

Year: 2001 Vol. 67 Ed. 2 - (8º)
Artigos Originais
Pages: 189 to 194
Eustachian Tube Function x Nasopharyngoscopy: A Comparative Study Among the Evaluation Procedures of the Eustachian Tube.
Author(s):
Isabella M. C. Silva*,
Mariza R. Feniman**,
José C. Jorge***.
Keywords: auditory tube, nasopharyngoscopy, Eustachian tube function, tympanic membrane perforation, Eustachian tube
Abstract:
Introduction: The good performance of the auditory tube is necessary for a healthy and functional tympanum cavity. The precise evaluation of its performance during the audiology practice allows a prediction of the success of procedures used by the professional in order to improve alterations in middle ear. Objective: The aim of this research is to evaluate the function of the auditory tube in individuals with tympanum perforation, through the use of an imitanciometer, to visualize the conduct of auditory tube during rest periods and during swallowing, through the nasopharyngoscopy, and to report results obtained by both procedures. Study design: Clinical prospective. Material and method: 40 ears of 31 individuals with bilateral and unilateral tympanum membranes perforations were evaluated. The evaluation was a research test of the auditory tube function, using imitanciometer and nasopharyngoscopy. Results: A closed ill-functioning auditory tube was the most frequent finding reported during auditory tube function research (62,5%), followed by hypofunctioning auditory tube (20%), opened ill-functioning auditory tube (12,5%) and functioning auditory tube (5%), all of which were found by the imitanciometer, in order to examine the auditory tube permeability. With regard to the behavior of auditory tube during rest periods and during swallowing, the most frequent visualization on the nasofiringoscopy was closed an rest and open at swallowing (55%), followed by open/open (30%), and by closed/closed and no visualization (both with 7, 5%). Conclusion: The findings did not allow a direct confrontation between the results of both procedures, due to the different approaches of each one. The information provided complement clinical exam and aid the choice of the most appropriate procedure for each individual.
![]()
INTRODUCTION
The eustachian tube, the canal that communicate the middle ear with the nasal portion of the pharynx, ha; two main parts13. The fibrocartilaginous portion of the tube ends in the nasal portion of pharynx, forming the torus tubarius and amounts to the two anterior thirds of the eustachian tube. The posterior third is the bone portion of the eustachian tube that communicates directly wits epytympanic cavity, though the tympanic tube orifice. It; total average length varies from 31 to 38mm. In adults, it is located at 45° from the horizontal plan and in children, this angle is smaller, as low as 10° in newborns3.
The eustachian tube has many functions that aim at establishing a good performance of middle ear system - mastoid cells - eustachian tube - nasal portion of pharynx It remains closed during rest, protecting the middle ear from the flow of secretions and microorganisms from the rhinopharynx, from sounds and pressure variations that take place all the time in the pharynx, such as breathing, cough; dry or nose blowing. The opening is intermittent, by the action of the tensor palatini muscle, in order to let pass air from the nasopharynx into the middle ear. It enables equalization of pressures from the tympanic cavity and the environment, plus the entry of oxygen that had been used by the mucosa cells of middle ear2,5,12,14.
There is also the role of drainage of ear secretions to the nasal portion of pharynx5. The accumulation of secretion in the middle ear and the action of palatini tensor muscle promote change in pressure, which result in clearance of part of the secretion that is in there8. Malfunctioning of palatini tensor muscle affects the function of the eustachian tube, and consequently, the tympanic cavity.
There are still possible alterations of eustachian tube functions, such as an open and obstructed tube5. The open tube brings infections to the middle ear because of the flow of pharyngeal secretions. The obstruction may be functional because of muscle incapacity to open the lumen or to break with the abnormal forces that keep it closed. It may be a mechanical obstruction, due to external factors, such as adenoid and tumors, or intrinsic factors, such as infections, inflammations, allergy and congenital stenosis1. Malfunctioning of eustachian tube, in case of obstruction, promotes hypoventilation of tympanic cavity that causes increase of mucus and negative pressure, by air absorption, causing secretory, serous and chronic otitis, primary cholesteatomas and tympanic membrane atelectasia1,5.
A frequent factor that may affect the good performance of eustachian tube is the infection of upper airways7. In such cases, airflow through the eustachian tube decreases, favoring the creation of negative pressure in the middle ear.
A functioning eustachian tube is essential to have a healthy anti functioning tympanic membrane Precise evaluation of eustachian tube function in the clinical audiological practice aims at safely defining eustachian tube status in order to guarantee the success of any type of procedure used by the physician to improve the middle ear affection. There are a number of tests to accomplish that: Bortinick test, Toynbee maneuver, Valsalva test, forced response, tube auscultation, endoscopic tests, immitanciometry and inflation and deflation test, among other3,6,9.
Inflation and deflation test consists of introduction of positive and negative pressure, respectively, of 200dapa in ears with tympanic perforation, and ask the patient to drink water in small sips, swallow dryly, move the jaw or yawn, in order to cause the active opening of eustachian tube by contraction of palatini tensor muscle and equalize the pressure in the middle ear3. The deflation test, however, may cause collapse of eustachian tube because of the negative pressure, leading to no equalization of pressures. Some assessment protocols use only the introduction of positive pressure at 200dapa in the external acoustic canal sealed with a rubber tip11,15. We noticed that other studies showed less response variability when conducting the test with swallowing of water and authors stated that three swallowing movements are enough to reach the expected result. The results obtained from this test may bell:
closed eustachian tube: if there is no reduction of pressure in the tympanic cavity, showing poor functioning of the tube;
hypo-functioning eustachian tube: if there is a gradual reduction of pressure in the middle ear, without total elimination of pressure;
functioning eustachian tube: if there is gradual reduction up to zero, as displayed in the manometer;
ill-functioning eustachian tube: with permanent and pathological opening, if there is quick release of pressure in the middle ear.
It is believed that the prognosis of a functional surgery of tympanic membrane may be estimated based on the results of that testes.
Another way of assessing the status of the eustachian tube is the visualization of pharyngeal ostium by nasopharyngoscopy By means of endoscopy, conducted via transoral or transnasal in patients with or without tympanic perforation, we may visualize the structures, such as torus tubarius, veli palatini, orifice of the tube and cartilaginous portion, and the dynamic of these structures10,17. It has been said that it is not possible to evaluate eustachian tube status by nasopharyngoscopy3. There are reports of 3 different ways to define the structure of the pharyngeal orifice of eustachian tube10:
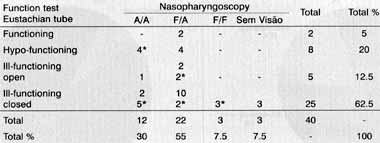
1. associated movement of soft palate and eustachian tube;TABLE 1 - Distribution of eustachian tube status observed in eustachian tube function test and nasopharyngoscopy of the participants in the study.
Key: A/A- Open eustachian tube at rest, mantained open during swallowing; F/A- Closed eustachian tube at rest and opening during swallowing; F/F - Closed eustachian tube at rest, maintained closed during swallowing; (*) Presence of secretion in eustachian tube and nasal nasopharynx; SEM VISAO - Eustachian tube could not be visualized because of hypertrophy of pharyngeal tonsil.
2. eustachian tube with no movement, remains open or closed, both at rest and during swallowing;
3. hyperplasia of soft palate, obstructing the lumen o the tube, especially in cases of cleft palate.
The same study concluded that there was n correlation among the results of the different eustachia tube functional tests.
The present study intended to assess the status of eustachian tube in patients with tympanic membrane perforation by investigating tube function using immitanciometer, visualization of eustachian tube at rest and during swallowing with nasopharyngoscopy and relate the results obtained with both exams.
MATERIAL AND METHOD
The sample of the present study was selected from the practice at Centro de Distúrbios da Audição, Linguagem e Audição (CEDALVI), Hospital de Reabilitação de Anomalias Craniofaciais (HRAC), at Universidade de São Paulo (USP), campus de Bauru: Thirty-one subjects participated in the study - all of them had uni or bilateral tympanic perforation, corresponding to 40 ears. The etiology of perforation was varied, including chronic otitis and mechanical trauma.
All subjects were submitted to ENT assessment, audiological tests and eustachian tube test in the perforated ear using the immitanciometer and nasopharyngoscopy.
The eustachian tube function test was conducted with the immitanciometer AZ7 Interacoustics. First, we placed the probe into the ear with the perforation followed by the introduction of 200dapa of positive pressure11,15. The patient was asked to swallow water three times. In each swallow, we observed the position of the display of the manometer, which indicated loss of pressure after swallowing. The results to this test followed the description reported by the literature11.
1. functioning eustachian tube: if there was gradual reduction of pressure injected in the tympanic cavity after each sip, the eustachian tube was working appropriately; after three swallowings, the pressure returned to zero;
2. hypo-functioning eustachian tube: there was a gradual reduction of pressure injected in the middle ear after each sip due to the action of the eustachian tube; however, there was positive pressure left in the tympanic cavity after the three swallowings;
3. ill-functioning eustachian tube
3.1: Open tube - there was a quick release of pressure right after the first sip, though an open eustachian tube, or when there was pressure leak while trying to seal the external auditory canal; 3.2: Closed tube - when there was no release of pressure in the tympanic cavity, maintaining the positive 200dapa pressure.
Nasopharyngoscopy was conducted by an otorhinolaryngologist using the equipment Olympus ENF Type P3, Rhinolaryngoscope Olympus, coupled to a Color Video Printer MAVIGRAPH OF - 5000/UP - 5000 W/UP - 5050 SONY, AR - T2. The optic fiber was inserted in the nostril' that corresponded to the perforated side of the tympanic membrane. We asked the patient to swallow water and that was the moment we observed the status of the eustachian tube. The auditory tube behaviors observed were described as follows:
1. Closed eustachian tube at rest and opening during swallowing (F/A);
2. Closed eustachian tube at rest, maintained closed during swallowing (F/F);
3. Open eustachian tube at rest, maintained opened during swallowing (A/A);
4. Eustachian tube could not be visualized because of hypertrophy of pharyngeal tonsil (SEM VISAO);
5. Eustachian tube with secretion in the tympanic cavity at the nasal portion of pharynx.
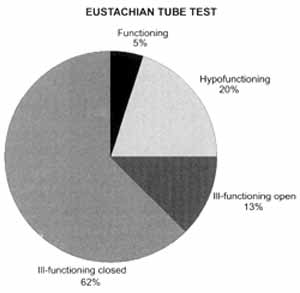
Graph 1. Distribution of eustachian tube status observed in the test of eustachian tube function for the participants of the sample.
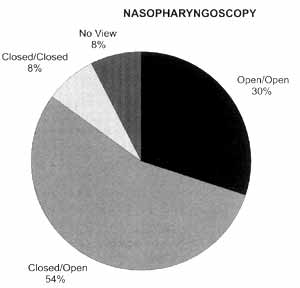
Graph 2. Distribution of eustachian tube status observed through nasopharyngoscopy in all subjects.
RESULTS
The results obtained from the application of the tests proposed by the present study are presented in Table 1, Graphs 1 and 2 and Figures 1, 2 and 3.
DISCUSSION
The results expected as normal by correlating the two tests were functioning eustachian tube according to the auditory tube test, indicating good permeability of air through the tube during its opening, caused by the action of palatini tensor muscle during swallowing11, and rhinopharynx visualization of closed tube ostium at rest and open ostium during swallowingl6,17 studied by nasopharyngoscopy. Such results were found in only two ears.
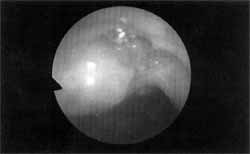
Figure 1. Image of closed and at rest ostium of eustachian tube visualized though nasopharyngoscopy.
Figure 2. Image of the ostium of the eustachian tube during swallowing, seen by means of nasopharyngoscopy.
Figure 3. Image of eustachian tube ostium, showing the presence of secretion, visualized by means of nasopharyngoscopy.
One of the reasons to explain the low number of normal results was the presence of secretion in 40% of the ears in the sample. Another study showed 72.7% of secretion in children and 23.1 % in adults16. The presence of secretion in the eustachian tube during the application of pressure in the tympanic cavity may lead to the false results of ill-functioning closed or hypo-functioning eustachian tube. The muscular movement responsible for opening the tube may be appropriate, but due to secretion, air is not normally released. The tube had no permeability to the air passage in 87.5 % of the ears with secretion in the eustachian tube, as may be seen in Figure 3.
In the three cases in which it was not possible to visualize the eustachian tube during nasopharyngoscopy (7.5%), we observed cases of pharyngeal tonsil hypertrophy. These subjects were referred to adenoidectomy by the otorhinolaryngologist who participated in the study. There was also a study in the literature showing that adenoids prevented appropriate visualization of tube ostium in 52 % of the children in the sample16.
In the remaining cases, it was not possible to relate visualization of nasopharyngoscopy with the results of eustachian tube function test; the results were in accordance with the literature that showed that each of the tests assess a different aspect of the structure, therefore, it is not possible to directly correlate them10.
During the performance of eustachian tube function test, no patients required more than three sips of water4.
The presence of secretion in the nasal portion of pharynx and in the eustachian tube influenced the results of auditory tube test, because it changed permeability of air through the eustachian tube.
CONCLUSION
The results obtained with the present study did not produce direct correlation of the data provided by the two tests, because each of them supplied different information about eustachian tube. Functioning and air permeability may be detected using the eustachian tube function test in ears with perforated tympanic membrane, by means of immitanciometer. In order to visualize structures at rest and during activity, nasopharyngoscopy is indicated.
Therefore, the two tests are complementary and important for a precise diagnosis of eustachian tube status. We believe that as a result of the use of both procedures, the otorhinolaryngologist will know more before indicating surgical procedures, such as tympanoplasty; thus, thanks to better scientific support, he or she may guarantee more successful results and lower risks of recurrence.
REFERENCES
1. ABIUSO, J.; MAY, A. - Estudo de la funcion tubaria en timpanos indemnes. Rev. Otorrinolaringol. Cir. Cabeza Cuello, 51: 32-7, 1991.
2. BLUESTONE, C. D. - Enfermedades y transtornos de la trompa de eustaquio: oido medio. In: PAPARELLA, M.M.; SHUMRICK, D.A.; GLUCKMAN, J. L.; MEYERHOFF, W L. Otorrinolaringología. 3 ed. Buenos Aires, Panamericana, 1994a. v 2. p. 1509-42.
3. BLUESTONE, C. D. - Fisiología del oído medio y de la trompa de eustaquio. In: PAPARELLA, M. M.; SHUMRICK, D. A.; GLUCKMAN, J. L.; MEYERHOFF, W L. Otorrinolaringología, 3 ed. Buenos Aires, Panamericana, 1994b. v 1. n.190-232.
4. CARO, J.; ARGOMEDO, C.; LEVY, R. - Nomalización de la prueba de función tubaria con timpano abierto por otitis media crónica. Rev. Otorinolaringol. Cir. Cabeza Cuello, 50: 125-31, 1990.
5. DOYLE, W J. - Physiology: introduction Ann. Otol Rhinol. Laringol, 94: 20-1, Suppl. 120, 1985.
6. FINKELSTEIN, Y; TALMI, Y E; RUBEL,Y; ZOHAR, Y - An objective method for evaluation of the patulous eustachian tube by using the middle ear analyzer. Arch Otolaryngol Head Nech Surg., 114: 1134-8, 1988.
7. HOLMQUIST, J. - Eustachian tube function and upper respiratory tract infection. Ann. Otol Rhinol. Laringol., 94: 41-2, Suppl. 120, 1985.
8. HONJO, I. - Clearance function of the eustachian tube. Ann. OW Rhinol. Laringol, 94: 29-30, Suppl. 120, 1985.
9. INIQUEZ, R.; ARAVENA, E - La permeabilidad tubaria en el pronostico de las timpanoplastias. Rev. Otorrinolaringol. Cir. Cabeza Cuello, 42: 6-9, 1982.
10. JAUMANN, M. E; STEINER, W; BERG, M. - Endoscopy of the pharyngeal eustachian tube. Ann. Otol. Rbinol. Laryngol. Suppl.. 89 (3): 54-5. 1980.
11. LOPES FILHO, O.; CAMPOS, C. A. H. de - Tratado de otorrinolaringologia. São Paulo, Roca, 1997. p.182 -3.
12. MONSELL, E. M.; HARLEY, R. E. - Eustachian tube dysfunction. Otolaryngol. Clin. North. Am., 29: 437-44, 1996.
13. ROOD, S. R.; DOYLE, W J. - Anatomy : introduction Ann. Otol. Rhinol Laringol., 94: 6-8, Suppl. 120, 1985.
14. STENFORS, L-E.; HELLSTROM, S.; ALBIIN, N. - Middle ear clearance. Ann. Otol. Rhinol. Laringol., 94: 30-1, Suppl. 120, 1985.
15. RUSSO, I. C. P; SANTOS, T. M. M. - Medidas da imitância acústica: avaliação quantitativa da função tubária. In: RUSSO, I. C. E; SANTOS, T M. M., dos. - A prática da audiologia clinica. 4.ed. Sao Paulo, Cortez, 1993. p.145-7.
16. TAKAHASHI, H.; HONJO, I.; FUJITA, A. - Endoscopic findings at the pharyngeal orifice of the eustachian tube in otitis media with effusion Eur. Arch. Otorbinolaryngol., 253: 42-4, 1996.
17. YAMASHITA, K. - Endoscopic testing methods. Ann.Otol. Rhinol Laringol., 94: 26-7, Suppl. 120, 1985.
* Audiologist at Hospital de Reabilitação de Anomalias Craniofaciais da Universidade de São Paulo (HRAC-USP), Bauru/SP
** Ph.D. Professor of the Course of Speech and Hearing Disorders at Faculdade de Odontologia de Bauru, Universidade de São Paulo (FOB-USP), Bauru/SP
*** Otorhinolaryngologist at HRAC-USP, Bauru/SP
Hospital de Reabilitação de Anomalias Craniofaciais (HRAC) - USP - Bauru /SP
Address for correspondence: Isabella Monteiro de Castro Silva - São 403 Bloco R - Apt° 202 - 70237-180 Brasília /DF - Tel: (5561) 226-8685 / 9977-0521
Article submitted on August 28, 2000 - Article accepted on January 15, 2001.


Print: ![]()