

Year: 2001 Vol. 67 Ed. 2 - (11º)
Artigos Originais
Pages: 213 to 218
Distortion Products Evoked Otoacoustic Emissions Measurements in Noise Induced Hearing Loss Patients.
Author(s):
Gilberto Gattaz*,
Silvia R. G. Wazen**.
Keywords: distortion products, noise induced hearing loss
Abstract:
Introduction: Noise is one of the most frequent problems spotted out in industrial workplaces. High-intensity noise or long-term exposition to noisy areas cause definite reduction of the hearing sensitivity due to the damage in the internal ear sensorial organs. Concerning the occupational health field, the most used procedure in the diagnosis of hearing loss in the pure tonal audiometry. Nevertheles, the diagnosis of noise-induced hearing loss can only be established by means of a series of procedures involving clinic anamneses, occupational background, physical exam, hearing admission evaluation, as well as monitoring the individual's hearing throughout his professional life. Other complementary tests such as impedance measurements, speech psycho-acoustic tests together with evoked otoacoustic emissions (EOAE) should be used, if needed. Considering that the EOAE as well as the pure tone audiometry tests do have distinct methodological patterns and that the EOAE does not really quantify the hearing loss, the purpose of the present paper is to analyse the results obtained in the pure tone audiometry, as well as in the EOAE by distortion product (EOAPD), thus setting comparison parameters between the two exams on individuals exposed to occupational noise. Study design: Clinical prospective. Material and method: 31 people have been analysed, all of them belonging to the male sex and aging between 31 to 63, who Nave been exposed to noise for a period longer than 10 years. Out of these, 59 ears have been evaluated by means of pure tone audiometry, impedance measurements and EOAPD. Results: The results show that there was a significant correlation between audiometry and EOAPD, mainly in the high frequencies.
![]()
INTRODUCTION
Development of society has contributed to the production of noise at higher and higher levels. Noise is mechanical vibration that prolongs through the air, and as it reaches the ear, produces the hearing sensation. Noise is one of the most commonly identified problem in industrial workplace (Nepomuceno, 1979).
Noise affects people that work in industrial settings, causing irritability, reduction of efficacy at work, physiological alterations of cardiac rhythm and blood pressure, and psychological disorders.
It is considered that noise affects people physical, psychological and socially and it may also cause fatigue, hearing impairment and interference in communication.
Loud noise or prolonged exposure in noisy areas may cause permanent reduction of hearing sensitivity, due to damage to inner ear sensorial mechanisms.
Seligman (1997) reported that based on the category that described permanent changes in thresholds, we may divide the symptomatology of noise-induced hearing loss (NIHL) in two large groups: auditory symptoms (hearing loss, tinnitus, difficulty to understand speech and others) and non-auditory symptoms (communication disorders, sleep alterations, neurological, vestibular, digestive and behavioral disorders).
In the area of Occupational Health, the procedure used to diagnose hearing loss is pure tone audiometry. Pure tone audiometry and search of each frequency threshold is the test that complies the best with the needs of careful NIHL investigation, provided that some quality technical principles are followed.
The importance of audiometry to identify NIHL is great. However, it should not be overestimated and used as the only single tool for diagnosis. In addition to the imprecision deriving from the subjectivity of the method, such as motivation, level of intelligence, level of language, education, willingness to cooperate and concentration of subjects (Price, 1978), the test does not detect problems that arise before the hearing loss, such as recruitment and tinnitus (Costa apud Michael and Bienvenue, 1976). It is a test subject to errors because it requires previous knowledge about anatomy and physiology, concepts of generation and transmission of sound, and it depends on equipment.
The diagnosis of NIHL may only be defined based on a set of procedures that involves clinical anamnesis, occupational history, physical exam, admission hearing test and monitoring of subject's hearing throughout his or her occupational life. If so required, complementary tests may be used, such as immitanciometry, speech psychoacoustic tests and evoked otoacoustic emissions (OAE).
Taking into account that OAE and pure tone audiometry are tests with distinct measurement patterns and that OAE does not quantify hearing loss, the purpose of the present study was to analyze the results obtained from pure tone audiometry and OAE, producing parameters for comparison between the two methods in subjects exposed to industrial noise.
LITERATURE REVIEW
A. Otoacoustnc emissions
Otoacoustic emissions were first observed by the English professor David Kemp, in 1978, who defined them as release of sound energy originated from the cochlea that is propagated by the middle ear until it reaches the external auditory canal. Kemp showed that OAE are present in all functionally normal ears and are not detected if thresholds are above 20-30dB.
Carnicelli apud Hood et al., 1996, mentioned that the origin of otoacoustic emissions is related to mechanical movement or electromobility of external hair cells, controlled by auditory efferent pathways through the olivocochlear system.
The recording of evoked otoacoustic emissions is the latest method to detect cochlear hearing alterations. It consists of an objective method that is relatively simple, fast, non-invasive, that does not require electrodes - capture of sound is done by a microphone placed in the external auditory canal - and it may be performed at any age range (Kemp et al., 1990).
Gattaz apud Koller et al. (1991) reported that the study of OAE provides a new opportunity to assess fatigue and early auditory disorders, noticing a reduction of amplitudes or even absence of response, depending on duration and intensity of noise exposure.
It has been described that otoacoustic emissions may also be employed in hearing conversation programs in order to detect early hearing impairment caused by occupation exposure (Hotz et al., 1993; Engdahl et al., 1996).
One of the important aspects of OAE is the possibility of studying the mechanical aspects of cochlear function in a non-invasive and objective way, regardless of the potential of the neural action. Therefore, clinically objective information may be obtained about neural elements of cochlea. Most of the hearing losses, such as noise-induced and hereditary affections, originate from these elements. The other objective methods currently in use in daily audiological routine do not measure directly the responses of these elements.
It has been demonstrated that short noise exposures result in decrease of OAE amplitude, altering the composition of frequencies and increasing thresholds (Ros'si et al., 1991; Avan et al., 1993).
According to Probst et al., (1993), OAE are considered by the authors as the ideal test to monitor noise-inducedcochlear alterations, owing to its frequency specificity and the possibility of testing frequencies from 4 to 8kHz.
B. Noise induced hearing loss (NIHL)
Skellett apud Saunders et al. (1985, 1991) described that exposure to sounds induce changes in the structure and function of auditory pathways. The changes depend on duration, intensity and temporal pattern of exposure. Alterations of auditory function after very intense sound levels may be attributed to mechanical changes of cochlear structure.
Studies conducted in the field about hearing loss in industrial workplaces, as well as lab studies, identified four important factors that contribute to the risk of noise and hearing. They are: (a) total sound level, measured in dB; (b) spectral distribution (distribution of sound energy by frequency), (c) duration and distribution of noise (sound exposure during a normal work day); and (d) cumulative exposure in days, weeks or years (Academy of Otolaryngology - Head and Neck Surgery, 1988).
The risk of noise damage is higher as a result of increase in noise level or increase in duration of exposure, but it also depends on the characteristics of sound. In addition, sensitivity to noise is an individual element.
Audiometric exams are the only possible way to detect noise susceptibility of subjects; by comparing results of periodical exams, we may estimate if an employee is being affected by a noisy environment.
Among the alterations that comprise the clinical picture of the occupational disease, higher auditory thresholds are detected by audiometry, tracings share relatively constant and well defined characteristics and enable differential diagnosis with other hearing pathologies.
Comitê Nacional de Ruído a Conservação Auditiva - National Committee for Noise and Hearing Preservation (1994) defined that occupation NIHL, differently from acoustic trauma, is a gradual reduction of hearing acuity, caused by continuous exposure to high levels of noise. It is characteristically a sensorineural loss, because of the damage caused to Corti's organ cells. The process of NIHL involves not only sensorial cells but also supporting cells, nerve fibers and vascular supply (Henderson and Hamernik, 1995).
Once present, NIHL is irreversible and almost always similar bilaterally. The hearing loss rarely progresses into profound loss, because it seldom goes below 40dBHL in low frequencies and 75dBHL in high frequencies.
Initially and predominantly it is manifested in the high frequencies 6, 4, or 3kHz, and as the damage progresses, it extends to frequencies 8, 2, 1, 0.5 and 0.25 kHz, which take longer to be affected. It normally reaches the maximum for frequencies 3, 4, and 6kHz within the first 5 to 10 years of exposure, under stable noise conditions. Once interruoted the exposure, there should be no further progression of loss.
Unfortunately, NIHL is followed by a constellation of hearing deficits, such as loudness recruitment (Henderson and Salvi apud Hickling, 1967), tinnitus (Loeb and Smith, 1967), poor frequency selectivity, temporal processing and poor speech perception (Leshowitz and Lindstrom, 1977; Wightman et al., 1977).
Melnick (1978) emphasized that "the range of severity of losses may be due to differences both of susceptibility of subjects (gender, concomitant exposure to other agents, pre-existent hearing loss, age, etc) and physical characteristics of noise (spectrum of frequencies, intensity, etc.).
Studies suggested that NIHL may be aggravated by simultaneous exposure to intense noises and other agents, such as chemicals and vibration. Similarly, the worker that takes ototoxic drugs or has any other diseases has higher susceptibility to noise (Comite Nacional de Ruído e Conservação Auditiva, 1994).
MATERIAL AND METHOD
The study included analysis of audiological tests of 31 male subjects ranging in age from 31 to 63 years, with history of noise exposure longer than 10 years. Among them, 59 ears were evaluated using pure tone audiometry, speech discrimination, acoustic immitance and DPOAE, and all procedures were conducted after auditory rest. We excluded subjects with conductive loss or sequelae of otitis media at otoscopic assessment, tympanometry and search for acoustic reflex. On the other hand, we did not exclude exams that presented other causes of associated hearing losses.
It is important to point out that even audiometric tests with inconsistent and incompatible responses with speech discrimination were considered in the study.
The spectrum of frequencies studied both for audiometry and otoacoustic emissions included frequencies 1k, 2k, 3k, 4k, 6k and 8 kHz. Frequencies 0.25 and 0.5 kHz were not included in this study, since they are rarely affected in NIHL and in order to prevent difficulties to capture these frequencies with distortion product.
The devices used to conduct pure tone audiometry and immitanciometry were Kamplex AD 27 and Kamplex AZSR, respectively. To obtain DPOAE we used Madsen Celesta 503 in sound treated booth. All devices belonged to Instituto de Otorrinolaringologia de São Paulo - Hospital dos Defeitos da Face.
Amplitude of DPOAE was measured by different combinations of f1 and f2. The ratio fl/f2 was maintained constant in 1.22. Both tones were applied simultaneously at similar 70dBSPL intensity
Figure 1. Porcentage of altered responses.
Figure 2. Individual responses.
RESULTS AND DISCUSSION
First of all, we should point of that interpretation of results followed a standardization pattern, according to the parameters provided by the equipment's software.
The spectrum of frequencies considered, both for audiometry and DPOAE involved frequencies 1k, 2k, 3k, 4k, 6k and 8 kHz. Frequencies 0.25 K and 0.5 kHz were not included in the study because they are rarely affected by NIHL and sometimes they are difficult to capture with distortion product.
We compared the percentage of altered responses in both exams in the respective frequencies, considering pure tone thresholds higher than 25dBHL for pure tone audiometry and responses below the normal range for distortion product (Figure 1).
We observed good correlation between responses provided in both tests. We recorded the highest percentage indexes in frequencies 4 and 6kHz, that is 91.1% and 97.3%, respectively, showing what is characteristic of NIHL, according to the Comite Nacional de Ruído a Conservação Auditiva (1994).
By comparing isolated percentage of responses altered in each frequency, if pure tone thresholds were higher than 25dBHL in audiometry and responses below normal range in distortion product, we observed the highest percentage indexes of pure tone in 4 and 6 kHz (4KAUD and 6K AUD) and recording of altered DPOAE in 3 and 4 kHz (3K DP and 4K DP), showing reduction in the frequency range, which is evident in NIHL (Figure 2).
As to the two tests conducted, we should consider that there is not an exact coincidence of reduction in the same frequency, since they are different methods from a physiological standpoint. In audiometry, the response provided is subjective and behavioral, elicited by sound stimuli, and it depends on auditory processing. Otoacoustic emissions are an exclusively cochlear physiological phenomenon of pre-synaptic nature, and distortion product is recorded in a frequency (2f1-f2) different from the frequency that generated it (fl and f2). For example, if we analyze DPOAE at frequency of 3 kHz, frequencies of stimuli fl and f2 will be, respectively: fl = 2,734 Hz and f2 = 3,348 Hz, and distortion product will be recorded at (2f1-f2) = 2,126 Hz).
Figure 3 correlates normal results obtained with audiometry and altered results obtained with DPOAE. We noticed an incidence below 30% in all frequencies analyzed in the study.
Suckfull et al. (1996) reported that one of the factors involved in the variation of amplitude of DPOAE is status of middle ear. Even minor pressure differences of middle ear affect transmission of DPOAE and lead to a significant reduction of DPOAE.
We should highlight that the studied population presented normal otoscopy and immitanciometry.
Weinstein apud Etholm and Belal (1974) and Covell (1952) raised the issue of subjects' age. Although alterations of hearing system related to age are more marked in the inner ear and central auditory pathways, they are susceptible to alterations of external and middle ear structures. Tympanic membrane becomes more rigid, articulation of ossicles suffer a process of progressive calcification and tensor tympani and stapedial muscles become atrophic as a result of aging, which could interfere in the recording of DPOAE. These findings could justify the results previously reported, represented by normal audiometry and altered DPOAE.
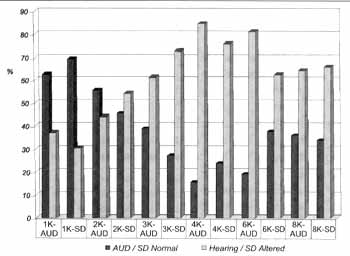
Figure 3. Comparison of standard deviation in normal and abnormal audiometry.
On the other hand, we may argue that these alterations of DPOAE in individuals with normal audiometry may be a sign of cochlear dysfunction or deficit, that is, since we capture abnormal DPOAE and taking into account that it is a highly sensitive test, we may suppose that the tracings represent the indication of an early stage of noise induced hearing dysfunction (Hall apud Desai et al., 1999).
Upon comparing altered results of audiometry and normal results of DPOAE (Figure 3), indexes of 64.3%, 54.5% and 35 % in frequencies 4, 6 and 8 kHz, respectively, were observed. These results may be explained by the fact that it is quite common to find inconsistent responses obtained for audiometric pure tone thresholds, because some patients are not willing to cooperate or may be malingering.
CONCLUSIONS
In view of the results obtained with the present study, we concluded that DPOAE showed significant correlation when compared with pure tone audiometry, especially in high frequencies.
Therefore, because of its unique characteristics and properties, and thanks to its high frequency specificity DPOAE is an additional instrument to diagnose hearing loss induced by noise and to identify minimal functional alterations of the peripheral hearing system, even before a hearing loss, which may provide early detection of auditor3 damage caused by occupational exposure.
Currently, audiometry is considered an important procedure to monitor NIHL. However, owing to the increasing number of legal proceedings, the responsibility upon the physician or audiologist to interpret the exam is highly significant.
In many occasions, professionals are faced with difficulties during conduction of audiometry, because it is a subjective test, involving social, cultural, environmental and biological aspects, which in many situations requires attention and concentration by the tested subject.
Since there is the likelihood of having variation of audiometric results or even inconsistent pure tone thresholds because of subjects who do not collaborate or try to malinger, it is desirable to have objective tests in order to monitor cochlear alterations induced by noise to support professionals that work in the area of occupational health.
We should also point out that more studies should be conducted in this area in order to standardize the recording of distortion product and better monitor the status of the cochlear epithelium in subjects exposed to occupational noise.
REFERENCES
ALMEIDA, C. I. S. - Diagnóstico diferencial da disacusia neuro-sensorial pelo ruído. In: Nudelmann, Costa, Seligman & Ibanez, PAIR.; 1.ed. Porto Alegre: Bagaggem. 1997, 181-88.
BEVILACQUA, C. M.; FERREIRA, D. M.; SILVA, S. C.; MAYRINK, E. C. - Os Efeitos do Ruído na Audição: Revista de Acústica a Vibrações, 12: 30-43, 1993.
CARNICELLI, F. V M. - O use das emissões otoacústicas no diagnóstico a prevenção da perda auditiva induzida pelo ruído. In: Nudelmann, Costa, Seligman & Ibanez, PAIR.; 1.ed. Porto Alegre: Bagaggem. 1997, 237-46.
COMITE NACIONAL DE RUÍDO E CONSERVAÇÃO AUDITIVA - Perda Auditiva Induzida pelo Ruído Relacionada ao Trabalho. JBM., Vol. 67: 156-7, 1994.
COSTA, A. E. - Classificação a Quantificação das Perdas Auditivas em Audiometrias Industriais. Revista Brasileira de Saúde Ocupacional., 16: 35-8, 1988.
FILHO, L. O.; CARLOS, C. R. - Emiss6es Otoacústicas. In: Filho, Tratado de Fonoaudiologia, 1.ed. São Paulo: Roca. 1997, 221-38.
GATTAZ, G. - Registro das Emissões Otoacústicas Evocadas e Sua Aplicação Clínica na Audiologia Infantil. In: Caldas & Sih, Otologia a Audiologia em Pediatria., 1.ed. São Paulo: Revinter. 1999, 211-15.
GATTAZ, G.; RUGGIERI, M.; BOGAR, E - Estudo das Emissões Otoacústicas Evocadas em Adultos Jovens Audiologicamente Normais: Rev. Bras. Otorrinolaringol., 60 (1): 15-8 ,1994.
HALL, J. W - Clinical Applications of Otoacoustic Emissions in Adults. In: Hall, J. W III., Handbook of Otoacoustic Emissions, San Diego: Singular. 2000, 481-541.
HARRIS, E F.; PROBST, R. - Otoacoustic Emissions and Audiometric Outcomes. In: Robinette & Glattke, Otoacoustic Emissions: Clinical Applications., 1.ed. New York: Thieme. 1997, 151-80.
HENDERSON, D.; HAMERNIK, E R. - Biologic Bases of Noise Induced Hearing Loss. Occupational Medicine. State of the Art Reviews., 10: 513-34, 1995.
HENDERSON, D.; SALVI J. R. - Effects of Noise Exposure on the Auditory Functions. Scandinavian Audiology., 27: 6373, 1998.
HIMBERLEY, E B.; BROWN, K. D.; ALLEN, B. J. - Distortion Product Emissions and Sensorineural Hearing Loss. In: Robinette & Glattke, Otoacoustic Emissions: Clinical Applications., 1.ed. New York: Thieme. 1997, 181-204.
KOWALSKA, S. M.; KOTYLO, E; HENDLER, B. - Comparing changes in transient-evoked otoacoustic emission and puretone audiometry following short exposure to industrial noise. Noise & Health., 2: 50-57,1999.
LAZMAR, A. - Diagnóstico da doença professional induzida pelo ruído. In: Nudelmann, Costa, Seligman & Ibanez, PAIR.; l.ed. Porto Alegre. Bagaggem. 1997, 153-62.
LONSBURY MARTIN, L. B.; MARTIN, K. G.; WHITEHEAD, L. M. - Distortion Product Otoacoustic Emissions. In: Robinette & Glattke, Otoacoustic Emissions: Clinical Applications., 1.ed. New York. Thieme. 1997, 83-109.
MELNICK, W - Saúde Auditiva do Trabalhador. In: Katz, J., Tratado de Audiologia Clinica., 4.ed. São Paulo. Manole. 1999, 529-47.
NEPOMUCENO, X. L. - Medidas Técnicas para análise, avaliação a controle do barulho na industria. Revista Brasileira de Saúde Ocupacional., 7: 06-23, 1979.
NORTON, J. S.; STOVER J. L. - Emissões Otoacústicas: Um Novo Instrumento Clinico. In: Katz, J., Tratado de Audiologia Clínica., 4.ed. São Paulo. Manole. 1999, 444-60.
PIALARISSI, R. E; GATTAZ, G. - Emissões Otoacústicas: Conceitos Básicos a Aplicações Clinicas. Arq. Fund. Otorrino-laringologica., 1 (2): 41-3, 1997.
SELIGMAN, J. - Sintomas a sinais na PAIR. In: Nudelmann, Costa, Seligman & Ibanez, PAIR., l.ed. Porto Alegre: Bagaggem. 1997, 143-52.
SUCKFfTLL, M.; SCHNEEWEIB, S.; DREHER. A.; et al. Evaluation of TEOAE and DPOAE Measurements for the Assessment of Auditory Thresholds in Sensorineural Hearing Loss. Acta Otolaryngology., 116: 528-33, 1996.
WEINSTEIN, B. E. - Presbiacusia. In: Katz, J., Tratado de Audiologia Clinica., 4.ed. São Paulo. Manole. 1999, 562-77.
WHITE, R. D.; BOETTCHER, A. F.; MILES, R. L.; et al. Effectiveness of intermittent and continuous acoustic stimulation in preventing noise-induced hearing and hair cell loss. J. Acous. Soc. Am., 103 (3): 1566-72, 1998.
* Otorhinolaryngologist. Ph.D., Assistant Professor of Faculdade de Fonoaudiologia - PUC /SP
** Speech and Hearing Therapist, Master studies under course at the Post-Graduation Course on Disorders of Communication PUC /SP
Study conducted at Instituto de Otorrinolaringologia de São Paulo - Setor de Otorrinolaringologia - Hospital dos Defeitos da Face.
Address for correspondence: Dr. Gilberto Gattaz - Rua Cincinato Braga, 59 - 5° andar, cjto. D-1 - 01333-011 São Paulo /SP
Tel: (55 11) 288-4186 - Fax: (55 11) 3887-9913 - E-mail: sgattaz@ibm.net
Article submitted on October 18, 2000. Article accepted on January 15, 2001.
Print: ![]()