adults are well defined. It is known that secretory otitis media secondary to nasopharynx carcinoma does not respond well to ventilation tubes and frequently leads to persistent otorrhea through the ventilation tubes 15.
Similarly to any other malformation, we expect manifestations in early childhood, especially in the malformation of the auditory tube since there is prevalence of upper airway infections in this area and age range, which may progress to repetitive otitis media and secretory otitis media, following the continuum that takes to chronic otitis media. However, in the comprehensive literature review both including Brazilian and international studies, we did not find any case of isolated auditory tube malformation. What is curious and intriguing about this case is that the first otitis episode was one year after the diagnosis of AIDS in a 72-year-old patient, and endoscopy revealed absence of ipsilateral torus tubarius, a fact confirmed by MRI - malformation of the membranous path of the auditory tube.
In our case, we concluded that it was a congenital malformation case based on the findings of MRI and fibroscopy. In the MRI, the membranous portion of the auditory tube had a homogeneous aspect, with no neoformation, inflammatory activity and indications of fibrosis in the region that could occlude the tube lumen. Fibroscopy did not identify the presence of a torus tubarius and pharyngeal orifice of the tube, and the mucosa that recovered the region had normal aspect, agreeing with the MRI findings.
In the present case of SOM in an elderly subject with AIDS, with malformation of the auditory tube, we decided to place prolonged ventilation tubes, which initially improved the clinical picture and then progressed to persistent otorrhea and extrusion of the tube 4 months after the surgery. It is important to point out that in an elderly patient with AIDS we could not expect better results, since we believe that hyperreactivity of the mucosa is associated with immune affections, maintaining otorrhea, despite the ventilation tube. Reinforcing this hypothesis, we have observed periods of intermittent otorrhea through the perforation of the tympanic membrane (site where the tubes were placed), despite all recommended care.Table 1. Causes of secretory otitis media in adults.
CLOSING REMARKS
Disagreeing with the knowledge that malformation symptoms are manifested in childhood and upper airway infections present greater prevalence in childhood, we expected auditory tube malformation to manifest as chronic otitis media in this age range. It is intriguing that the otitis case of our patient had its first episode at the age of 72 years, one year after pulmonary tuberculosis that led to the diagnosis of AIDS. Acute otitis media developed to secretory otitis media and in the unilateral investigation of SOM in an adult, it required the conduction of an endoscopy. In an elderly patients with AIDS we expected to observe an increase in nasopharyngeal lymphoid tissue obstructing the auditory tube, or even a tumor. However, what we observed was a wide nasopharynx and absence of ipsilateral torus tubarius and the MRI confirmed the endoscopic findings with absence of the cartilaginous portion of the auditory tube.
REFERENCES
1. Gacek RR. A differential diagnosis of unilateral serous otitis media. Laryngoscope 1992;102:461-8.
2. Robinson PM. Secretory otitis media in the adult. Clinical Otolaryngology 1987;12(4):297-302.
3. Gaze MN, Keay DG, Smith IM, Hardcastle PF. Routine nasopharyngeal biopsy in adult secretory otitis media. Clinical Otolaryngology 1992;17(2):183-4.
4. Osinubi OA, Thomas RSA, Lauder I. A rare cause of unilateral hearing loss. Self assessment questions 1999;584-5, 588-9.
5. Lucente FE. Aspectos Otorrinolaringológicos da síndrome da imunodeficiência adquirida. Clínicas Médicas da América do Norte 1991;6:1429-38.
6. France AJ, Kean DM, Douglas RHB. Adenoidal Hypertrophy in HIV infected patients. The Lancet 1988;2:1076.
7. Oksenhendler E, Lida H, D'agay MF. Tumoral nasopharyngeal lymphoid hyperplasia in human immunodeficiency virus-infected patients. Arch Intern Med 1989;149:2359-61.
8. Gordon S, Thompson S. The changing epidemiology of human immunodeficiency virus infection in older patients. Journal Am Geriatr Soc 1995;43:7-9.
9. Kaplan M, Susin M, Pahwa S et al. Neoplastic cs of HTLV III infection. Am J Med 1987;82:382-95.
10. Ferro S, Saht I. HIV Infection in patients older 55 years of age. J Acquire Immune Defic Syndr 1992;5:348-55.
11. Melo MR, Gorzoni M, Melo KC, Melo E. Síndrome da Imunodeficiência Adquirida no idoso. Revista Diagnóstico e Tratamento 2002;7(2):13-7.
12. Dempster JH, Simpson DC. Nasopharyngeal neoplasms and their association with adult onset otitis media with effusion. Clinical Otolaryngology 1988;13:363-5.
13. Lee WC, Weiner GM, Campbell JB. Should nasopharyngeal biopsy be mandatory in adult unilateral glue ear? J Laryngol Otol 1996;110:62-4.
14. Yung MW, Arasaratnam R. Adult-onset otitis media with effusion: results following ventilation tube insertion. J Laryngol Otol 2001;115:874-8.
15. Morton RP, Wollons AC, Mcivor NP. Nasopharyngeal carcinoma and middle ear effusion: natural history and the effect of ventilation tubes. Clin Otolaryngol 1994;19:529-31.
1 Master in Otorhinolaryngology, Medical School of Ribeirão Preto - FMUSP, Doctorate studies in Otorhinolaryngology under course, EPM.
2 Collaborating physician, Clinical Otorhinolaryngology, Hospital das Clínicas da FMUSP.
3 Ph.D. in Otorhinolaryngology, UNIFESP - EPM.
4 Full Professor, FMUSP.
Address correspondence to: Eliézia Helena de Lima Alvarenga - Rua Conselheiro Brotero, 1539/104 Higienópolis São Paulo SP 01232-011
Tel (55 11) 3826-8001 - E-mail:elalvarenga@aol.com.br
Article submitted on August 14, 2002. Article accepted on August 29, 2002.


Print: ![]()