

Year: 2001 Vol. 67 Ed. 4 - (8º)
Artigos Originais
Pages: 499 to 505
The Importance of Nasal Fiberoptic Examination to Dose Adenoid Hiperplasia in Children With Normal Paranasal Sinuses X-ray.
Author(s):
Renato C. Oliveira*,
Wilma T. Anselmo Lima**,
Bruno B. Souza***.
Keywords: adenoids, nasal obsctrution, fiberoptic examination in children
Abstract:
Introduction: The introduction of the fiberscope in clinical examination of the nasal cavity and nasopharynx has been of great value, especially when adenoidectomy is indicated. Study design: Clinical prospective. Material and method: We have studied 60 children aged between four and 12 years, presenting chronic nasal obstruction refractory to medical treatment and normal paranasal sinuses X-ray. There were 45 subjects from HCFMRP (Hospital das Clínicas, Faculdade de Medicina de Ribeirão Preto), and 15 from Hospital São Paulo, in Cianorte, Paraná. Nasal endoscopy was performed in all children in order to check the presence of adenoid hyperplasia regardless the normal X-ray finding. Results: The fiberscopic findings showed 27% (17 cases) of adenoids considered large, 42% (24 cases) moderate, and 31% (19 cases) small. In addition, we also found eight cases of hypertrophy of the posterior region of the inferior turbinates (13.3%) and four cases of posterior septal deviation. Conclusion: The results of our study showed the importance of nasal fiberscopic examination in children, providing a straight, three dimensional and dynamic evaluation of the paranasal sinuses area.
![]()
INTRODUCTION
Chronic nasal obstruction (CNO) is the most frequent clinical complaint in childhood, normally caused by adenoid hyperplasia. In such cases, adenoidectomy provides relief of the main symptoms of obstruction, which would contribute to improve other surrounding infection diseases, such as middle ear and paranasal sinuses infections. In Belgium, for example, in 1988, 23,638 adenoidectomies were performed and in 1989, 25,568 cases were operated on, among a population of approximately 9.5 million inhabitants24.
There are a number of causes of CNO in childhood and they may lie in the nasal cavities and/or nasopharynx. In the first year of life, clinical investigation should be directed to stenosis and choanal atresia. Other causes, such as mucosal edema, cysts and tumors, should also be excluded. Butugan et al. (1999)3, in a study of childhood nasal tumors, in patients aged one to 12 years, for a period of 15 years, at Hospital de Clínicas da USP, related 23 patients with an incidence of 6/1 in males. Ninety-one percent of the patients presented CNO and juvenile nasoangiofibroma was diagnosed in 60.7% of the cases.
Adenoid hyperplasia and hypertrophic rhinitis are the most common caused of CNO in children. The increase of adenoid tissue takes place between the ages of 3 and 7 years. Physiological involution normally starts after 6 years of age, continuing until the adolescence. Although infrequent, it may happen at adult age, such as in the 35 cases of adenoid growth in subjects aged 20 to 42 years described by Kamel et al., in 1996.
The enlargement of adenoid may determine a partial or total blockage of choanae. Classically, the signs considered indicative of nasal obstruction due to adenoid hyperplasia are mouth breathing, hyponasal speech and snoring1,15,20. History of persistent rhinorrhea, post-nasal dripping and chronic cough is common but they are not adenoid hyperplasia-specific. They may also be present in cases of chronic adenoiditis, allergic rhinitis and chronic rhinosinusitis 2. Adenoid face is characterized by opened mouth, elongated face and anterior open bite, normally a consequence of upper airway obstruction, especially because of adenoid hyperplasia10.
Moreover, various authors have found a correlation between adenoid and otitis media with effusion and recurrent otitis media and nasosinusal diseases5,13,21,23.
Alterations of facial growth that occur as a result of CNO manifest as a series of important clinical signs. There may be compromise of facial bone growth pattern, dental arches (malocclusion), skull-mandible function and palate shape (high vault palate).
Therefore, diagnosis should be clearly made, even in patients who do not have strong clinical and radiological suspicion, preventing the application of other unsatisfactory therapeutic methods.
Investigation methods of CNO in children
In 1842, Macleod Yearsly performed the first adenoidectomy, which later was described in details by Wilhelm Meyer, in 18681. From that time on, we have been trying to define which investigation methods would be the most reliable to diagnose the causes of CNO in children. The examination of rhinopharynx with digital palpation and the use of mirror through the oral cavity to perform posterior rhinoscopy have been abandoned because they were traumatic and difficult to perform in children6.
Radiological tests are still widely used and visualization of rhinopharynx may be reached with lateral incidence of the face; moreover, the child should have the mouth closed and be during inspiration. Some studies conducted throughout the years have shown that all children over 6 months of age present adenoid tissue visible at radiological imaging, and they consider that x-ray is an acceptable method to evaluate the size of adenoids and the air space of rhinopharynx7,8,12,14,16,17.
Wormald and Prescott (1991) concluded that the radiological method of Cohen and Konak7 is that one that presents the best correlation with the findings of the endoscopic assessment25 when evaluating the air space of rhinopharynx.
CT scan and MRI are nor used as routine for diagnosis of chronic nasal obstruction in children.
Computed rhinomanometry and acoustic rhinometry are objective tests that may support the professional in the surgical indication of adenoid and/or tonsil hypertrophy. As to computed rhinomanometry, the main problem is the limitation of the test in children, who frequently reject the placement of the facial mask. Acoustic rhinometry is a simple and quick test to be conducted in children, at any age range, because it is noninvasive and requires minimal cooperation from the patient. Currently, special adapters for small nostrils (even in babies) have been successfully used. Despite the easy handling and the promising results, the few studies published in the literature showed inconclusive and controversial results.
Nasal fiberoptic test, in turn, enables observation of critical and inaccessible endonasal areas by traditional rhinoscopy. The first nasal-sinusal rhinoscopy was successfully performed for the first time in 1901, by Hirschmann, using a Nitze cytoscope26. In 1971, as a result of the development of Hopkins telescopes with optic systems formed by cylindrical lenses and supplied with coaxial illumination by optical fiber, the quality of the endoscopic image improved considerably. The illumination is more intense, the visualization angle is larger, and the focal distance is accommodated to the infinite, without distortion of images. Thanks to the development of flexible optic fibers, with excellent quality (nasal fiberscope), it has been possible to have direct and safe visualization of rhinopharynx, important for the selection of children with the indication of adenoidectomy4.
Figure 1. Normal paranasal sinuses x-ray.
Figure 2. Patient submitted to rigid fiberoptic examination.
The purposes of the present study were:
To clinically evaluate children with chronic nasal obstruction and normal paranasal sinuses x-ray;
To demonstrate, through nasal fiberscopic findings, that adenoid hyperplasia may by the cause of chronic nasal obstruction in children with normal paranasal sinuses xray.
MATERIAL AND METHOD
Patients
The sample consisted of 60 children with CNO aged 4 to 12 years, during August 1996 and May 1999, seen at the Ambulatory of Rhinosinusology at HCFM-RP/SP and Hospital Sao Paulo, in Cianorte/PR.
Radiological assessment
All patients were submitted to simple paranasal sinuses x-ray. They were positioned at standing position, at a distance of 180 cm from the tube and exposed to 100 Kv and 50 mA, from 0.4 to 0.6 seconds of exposure, depending on the age of the child.
We also performed radiological analysis to evaluate the size of the adenoid in relation to the nasopharynx.
We used the method by Cohen and Konak (1984)7. Patients who presented normal radiological analysis were submitted to nasal flberoptic examination that same day (Figure 1).
Nasal fiberoptic examination
We used two types of nasal fiberscopes:
a) Flexible nasofiberscope - Fujinon, 2.7 mm, associated to a micro camera Toshiba and light source Pentax LX 3000.
b) Rigid nasofiberscope - Hopkins (Karl Storz Germany), 30°, associated to a micro camera telecon-C NTSC and light source Endolux (H. Strattner), halogen source of 250 W 14' Video monitor Panasonic21.
All examinations were recorded in video, allowing revaluation and classification of the severity of adenoid obstruction.
Conduction of examinations
Children were maintained in the examination room with their parents. They were seated and received a cotton ball soaked in xilocaine spray at 10% and epinephrine at 1 % in each nostril, for about 10 to 15 minutes. We used inferior and middle meatus as the route of access to collect images from the posterior nasal space and rhinopharynx (Figure 2).
Measure of size of adenoids
The parameter used to classify the size of adenoids by nasal fiberoptic examination was the distance from the vomer to the adenoid tissue, classified in three groups23:
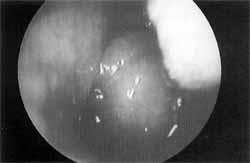
Figure 3. Image of large sized adenoids
a) Small adenoid: distance > 1 cm - obstruction < 40%;
b) Moderate adenoid: distance from 0.5 to 1 cm - obstruction between 40% and 60%;
c) Large adenoid: distance < 0.5 cm - obstruction > 60%.
RESULTS
Age of patients varied from 4 to 12 years (mean age of 8.4 years), divided into 33 male and 27 female patients.
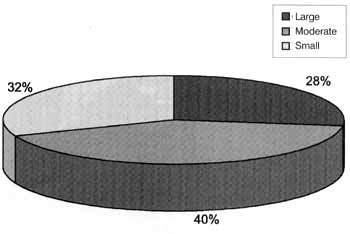
Graph 1 presents distribution of size of adenoids obtained by nasal fiberoptic examination: 28% (17 cases) of large adenoids (Figure 3); 40% (24 cases) of moderate adenoids, and 32% (19 cases) of small adenoids.
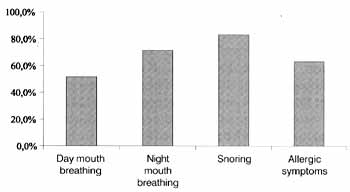
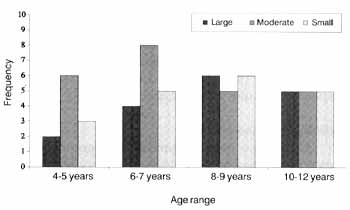
Graph 2 presents the predominant symptoms collected from the anamnesis of the studied patients. It was observed that in 83.3% (n = 50) snoring was the most frequent complaint in the studied group. In the age group from 4 to 7 years, there was predominance of moderate sized adenoids. From 10 to 12 years, no significant alterations were noticed in adenoid size. Small sized adenoids were more common in the age range up to 9 years. In the present study, moderate sized adenoids were predominant.
The endoscopic examination revealed 8 cases of significant atrophy of the posterior region of inferior turbinate (13.3%) and in 4 cases there was posterior septal deviation (6.6%) associated with moderate sized adenoids, not identified by the radiological examination.
DISCUSSION
Adenoid is an organ situated at a critical anatomical position on the roof of the nasopharynx and it presents an important role in the diseases of upper respiratory tract in children. Adenoid hyperplasia is considered a casual factor of otitis media with effusion, nasal obstruction, snoring, rhinosinusitis, sleep apnea and facial development disorders24.
Graph 1. Distribution (%) of the size of adenoid hyperplasia according to endoscopy of studied patients.
Graph 2. Predominant symptoms presented by 4-12 year-old patients in the studied group.
Graph 3. Size of adenoid according to age group of studied patients.
Adenoidectomy is one of the most frequent surgeries performed in children, and it is highly effective if well indicated. Wang et al. (1995)24 referred that adenoidectomy improves nasal obstruction in 77.2% of the children with adenoid hyperplasia, and snoring is suppressed in 89% of the surgery. Despite the consensus about its benefits, much has been said about diagnosis. Exact assessments of size of adenoids and its relation with the posterior nasal space (such as the posterior portion of inferior nasal turbinate or the nasal septum), are hardly ever clinically obtained.
Various complementary tests have been conducted for years in order to diagnose adenoid hyperplasia, including adenoid tissue shadow in lateral paranasal sinuses x-ray observed by Mignon in 189818. Among other more current possibilities deemed useful by the authors, there is acoustic rhinometry. However, none of the methods provides direct visualization of adenoid for appropriate evaluation of size, shape and relation with the other nasal structures and nasopharynx, as provided by nasal fiberoptic examination.
Enlarged pharyngeal tonsil is a globular three-dimensional structure, which moves towards the choanas from the posterior wall and roof of the nasopharynx, leading to partial or total obstruction. This concept is different in the radiological interpretation, which is based on a static situation9.
Cohen et al. (1992)8 published a study correlating lateral paranasal sinuses x-ray and size of adenoid. They concluded that radiological examination is the most appropriate pre-operative examination for children considered to adenoidectomy. However, they acknowledged the limitations of the test and found poor correlation between x-ray and operative observations (Pearson coefficient: 0.34).
Wang et al. (1997)23 correlated existence of adenoid hypertrophy in lateral paranasal sinuses x-ray in 88% of the cases submitted to nasal endoscopy. In 26%, however, the radiological examination failed to confirm the hypertrophy of the adenoid tissue when compared to the endoscopy.
Failures in radiological examinations are due to a number of factors:
The x-ray is limited because it provides only two-dimensional information about the nasopharynx, which is an anatomical three-dimensional structure4.
small head rotation movements during the radiological examination may generate changes in the distances between the structures involved, used to define the degree of obstruction.
contrast radiological studies of nasopharynx clearly demonstrated that the nasopharynx is a dynamic structure with contractile properties8: the soft palate moves during breathing, swallowing and when the mouth is opened. Under the circumstances, when the palate is elevated, it may strike as if it were an obstruction.
especially when the child is crying, the retropharyngeal wall will form an anterior bulging, producing a temporary enlargement of soft tissues in the nasopharynx, which causes reduction of the palatal air space. If in special situations, such as recurrent adenoids or presence of anatomical variations, the adenoid that is positioned superiorly to the nasopharynx may project into the choanae. Lateral x-ray will show absence of obstruction in the rhinopharyngeal space, and we may mistake "choanal adenoid" for posterior portion of the inferior turbinate 26. Pearl and Manoukian (1994)22, in a group of 33 adenoidectomies, found 31 patients (9.4%) with adenoid tissue extended from the. nasopharynx into the choanae and posterior nasal cavities (choanal adenoid).
The option for the method advocated by Cohen and Konak (1984)7, used in the present study, correlates size of nasopharynx and adenoid. It is a simple method, free of complicated calculations and measures that require good quality and standard of radiography. Therefore, it is a safe and quick method, enabling interpretation of radiological examinations used with scientific purposes.
Adenoids seem to enlarge quickly between 3 and 5 years of age, which may explain the facility to conduct the nasal fiberoptic examination, as described by the literature and confirmed by the present study5,25. The minimal age range was 4 years, which facilitated the conduction of detailed examination and guaranteed the child's cooperation. We should also point out that these patients had already been investigated with paranasal sinuses x-rays, in some cases more than one year before, and there was no obstructive adenoids.
Wang et al., 199723 studied 667 children aged 2 to 7 years with flexible nasal fiberoptic examination and found large sized adenoids in 45.5% of them; moderate size in 23.2 % and small size in 31.2%. However, they selected patients based on clinical picture (chronic nasal obstruction and snoring). This condition hinders the comparison with the results found by the present study, which considered symptomatology and normal paranasal sinuses x-ray.
Endo et al. (1997)11 evaluated 55 children aged one week to two years presenting nasal obstruction and no response to clinical treatment. They were all submitted to nasal fiberoptic examination under general anesthesia and one of the limitations found was the younger age of patients. The difference in the age range of studied patients prevented us from comparing to our results. Endo et al. presented nasal mucosa edema as the main cause of obstruction (34.5%) and adenoid tissue blocking the choanae (16%). The other causes were choana atresia, choanal stenosis, cyst of nasolachrymal duct, septal deviation and turbinate hypertrophy.
Chami (1998)6, in his study of nasal fiberoptic and radiological examinations of patients with pharyngeal tonsil hyperplasia, using adenoid/nasopharynx ratio described by Fujioka in 197912, noticed that night snoring was the main symptom in the sample (100%). Mouth breathing was present in 65.2%. The findings of the present study, using nasal fiberoptic examination, showed approximately 2/3 of the cases with adenoid hyperplasia as the main cause of nasal obstruction. Based on that, we developed an objective criteria for assessment of adenoid size and degree of nasopharynx obstruction, indicating surgical treatment as the most suitable in the majority of the cases.
CONCLUSIONS
Diagnostic investigation of chronic nasal obstruction in children may be initially directed by clinical and radiological data.
In patients in whom clinical data point towards chronic nasal obstruction and paranasal sinuses x-ray seem to be insufficient to confirm the cause of the obstruction, nasal fiberoptic examination becomes essential to elucidate diagnosis, safely leading to surgical treatment.
REFERENCES
1. BRODSKY, L. - Modern Assessment of Tonsils and Adenoids. Pediatrics Clinics of North America. 36 (6): 1551-1569, 1989.
2. BRODSKY, L. & KOCH, J. R. - Anatomic Correlates of Normal and Diseased Adenoids in Children. Laryngoscope. 102: 1268-1274, 1992.
3. BUTUGAN, O.; CAHALI, B. M.; MURAKAMI, M. S.; IKINO, C. M. Y; D'ANTONIO, W E. E A.; MEDEIROS, I. R. T M.; SANTORO, E. E; VOGELS, R. L.; SENNES, L. U. - Tumores nasais na Infância. Revista Brasileira de Otorrinolaringologia. 65: 20 - 24, 1999.
4. CASTRO JR., N. P; TACIRO, E. K.; TANAKA, C. Endoscopia Nasossinusal. Acta Awho. Vol. XI, (1): 3-7, 1993.
5. CAUWENBERG, P B. van; BELUSSI, L.; MAW A. R.; PARADISE, J. L.; SOLOW B. - The Adenoid as a key factor in upper airway infections. International Journal of Pediatric Otorhinolaryngology. 32 (suppl): S71- S80, 1995.
6. CHAMI, F. A. I. - Avaliação nasofibroscópica e radiológica de pacientes com hiperplasia da amígdala faríngea. Revista Brasileira de Medicina-ORL. 5 (4): 118125, 1998.
7. COHEN, D. & KONAK, S. - The evaluation of radiographs of the nasopharynx. Clin. Otolaryngology. 10: 73-78, 1985.
8. COHEN, L. M.; KOLTAI, E J.; SCOTT, J. R. - Lateral Cervical Radiographs and Adenoid Size: Do They Correlate? E. N. T. Journal. 71 (12 ): 638-642, 1992.
9. DEMAIN, J. G. & GETZ, D. W - Pediatric Adenoidal Hypertrophy and Nasal Airway Obstruction: Reduction with Aqueous Nasal Beclomethasone. Pediatrics. 95 (3): 355-364, 1995.
10. DEUTSCH, E. S. - Tonsilectomia a Adenoidectomia. Clínicas Pediátricas da América do Norte. 6: 1263-1282, 1996.
11. ENDO, L. H.; SAKANO, E.; MARRA, B. M. - Obstrução Nasal na Infância: Importância do diagnóstico endoscópico. A Folha Médica - Cadernos de ORL. 115 (1): 12, 1997.
12. FUJIOKA, M.; YOUNG, L. W; GIRDANY, B. R. Radiographic Evaluation of Adenoidal Size in Children: Adenoidal-Nasopharyngeal Ratio. AJR. 133: 401-404, 1979.
13. HIBBERT, J. - The current status of adenoidectomy: a survey among otolaryngologists. Clinical Otolaryngology. 2: 239-247, 1997.
14. HIBBERT, J.; STELL, E M.; WRIGHT, A. - Value of physical signs in the diagnosis of enlarged adenoids. Clinical Otolaryngology. 5: 191-194, 1980.
15. HIBBERT, J. & ATELL, PM.- A radiological study of the adenoid in normal children. Clinical Otolaryngology. 4: 321-327, 1979.
16. JEANS, W D.; FERNANDO, D. C. J.; MAW A. R. - How should Adenoidal Enlargement be Measured? A Radiological Study Based on Inter-observer Agreement. Clin. Radiology. 32: 337-340, 1987.
17. JOHANNESSON, S. - Roentgenologic Investigation of the Nasopharyngeal Tonsil in Children of different Ages. Acta Radiologica Diagnosis. 7: 299-304, 1968.
18. JOHNSON, A. E; MURRAY, A. J. M.; MARAN, A. G. D. Errors in the assessment of nasopharyngeal airway by radiography. The Journal otaryngology and Otology. 97: 1017-1026, 1983.
19. KAMEL, R. H. & ISHAY, E. A. Enlarged adenoid and adenoidectomy in adults: Endoscopic approach and histopathological study. The Journal of Laryngology and Otology. 104: 965-967, 1990.
20. MAW A. R.; JEANS, W D.; FERNANDO, D. C. J. - Inter-observer variability in the clinical and radiological assessment of adenoid size, and the correlation with adenoid volume. Clin. Otolaryngol. 6: 318-322, 1981.
21. PARADISE, J. L.; BERNARD, B. S.; COLBORN, D. K.; JANOSKY J. E. - Assessment of Adenoidal Obstruction in Children = Clinical Signs Versus Roentgenographic Findings. Pediatrics. 01 (6): 979 - 986, 1998.
22. PEARL, A. J. & MANOUKIAN, J. J. - Adenoidectomy: indirect visualization of choanal adenoids. Journal Otolaryngol. 23 (3): 221-224, 1994.
23. WANG, D. Y; BERNHEIM, N.; KAUFMAN, L.; CLEMENT, E - Assessment of adenoid size in children by fiberoptic examination. Clin. Otolaryngol. 22: 172-177, 1997.
24. WANG, D. Y; CLEMENT, E A. R.; KAUFMAN, L.; DERDE, M. P - Chronic nasal obstruction in children. A fiberscopics study. Rhinology. 33: 4-6, 1995.
25. WORMALD, E J. & PRESCOTT, C. A. J. - Adenoids: Comparison of radiological assessment methods with clinical and endoscopic findings. The Journal of Laryngology and Otology. 106: 342 - 344, 1992.
26. YANAGISAWA, E, & YANAGISAWA, K. - Endoscopic View of Adenoids. ENT. Journal. 73 (2): 74-75, 1994.
* Master in Otorhinolaryngology, Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo (FMRP-USP).
**Assistant Professor, Ph.D. in Otorhinolaryngology, FMRP-USE
*** Postgraduate in Otorhinolaryngology, FMRP-USE
Master Dissertation presented and approved at FMRP USE
Address correspondence to: Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FMRPUSP).
Avenida Bandeirantes, 3900-14049-900 Ribeirão Preto/ SP.
Article submitted on April 17, 2000. Article accepted on April 27, 2001.


Print: ![]()