

Year: 2001 Vol. 67 Ed. 1 - (21º)
Relato de Casos
Pages: 127 to 130
Acoustic Neuroma in Children.
Author(s):
Oswaldo L. M. Cruz*,
Eduardo A . D. Veluttini**,
Maria E. B. Pedalini***.
Keywords: acoustic neuroma, children, unilateral sensorineural hearing loss
Abstract:
Acoustic neuroma is infrequently suspected when dialing with a child with unilateral sensorineural hearing loss. Although viral infection remains the first cause of unilateral sensorineural hearing loss in childhood, the possibility of acoustic neuroma should be included and the image study of temporal bone is advisable as it can disclose a tumor, otic capsule malformation or inflammatory process of the inner ear. The authors present a discussion regarding the diagnosis of unilateral sensorineural hearing loss in children and a search of literature, illustrated with a case of a 8 years old child with profound unilateral (right) sensorineural hearing loss detected for 6 months. The CT study showed a 4 cm acoustic neurinoma which could be totally removed. Although the child presented a good post-operative evolution a Grade III facial paralysis remains after one year. An early diagnosis could allow a better functional evolution of the facial nerve.
![]()
INTRODUCTION
Acoustic schwannoma, not related to type 2 neurofibromatosis, is rare in children younger than 16 years. Its frequency is even lower in ages below 10 years and in our literature research we found only 7 cases published and grouped in the excellent review on the topic made by Kusunose et al.², in 1990.
After that publication, we could not find any other report until our presentation of a case of .acoustic neuroma in a 8-year-old child.
In addition to the peculiarity of the case because of its low occurrence, the discussion of some clinical aspects of unilateral sensorineural loss in children, with inclusion of the diagnostic possibility of acoustic schwannoma, seems to be relevant since in such circumstances unilateral hearing loss is normally associated with viral infections, otitis, trauma and genetic syndromes, leading the specialist to an investigation that may overlook the tumor.
The presentation of this case intends to show the need to include the occurrence of 81'' nerve tumors in children, and that is essential to use all diagnostic resources available to diagnose pediatric unilateral sensorineural loss.
CASE REPORT
We evaluated an 8-year-old child who had complaint of hearing loss on the left for 6 months, noticed by the child because he could not speak on the phone with the left ear.
He had history of mumps that had taken place 3 years before and no other condition that could be related to hearing loss, such as use of ototoxic drugs, trauma, family history of hearing loss, otitis media or other infectious diseases.
ENT exam was normal and we did not find any evidence of the presence of Von Reckinghausen (milk and coffee skin spots, nodules, etc).
Audiometry revealed profound sensorineural hearing loss on the left, average of auditory thresholds at 120dB, 0% at speech recognition index (Figure 1), homolateral vestibular hyporeflexia and normal decreasing pendulum rotation test.
A previous audiometric study conducted in another clinic 2 months before showed less severe hearing loss (average of thresholds at about 60dB), but compromised speech discrimination (0%).
Figure 1. Pure tone audiometry showing unilateral profound sensorineural hearing loss (left) with 0% result in speech recognition index.
Lab tests revealed the presence of antibodies against the virus of mumps of IgM class, characterizing previous contact, but not recent or active disease. There were no antibodies against simple herpes virus or cytomegalovirus.
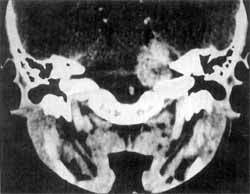
CT scan showed the presence of a large tumor mass in the right cerebellum-pontine region, uniform captation of iodine contrast, approximately 4 cm in size, located in the inner auditory canal (Figure 2). We did not observe alterations of the otic capsule or middle ear.
Diagnosis of acoustic schwannoma was made. The child was submitted to total resection of tumor via suboccipital access. Post-operatively, the patient remained well, except for facial paralysis grade IV (House-Brackmann). Histopathological analysis confirmed the diagnosis of schwannoma type Antoni A.
Post-op CT scan control was satisfactory; confirming the absence of residual tumor (Figure 3). During post-op follow-up we observed functional improvement of facial nerve paralysis up to grade III of House-Brackmann by the end of the first year.
Figure 2. CT at coronal section, after injection of contrast, revealing large expansive process located in the internal ear canal, characterizing an acoustic neuroma on the left.
Figure 3. Post-op CT scan at axial section showing total resection of the mass and bone defect of retromastoid suboccipital craniotomy.
DISCUSSION
Acoustic schwannomas are very rare in children who do not have neurofibromatosis. In the age range below 10 years, only 7 cases in English and none in Portuguese have been reported in the literature.
As to clinical manifestations of acoustic neuroma, they are almost identical in adults and children 5. However, a relevant fact is that these tumors are normally detected in children when there are already neurological symptoms, because unilateral hearing loss is not usually noticed by children. Even when there is complaint and detection of hearing loss, it is normally attributed to mumps, acute otitis media, secretory otitis media or more difficult causes to find, such as the genetic one. Owing to these aspects, lab tests and imaging investigations are rarely ordered in the routine assessment of unilateral sensorineural hearing loss in children.
However, it seems to be essential to use all possible resources because of etiological multifactorial aspects in such cases3, such as the investigation of mumps antibodies and imaging exams.
The indication of imaging techniques aims not only at the detection of acoustic neuroma, but also the diagnosis of internal ear malformations. Despite the fact that MRI is the most sensitive imaging exam for neurinoma detection, out recommendation is that the CT be asked in order to have the possibility of detecting malformations that are not evidenced by MRI. In cases of evident inflammatory impairment, such as otitis or viral infections, MRI may show the inflammatory activity of the inner ear.
Another fundamental aspect is to value findings of audiological tests. The progressive character of sensorineural loss, the unilateral affection or asymmetry of involvement, the disproportional low speech discrimination and absence of stapedial reflex (if the hearing loss permits its investigation), should receive special attention and indicate the need to carry on with the investigation. If possible, there is the indication of carrying out brainstem evoked potentials, in addition to lab tests and imaging techniques we have already mentioned.
The treatment of choice for schwannomas is surgery, since there is no other therapeutic possibility that could be used during childhood.
In the case presented here, surgery was uneventful, although there were some difficulties expected in childhood such as more bleeding because of increased tumor vascularization 1, 4. Even functional recovery of facial nerve was compatible with the results we have for resections of large tumors, showing that the behavior of that nerve in children is the same as in adults as to resistance to operative trauma. Nevertheless, if diagnosis-had taken place before, a resection of a smaller tumor would definitely contribute to better functional results of the facial nerve.
REFERENCES
1. ALLCUT, D. A.; HOFFMAN, H. J.; ISLA, A.; BECKER, L. E; HUMPHREYS, R. P. - Acoustic schwannomas in children Neurosurgery, 29: 14-18, 1991.
2. KUSUNOSE, M.; NISHIJIMA, M.; OKA, N.; YAMATANI, K; TAKAKU, A. - Acoustic neurinoma in a child. Neurol. Surg., (JP), 18: 301-306,1990.
3. MATTUCCI, K. F.; GLASS, W. M.; SETZEN, M.; LEVIN, W. - Childhood acoustic neuroma. N. Y. State J. Med. (December): 665-666, 1987.
4. RUHWORT, R. G.; STORBY, W. A.; SMITH, S. F. Acoustic neuroma in a child treated with the aid of preoperative arterial embolization. J. Neurosurg., 61: 396398, 1984.
5. SCHULMAN, M. H.; WELCH, K.; STRAND, R.; ORDIA, J. A. - Acoustic neuromas in children. AJNR 7: 519-521, 1986.
* Head of the Sector of Otology of the Discipline of Otorhinolaryngology - EPM - UNIFESP. Full Professor in Otorhinolaryngology, Faculdade Medicina da Universidade de São Paulo - FMUSP.
** Ph.D., Assistant - Division of Neurosurgery - Hospital das Clínicas da FMUSP.
*** Speech and Hearing Pathologist of the Sector of Speech and Hearing Pathology at Hospital das Clínicas da FMUSP.
Study conducted at Hospital Alemão Oswaldo Cruz.
Address for correspondence: Rua Mato Grosso, 128/74 - 01239-040 São Paulo /SP - Tel: (55 11) 256-6368 - Fax: (55 11) 256 9268 - E-mail: olacruz@sol.com.br
Article submitted on February 16, 2000. Article accepted on July 13, 2000.

Print: ![]()