

Year: 2001 Vol. 67 Ed. 1 - (10º)
Artigos Originais
Pages: 67 to 72
Otolaryngologic Manifestations of GERD in Children.
Author(s):
Claudia A. Eckley*,
Gisela Zuna**,
André C. Duprat***,
Henrique O. Costa****.
Keywords: reflux laryngitis, otitis, GERD, child
Abstract:
Introduction: The atypical manifestations of gastroesophageal reflux disease (GERD) may bring patients to the attention of the otolaryngologist and may present without digestive symptoms. In the pediatric population the diagnosis of upper respiratory menifestations of GERD becomes a special challenge due to the inability of smaller children to express their symptoms. Flexible laryngoscopy becomes pivotal to establish mucosal damage and other abnormalities caused by the refluxed material. Material and method: In this study the authors report 12 children, five boys and seven girls, with Otolaryngologic manifestations of GERD diagnosed through flexible endoscopy and digestive cintilography. Children's age ranged from four months to 12 years with a mean of 34 months. Results: Chronic Otitis Media was reported in 75% of children, 77% with rhinopharyngeal mucosal abnormalities. Deficit in weight gain was found in 83% of the children. All patients presented hiperemia and edema of the posterior larynx. Conclusions: The authors conclude that a strong suspicion is necessary for diagnosis of patients with recurrent/chronic otitis media or growing deficits. They also discuss the importance of flexible endoscopy, a minimally invasive, well tolarated procedure, for the diagnosis of the otolaryngologic manifestations of GERD in the pediatric population.
![]()
INTRODUCTION
Gastroesophageal reflux disease (GERD) has been attracting the attention of otorhinolaryngologists because of its head and neck manifestations. In pediatric patients, symptoms may be very different from those found in the classic manifestation of GERD, especially in patients too young to report their complaints. In addition to the diagnostic difficulties, infants present physiological regurgitation, and it becomes difficult to differentiate between normal and pathological reflux. Thanks to technological breakthroughs, it has been possible to diagnose the pathology in the pediatric population using less invasive methods. However, in order to diagnose GERD with otorhinolaryngological manifestations it is necessary to have a very strong clinical suspicion, which will be confirmed by the physical exam and analysis with flexible endoscopy.
The first description of the association between gastroesophageal reflux and laryngeal problems was made by Cherry and Marguiles in 1968 6, when they reported 3 cases of patients with laryngeal granulomas associated with reflux esophagitis. Since then, many studies have been published about the otolaryngological manifestations of the disease, both in adults and in children; it became evident that diagnosis of upper manifestations of the disease depends almost exclusively on a careful otorhinolaryngological exam, because in only about 30% of the patients with this form of GERD there are gastric and esophageal alterations2, 8,14,25.
Similarly to all new diseases, it takes time to understand the mechanisms involved, in its generation and maintenance, sometimes leading to misunderstanding and confusion. We initially believed that patients with suspicion of upper reflux (that affected larynx, pharynx, middle ear, trachea and bronchi) would necessarily have reflux esophagitis, hiatus hernia, or, other gastroenterological alterations compatible with the diagnosis of GERD, as we knew so far. We used well established diagnostic tools and interpretations for GERD, but we did not manage to confirm the diagnosis of otorhinolaryngological patients with hypothesis of reflux. However, therapeutic tests showed positive results in this population. Studies by researchers such as Koufman 25,27 and Oson 30, ended up proving that despite being caused by the same mechanism, gastroesophageal reflux disease has two different clinical manifestations: the classic form, manifested with esophagitis and called gastroesophageal reflux (GER), and an atypical form that may manifest upper symptoms, called laryngopharyngeal reflux (LPR). The explanation for the presence of upper symptoms without digestive symptoms lies in the anatomy and physiology of the digestive and respiratory tracts.
The esophagus has mechanisms of mechanical protection (recovering epithelium and mucus) and chemical protection (sodium bicarbonate produced in the esophagus and by the salivary glands, prostaglandins, mucins, epidermal growth factor, and other polypeptides capable of affecting the regeneration of the digestive tract), which make it resistant to small amounts of acid and pepsin that suffer physiological reflux5,15,21,38. Saliva is also responsible for the chemical balance of the digestive mucosa, working as a diluting agent, acid neutralizer and stimulator of metabolism of the digestive epithelium by means of the production of the same polypeptides referred above, and volume and concentration of these organic and inorganic substances are increased significantly in the dyspeptic disease in reflux esophagitis12,22,34,37. Respiratory mucosa, on the other hand, in addition to being a kind of epithelium that is less prepared for attacks, does not have a protective mucus barrier, and possibly does not benefit from the protective action of saliva, such as the digestive mucosa. Therefore, small amounts of reflux known as physiological for the distal esophagus, if they reach the larynx, pharynx or bronchial tree, will result in local alterations. This explains why such a large number of patients with signs and symptoms suggestive of gastroesophageal reflux in the larynx and pharynx have results of endoscopy and esophageal pH monitoring within the normal range.
In the present study, we will show clinical presentation, physical findings of head and neck, nasofibroscopic findings and pathologies most frequently associated in a group of 12 children diagnosed with gastroesophageal reflux disease with otolaryngological consequences.
MATERIAL AND METHOD
We studied 12 consecutive children between January 1998 and July 2000, who were submitted to nasofibrolaryngoscopic exam because of different complaints of the upper airways and the presence of findings suggestive of gastroesophageal reflux. The men age of children at diagnosis was 34 months (ranging from 4 months to 12 years). All children included in the exam were in the pre-puberty phase. Five were male and seven were female subjects.
Children were referred from other departments of the hospital or came to the Department of Otorhinolaryngology spontaneously, because of respiratory symptoms associated with swallowing or otological symptoms. After general ENT assessment, they were referred to the department that conducted flexible endoscopic exams and underwent the exam under topic anesthesia with lidocaine 2% with or without 1:1,000 adrenaline (depending on clinical contraindication to use nasal vasoconstrictor), applied in the nostril five minutes before the exam. We used a 3.5mm flexible optical fiber by Pentax coupled to a micro camera and VHS video system to record the exam. The optical fiber was introduced through the nostril of the patient who was seated, and we evaluated nasal fossa, rhinopharynx, torus tubarius, oropharynx, hypopharynx and the larynx.
Graph 1. Initial symptoms of 12 children with ENT manifestations of GERD.
Source: SAME ISCMSP, 2000.
Cases that had findings suggestive of GERD who had not been evaluated by the Service of Pediatric Gastroenterology were referred back to the department and esophagus and stomach scintigraphy, swallowgram, 24-hour pH monitoring or EGD - esophagogastroduodenoscopy were performed in order to confirm the diagnosis.
Data were complied and statistically analyzed.
RESULTS
Graph 1 shows the main complaints that motivated patients to search for treatment. The presence of liquid reflex in the mouth and nose was reported by 7 (58%) of the 12 patients, all of them below 2 years of age, and two of them had cerebral palsy and a significant delay in neuropsychomotor development. Dysphonia was reported by 4 out of 12 patients, normally described as transient and characterized by occasional weaker cry. Four patients (33%) had complaints of repetitive acute otitis media (AOM) and another five (42%) had secretory chronic otitis media (SOM), amounting to 75% of the patients with otological alterations. Seven (77%) of these nine patients with otological alterations also had inflammatory signs on the posterior wall of the rhinopharynx characterized by granular aspect and mucosa hyperemia. One patient with SOM also had moderate adenoid hyperplasia that partially occluded the region of torus tubarius bilaterally (Figure 1). Only one in 9 patients with otological alterations did not have rhinopharynx or, nasal fossa alterations, but he had marked edema and hyperemia of the posterior third of the larynx, on interarytenoid and retrocricoid regions and on the arytenoids (Figure 2). The most frequent laryngeal findings were edema and hyperemia of posterior larynx, found at variable degrees, from moderate (60%) to marked (40%) in all 12 cases. Associated laryngeal alterations were vocal folds nodules in one 12year-old patient who also had significant inflammatory signs on all larynx and pharynx, and complaint of night laryngospasm and unsolvable dry cough. Cough was reported by 6 out of 12 patients (50%), and it was generally dry and following feeding, or when the patient was placed on horizontal supine position. Repetitive pneumonia was reported by 4 out of 12 children, two of which also had cerebral palsy. Delayed growth and weight gain were reported in 10 out of 12 patients (83%) with diagnosis of GERD.
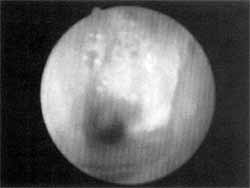
Figure 1. Nasofibroscopic aspect of the adenoid of one patient with GERD and repetitive otitis. We observed hyperplasia and purulent secretion of adenoid, as well as occlusion of torus tubarius.
Source: Ambulatory of Larynx, Department of Otorhinolaryngology at Santa Casa de São Paulo, 2000.
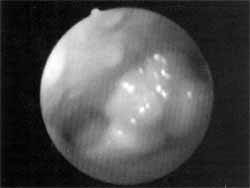
Figure 2. Nasofibrolaryngoscopic aspect of the larynx of a child with chronic laryngitis caused by GER. We observed marked edema of arytenoids and retrocricoid area, together with increase of lymphoid tissue on the posterior wall of hypopharynx, showing a granular aspect.
Source: Ambulatory of Larynx, Department of Otorhinolaryngology at Santa Casa de São Paulo, 2000.
All patients included in the present study were submitted to esophagus and stomach scintigraphy and had positive results for GER. Video swallowgram was conducted in 3 out of 12 patients, and it was interrupted in one 6-month-old patient with cerebral palsy because of intensive aspiration during the exam. Two-channel esophageal pH-monitoring-one channel on the distal esophagus and the other on the proximal esophagus, was conducted in two patients and it showed pathological reflux on the, proximal catheter in both cases. EGD was conducted in 3 children and one of them had esophagitis and the other two had moderate antral gastritis.
Patients were treated with pro-kinetics, posture and feeding modifications and surgery for non-responsive more severe cases. They showed significant improvement of signs and symptoms.
DISCUSSION
Otorhinolaryngological manifestations of GERD are atypical because initially they do not represent the disease and in many occasions they are not associated with perceptible digestive symptoms23, 24, 28, 29. In the pediatric population, diagnostic difficulty is even more marked because small children do not report symptoms. Head and neck symptoms normally associated with GERD and ENT manifestations in adults are dysphonia, throat clearing and pharyngeal bolus. These symptoms are obviously difficult to characterize in the pediatric population, and the most common symptoms in this age range are delay in growth and weight gain, cough and repetitive respiratory or otological infections1, 4, 9,10,16,19.
Dry cough in GERD is normally chronic and may present itself at any time during the day, but especially at night, at bed time. Apparently, not only the aspiration of the refluxed content generates the cough; it seems that the chemical stimulus of the distal esophagus is capable of triggering the reflex of cough7, 32. In addition, the cough itself increases intra-abdominal pressure and facilitates the additional reflux, contributing to the process. One of the most .dreadful symptom of LPR to the patient and the most worrying one to the physician is laryngospasm, a result of the increased concentration of Interleukin 2 on the inflamed mucosa, and secondarily derived from the liquor release of interleukin 6, which causes hyperreactivity of the larynx, specifically of the vocal folds. There are studies showing that the reflux on the proximal esophagus is capable of triggering the spasm of laryngeal reflex, because of the stimulus of laryngeal recurrent nerve 27. Patients with those symptoms are considered severe cases and require aggressive treatment.
LPR may affect the pharyngeal mucosa and cause a chronic inflammatory process of the rhinopharynx mucosa with symptoms of posterior nasal secretion, foul smell in the nose and nasal obstruction. Because it modifies the mouth pH directly or indirectly (through the dumping of saliva bicarbonate in the esophagus during the episodes of reflux), patients with GERD may have aphthas, repetitive stomatites, tooth decays and periodonditis²¹ ²².
In the pediatric population, rhinopharynx alterations are more common and they may generate repetitive adenoiditis and sinusitis, and because of the Eustachian tube, repetitive acute otitis media or secretory chronic otitis media3,18. Repetitive respiratory infections, in addition to leading to other respiratory complications, also compromise the growth and the development of children affected by the disease. The belief that reflux and repetitive otitis are associated is so strong that some physicians advocate the treatment of the latter with anti-reflux medication before surgical intervention. The number of advocators of anti-reflux treatment for children with difficult to thrive has also increased18,23,28. In our sample, 75% of the patients had otological alterations associated with the reflux and other 83% had delayed growth.
In the pediatric population, studies such as the one conducted by Giannoni, in 1998 18 and Bouchard, in 19993, showed an association of 61 to 64% of LPR and laryngomalacia, and these were the most severe cases. We did not find cases of GERD associated with laryngomalacia in the studied population.
As to diagnostic methods, although the world literature defends the use of two-channel 24-hour pH monitoring we still face difficulties when performing the exam in the pediatric population of our country1,3,11,13,17,20,26,33,39. European and American studies indicated a good acceptance of the exam by patients and parents, but the same is not true in Brazil. Therefore, the preferred exam to confirm the diagnosis of LPR in the pediatric population is scintigraphy, which has a sensitivity of about 80%. Flexible nasal laryngeal endoscopy, since it is less invasive, does not use radiation, does not pose risks of aspiration of contrast and enables excellent visualization of upper respiratory mucosa from the nasal fossae to rhinopharynx and larynx, is a valuable and essential tool for the diagnosis of otorhinolaryngological manifestations of GERD. The exam may be performed in probably all patients, provided that the family and patient collaborate. Although it causes some discomfort, it ceases when the device is removed, and it rarely causes any damage to the mucosa. The challenge is to exam older children that do not want to sit on the parent's lap and be restrained, so we need them to collaborate. When we carefully explain that it is not going to hurt and we incite the child's curiosity by saying we are going to see the nose on TV, the exam may be performed without physical or psychological traumas.
FINAL CONSIDERATION
Gastroesophageal reflux disease may be present with very distinct manifestations, and the laryngopharyngeal form is implied in up to 60% of the laryngeal complaints of patients that come to the otorhinolaryngologist and in up to 40% of the children that have difficulty to thrive. For the pediatric population, especially infants, there is a degree of physiological reflux. Pathological reflux cases are those that have temporary anatomical defects caused by the immaturity of the digestive tract, or permanent ones, because of digestive malformations. Most children with mild or moderate GERD manage to reach clinical control of the disease with posture and medication treatments after some months of growth and maturation. More severe cases, especially those with anatomical abnormalities, require surgical intervention or permanent isolation of respiratory tract in order to protect it from aspiration.
Although many studies on LPR have been made, we still do not completely understand the mechanisms involved in the upper manifestations of the reflex. Koufman believes that one of the factors responsible for reflux laryngitis is pepsin, which refluxes with the gastric content and is activated by an acid pH. Some studies have been designed to dose saliva pepsin in patients with LPR, but the test is not available for clinical practice yet. In addition to acid, alkali, or pepsin contained in the reflux, there should be some other local factor that justifies the hypersensitivity of the respiratory epithelium of some subjects compared to the others. There is still a lot to investigate in this area.
Similarly to other medical areas, this is an example of a disease that requires involvement of various specialists to treat patients appropriately. Therefore, the relationship between pediatrician, gastroenterologist, otorhinolaryngologist and pneumologist has to become very close, so that they may all share a common language in order to manage the patient together. The benefits from this joint approach are important for both the patient and the physician that aims at providing the well-being of patients.
REFERENCES
1. ACCORSINI, M.; AVERBENE, C.; CAIULO, V. A.; UGHI, C.; CECCARELLI, M.- La pH-metric esofagea delle 24 ore nella valutazione della patologia da reflusso gastroesofageo. Minerva Pediatr., 44: 185-188, 1992.
2. ARAÚJO, C. M.: Análise Crítica da pH-metric Esofágica no Refluxo Gastroesofágico a Laringofaríngeo. São Paulo, 2000. Dissertação de Mestrado - Faculdade de Ciências Médicas da Santa Casa de São Paulo.
3. BOUCHARD, S.; LALLIER, M.; YAZBECK, S.; BENSOUSSAN, A. - The Otolaryngologic Manifestations of Gastroesophageal Reflux: When is a pH Study Indicated? J. Pediatr. Surg., 34: 1053-1056, 1999.
4. BRULEY DES VARANNES, S.; RAVENBAKHT-CHARIFI, M.; CLOAREC, D.; PUJOL, P.; SIMON, J.; GALMICHE, J. P. Endobrachyoesophage et reflux gastro-oesophagien acide. Gastroenterol. Clin. Biol., 16: 406- 412, 1992.
5. BUMM, R.; FEUSSNER, H.; HÖLSCHER, A. H.; JÖRG, K.; DITTLER, H. J.; SIEWERT, J. R.- Interaction of gastroesophageal reflux and esophageal motility. Evaluation by ambulatory 24-hour manometry and pH-metry. Digestive Diseases and Sciences, 37(8): 1192-1199, 1992.
6. CHERRY, J.; MARGULIES, S. I.- Contact ulcer, of the larynx. Laryngoscope, 78: 1937-1940, 1968.
7. CONLEY, S. F.; WERLIN, S. L.; BESTE, D. J.- Proximal pH-metry for diagnosis of upper airway complications of gastroesophageal reflux. J. Otolaryngol., 24(5): 295-299, 1995.
8. COSTA, H. O.; ECKLEY, C. A.; FERNANDES, A. M. F.; DESTAILLEUR, D.; VILLELA, P. H. - Refluxo gastroesofágico: Comparação entre achados laríngeos a digestivos. Rev. Port. ORL, 35(1): 21-28, 1997.
9. DELAHUNTY, J. E.- Acid laryngitis. J. Laryngol. Otol., 86: 335-343, 1972.
10. DEVENEY, C. W.; BENNER, K.; COHEN, J.- Gastroesophageal reflex and laryngeal disease. Arch. Surg., 128: 1021-1027, 1993.
11. DUCHÉ, M.; FOURNIER-CHARRIÈRE, E.; DUCOT, B.; MESSERSCHMITT, C.; GOLDSZMIDT, D. - La Phmétrie de 24 heures en ambulatoire à domicile: Cécu parental et Familial. Étude prospective de 100 cas. Arch. Pédiatr, 2: 1047-1054, 1995.
12. DUTTA, S. K.; MATOSSIAN, H. B.; MEIROWITZ, R. F.; VAETH, J. - Modulation of Salivary Secretion by Acid Infusion in the Distal Esophagus in Humans. Gastroenterol., 103: 1833-1841, 1992.
13. EBERL, T.; WIENBECK, M.; BARNERT, J.Refluxösophagitis: manometrie and pH-metrie. Schweizerische Rundschau für Medizin (PRAXIS), 85(45): 1428-1431, 1996.
14. ECKLEY, C. A.; MARINHO, V.; RUIZ, W. S.; COSTA, H. O. - O uso da pH-metria Esofágica de Dois Canais no Diagnóstico da Laringite Crônica por Refluxo Gastroesofágico. Rev. Bras. ORL, 66(2): 110-114, 1999.
15. FIORUCCI, S.; SANTUCCI, L.; CHIUCCHIÚ, S.; MORELLI, A.- Gastric acidity and gastroesophageal patterns in patients with esophagitis. Gastroenterol., 103: 855-861, 1992.
16. FRASER, A. G. - Review Article: Gastro-oesophageal Reflux and Laryngeal Symptoms. Aliment Pharmacol. Ther., 8: 265-272, 1994.
17. GADEA, O.; OLMOS, J.; SOIFER, L.; DE LA CANAL, A.; PRECERUTTI, J.; DUBRA, C. - Variables pH-metricas en el reflujo gastro-esofagico del paciente asmatico. Acta Gastroenterol. Latinoamer., 23: 129-133, 1993.
18. GIANNONI, C.; SULEK, M.; FRIEDMAN, E. M. - Gastroesophageal Reflux Association with Laryngomalacia: A Prospective Study. Int. J. Pediatr. Otorhinolaryngol., 43: 11-20, 1998.
19. GUMBERT, L.; KALASH, N.; CHRISTOPHIE, D.; CONTENCIN, P. - Hoarseness and Gastroesophageal Reflux in Children. J. Laryngol. Otol., 112: 49-54, 1998.
20. HALAMA, A. R. - Clinical approach to dysphagic patient. Acta Oto-rhino-laryngologica Belg., 48: 119-126, 1994.
21. HANSEN, G.; MÜLLER, C.; SINHA, P. - Gastric Ulcer is Accompanied by a Decrease of Epidermal Growth Factor in Gastric Juice and Saliva. J. Clin. Chem. Clin. Biochem, 27: 539-545, 1989.
22. HELM, J. F.; DODDS, W. J.; HOGAN, W. J.; SOERGEL, K. H.; EGIDE, M. S.; WOOD, C. M. - Acid Neutralizing Capacity of Human Saliva. Gastroenterol., 83: 69-74, 1982.
23. HENDEL, J.; HENDEL, L.; AGGESTRUP, S.- Morning or evening dosage of omeprazole for gastro-oesophageal reflux disease? Aliment Pharmacol. Ther., 9:693-697, 1995.
24. KASAPIDIS, P.; XYNOS, E.; MANTIDES, A.; CHRYSOS, E.; DEMONAKOU, M.; NIKOLOPOULOUS, N.; VASSILAKIS, J.- Differences in manometry and 24-H ambulatory pH-metry between patients with and without endoscopic or histological esophagitis in gastroesophageal reflux disease. Am. J. Gastroenterol., 88(11): 1893-1899, 1993.
25. KOUFMAN, J. A.- The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH-monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope, 101(4, Part 2, Suppl. 53):1-78, 1991.
26. LI, V.; BOST, R.; CARAVEL, JP.; FOURNET, J.; HOSTEIN, J.- Endobrachyoesopage, reflux gastro-oesophagien acide et reflux duodénogastrique en période inter-digestive et postprandiale. Gastroenterol. Clin. Biol., 16: 978-983, 1992.
27. LOUGHLIN, C. J.; KOUFMAN, J. A. - Paroxysmal Laryngospasm Secondary to Gastroesophageal Reflux. Internet: jkoufman@ bgsm.edu, 1998.
28. METZ, D. C.; CHILDS, M. L.; RUIZ, C.; WEINSTEIN, G. S. - Pilot Study of the Oral Omeprazole Test for Reflux Laryngitis. Otolaryngol. Head & Neck Surg., 116(1): 41-46, 1997.
29. NASI, A.: Doença do Refluxo Gastroesofágico. Reavaliação Clínica, Endoscópica a Monitorização com pH metria Intraluminar Esofágica. Estudo Clínico. São Paulo, 1996. Tese de Doutourado - Faculdade de Medicina da Universidade de São Paulo.
30. OSON, N. R.- Effects of stomach acid on the larynx. Proc. Am. Laryngol. Assoc., 104: 108-112, 1983.
31. OTT, D. J. - Gastroesophageal Reflux: What is the Role of Barium Studies? AJR, 162: 627-229, 1994.
32. PATTERSON, W. G.; MURAT, B. W. - Combined ambulatory esophageal manometry and dual-probe pH-metry in evaluation of patients with chronic unexplained cough. Dig. Dis. and Sci., 39 (5): 1117-1125, 1994.
33. SARASWAT, V. A.; DHIMAN, R. K.; MISHRA, A.; NAIK, S. R.- Correlation of 24-hour esophageal pH patterns with clinical features and endoscopy in gastroesophageal reflux disease. Dig. Dis. and Sci., 39 (1): 199-205, 1994.
34. SAROSIEK, J.; McCALLUM, R. W.- Do Salivary Organic Components Play a Role in Health and Disease of the Esophageal Mucosa? Digestion, 56 (Suppl 1): 32-37, 1995.
35. SHAW, G. Y.; SEARL, J. P. - Laryngeal manifestations of Gastroesophageal Reflux before and after Treatment with Omeprazole. South Med. J., 90 (11): 1115-1122, 1994.
36. SMIT, C. F.; TAN, J.; DEVRIESE, P. P.; MATHAUS-VLIEGEN, L. M. H.; BRANDSEN, M.; SCHOUWENBURG, P. F. - Ambulatory pH Measurements at the Upper Esophageal Sphincter. Laryngoscope, 108: 299-302, 1998.
37. SONNENBERG, A.; STEINKAMP, U.; WEISE, A.; BERGES, W.; WEINBECK, M.; ROHNER, H. G.; PETER, P. - Salivary Secretion in Reflux Esophagitis. Gastroenterol., 83: 889-895, 1982.
38. TOBEY, N. A. - How does the Esophageal Epithelium Maintain Its Integrity? Digestion, 56 (Suppl 1): 45-50, 1995.
39. WEINBECK, M.; BARNERT, J.; EBERL, T.- Gesicherte Indikationen für manometrie and pH-metrie der speiseröhre. Internist, 27: 714-722, 1986.
40. WIENER, G. J.; KOUFMAN, J. A.; WU, W. C.; COOPER, J. B.; RICHER, J. E.; CASTELL, D. O.- The pharyngo-esophageal dual ambulatory pH probe for evaluation of atypical manifestations of gastroesophageal reflux. Gastroenterol., 92: 1694-1697, 1987.
* Assistant Professor of the Department of Otorhinolaryngology at Santa Casa de São Paulo.
** Master studies under course at the Department of Otorhinolaryngology, Santa Casa de São Paulo.
*** Professor of the Department of Otorhinolaryngology at Santa Casa de São Paulo.
**** Joint Professor of the Department of Otorhinolaryngology at Santa Casa de São Paulo.
Study conducted at the Department of Otorhinolaryngology Santa Casa de São Paulo.
Study presented at 35° Congresso Brasileiro de Otorrinolaringologia, with was awarded with a special citation.
Address for correspondence: Dra. Claudia Eckley - Rua Sabará 566, cjto. 23 - Higienópolis - 01239-011 São Paulo /SP - Tel/ Fax: (55 11), 257-2686.
E-mail: ceckley@unysis.com.br
Article submitted on. August 15, 2000. Article accepted on October 20, 2000.
Print: ![]()