

Year: 2001 Vol. 67 Ed. 1 - (1º)
Artigos Originais
Pages: 9 to 14
Noise-Induced Hearing Loss: Analysis of the Tonal Audiometry Findings, Potencials Evoked by the Cerebral Trunk and Otoacoustic Emissions Evoked by Distortion Product.
Author(s):
Líscia, L. A. Ferreira*,
José A. M. Silveira**,
Cristiane C. Percebo***,
Fabiana Gonçalez****.
Keywords: noise-induced hearing loss, hearing thresholds, otoacustic emissions, brainstem auditory evoked potentials, audiometry.
Abstract:
Material and method: The authors evaluated the tonal audiometry, logoaudiometry, presence of the estapedic reflex, brainstem auditory evoked potentials (BERA) and otoacustic emissions by products of distortion findings, in 80 ears of patients exposed to intense noise and directed for investigation of noise-induced hearing loss in the period of october of 1998 to october of 1999. The audiometry was evaluated by the curve types, discrimination and presence or absence of Metz recruiting; in BERA were appraised: the waves morphology, the intervals range I-V and the hearing threshold; the otoacustic emissions were evaluated by the alterations of the products of distortion. The findings of the exams were studied separately and among themselves. Results: In the tonal audiometry, the more constant type of curve was the sharp fall, and there was alteration of the products of distortion in 82,4% of the ears with loss starting from 3 kHz, 93,3% starting from 4 kHz and 91,9% starting from 6 kHz. The authors call attention for the great importance in the study of those frequencies in exposed patients to noise. As for the hearing loss degree, the authors found light degree in 20,55 of the ears, moderate in 32,4 %, moderate-severe in 25,6%, severe in 9,46% and deep in 10,81% of the ears In study of BERA, the alteration of morphology of the waves was distributed like this: 13,75 % of alteration in wave 1, 12,5 % in wave III and 12,5% in wave V. As for the interval range I-V, alteration was observed in 15% of the ears. To BERA we found differences of thresholds between the tonal audiometry and the evoked potential that varied from 26,6 to +31,7 dB, being the average of those values of 4,48dB and the medium of 5,0dB. By the otoacustic emissions by products of distortion's study we observed alteration of those values in 41,25% of the ears in 2 khz, in 72,5% of the ears in 4 kHz and in 72,5% of the ears in 4 kHz. The ears that presented threshold alterations in tonal audiometry were studied as the presence or alteration of the distortion products to the otoacustic emissions. Ali the patients with alteration of the threshold to the tonal audiometrygram Independently of the attacked frequency, showed, alteration of the answers to the oto-acoustic emissions. Among the seven ears with normal tonal audiometry two were observed with threshold alteration to BERA and one with alteration of the products of distortion. Conclusion: The obtained data, suggests that the objectives exams are more sensitive in the diagnosis of PAIR, than the tonal audiogram, however a segment of a larger number of patients exposed to noises with normal audiometry is necessary so that such affirmative such affirmative can be confirmed.
![]()
INTRODUCTION
Hearing has a key role in the integration of men into the society. In the United States, about 28 million people have hearing losses and out of this total, 10 million of them were caused by excessive exposure to noise5.
Noise induced hearing loss (NIHL) is a cumulative and insidious cochlear pathology, generally resulting from the prolonged exposure to noise in the work environment without use of ear protector. It is caused by any regular exposure of about 90dBSPL, eight hours a day, for many years5.
Many studies have been conducted in order to describe the alterations and to correlate findings of pure tone audiometry, auditory brainstem evoked potentials (BERA) and otoacoustic emissions (OAE) in patients exposed to high intensity noise. Suzuki et al .8 showed a close relation between pure tone audiometry and BERA thresholds in patients exposed to noise, and BERA thresholds were better than the audiometric ones in 20dB or more. Another study by Jerger and Mauldin3 found that pure tone audiometry thresholds in 1, 2 and 4 KHz could be 40% lower than those found in BERA. Noorhassin et al.4 observed that patients with pure tone thresholds of up to 25dB who had been exposed to noise presented alterations in the morphology of BERA waves in 57% of the cases. Hall and Lutman¹ concluded that serial OAE in patients exposed to noise could detect minimal alterations of cochlear function, before the hearing loss could be detected in the pure tone audiometry.
The objective of the present study was to assess the findings and compare the sensitivity of pure tone audiometry, speech discrimination, brainstem evoked potentials and distortion product evoked otoacoustic potentials in patients exposed to high intensity noise.
MATERIAL AND METHOD
We selected 80 ears of 42 patients with hypothesis of NIHL, referred to Clínica Otorhinus, in São Paulo, between October 1998 and October 1999.
Forty-one patients (97.6%) were male and one was a female patient, with ages ranging from 27 to 70 years (median age of 49 years).
In all selected ears we conducted pure tone audiometry, speech discrimination, acoustic immitance, brainstem evoked potentials (BERA) and distortion product evoked otoacoustic potentials (DPOAE).
Pure tone audiometry was performed in sound proof booth, using the equipment MAICO-MA41 and acoustic immitance was made with the impedanciometer Rexton Impedance Audiometer 128. For BERA, we used the equipment Amplaid MK-12 with surface electrode. The active electrode was placed on the forehead, the reference one on the mastoid bone on tested side and the ground electrode was placed on the opposite mastoid. We used clicks as stimuli, presented through earphones at intensities from 50 to 120dbSPL. To conduct otoacoustic emissions, we used the program Scout Sport (Distortion Product Otoacoustic Emissions Measurement System - program version 1.54) by Biologin Systems Corporation, evaluating frequencies from 0.5 to 8 kHz.
In the pure tone audiometry, we assessed auditory thresholds and the curve was classified as: plateau, descending (hearing loss from 2 KHz on), fall in high frequencies (as from 3 KHz), notch and normal. Data from speech discrimination were classified as: less than 80%, between 80 and 88% and more than 88%; in addition we registered the presence or absence of recruitment.
We studied morphology of BERA waves I, III and V, interpeak interval I-V and hearing thresholds. In otoacoustic emissions, we investigated the presence of distortion product in frequencies 2, 4 and 6 KHz.
Findings from BERA and OAE were compared to pure tone thresholds in frequencies 3, 4 and 6 KHz. The mean pure tone thresholds for frequencies 2, 4 and 6 KHz were compared to the thresholds obtained at BERA.
RESULTS
Table 1 shows the distribution of the different types of curve obtained in 80 studied ears; it also shows speech discrimination and presence or not of Metz recruitment.
Upon evaluating the severity of hearing loss in each ear that had thresholds alterations, regardless of the affected frequency (73/80 - 97.25%), we found mild hearing loss in 15 ears (20.55%), moderate loss in 24 ears (32.4%), moderately severe loss in 19 ears (25.6%), severe loss in 7 ears (9.46%) and profound in 8 ears (10.81%). In all ears that presented sensorineural loss, we observed reduced thresholds in 3, 4, 6 or 8 kHz.
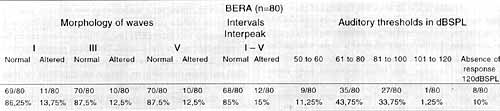
Findings of BERA and morphology of waves I, III and V, interpeak interval I-V and auditory thresholds are shown in Table 2.
Findings of DPOAE in frequencies 2, 4 and 6 KHz are shown in Table 3.TABLE 1 - Findings of pure tone audiometry.
TABLE 2 - Findings of evoked potentials
Comparing the results obtained by pure tone audiometry, BERA and DPOAE, we observed isolated alteration in the audiometry in one ear (1.25%), isolated alteration in BERA in four ears (5%), and isolated alterations of DPOAE in one ear (1.25%). Associated alterations between audiometry and BERA, in the presence of normal DPOAE, were found in 8 ears (10%); alterations in audiometry and otoacoustic emissions in the presence of normal BERA were found in 5 ears (6.25%), normal audiometry and alterations of BERA and DPOAE were found in 4 ears (5%). Fifty-four ears had alteration in all 3 procedures (67.5%), whereas in 3 cases there were no alterations in any of the exams (3.75%).
We studied the ears that presented abnormal thresholds at audiometry (n=73) to check if they had normal or altered distortion product otoacoustic emissions. All patients who had abnormal thresholds at audiometry, regardless of frequency, also had abnormal response to DPOAE. By studying the frequencies of 3, 4 and 6kHz, we observed abnormal response to DPOAE in 61 ears (82.4%) as from 3 kHz; in 69 ears (93.3%) as from 4 kHz and in 68 ears (91.9%) as from 6 kHz.
Among the seven ears with normal pure tone audiometry, only one case did not show DPOAE. Among the 45 ears with sensorineural loss up to SSdB in frequencies 3, 4 and 6KHz, 41 ears (91.1%) had alteration of DPOAE and, in the same group, 38 ears with moderate hearing loss (thresholds between 40 and 55dB) presented the highest incidence of alterations of otoacoustic emissions - 94.7% (36/38).
DISCUSSION
It is known that chronic exposure to noise leads to damage of outer hair cells, especially those located on the cochlear basal spiral, as well as reduction of cochlear flow and steriocilia impairment, resulting in reduction of fast contraction of outer hair cells and degeneration of nervous fibers of Corti´s organ 8. Extension and location of histological lesions depend on the frequency of noise, sound pressure level, and duration of exposure; however, susceptibility to this damage has an individual nature.
The hearing loss has a faster evolution in the first 10 to 15 days of exposure and after some years, it seems to reduce it, reaching a plateau. Initially, the most affected frequencies are in the range of 4 to 6KHz, with less marked losses above or below this range, creating what is called a notch. As a result of continuous exposure, the middle frequencies are affected, impairing the conversational area and reducing speech recognition5.TABLE 3 - Findings of distortion product otoacoustic emissions.
TABLE 4 - Comparison of findings of audiometry, BERA and OAE.
The diagnosis of work-related hearing loss is not al ways simple because audiometric profiles are variable. A constant characteristic is the presence of recruitment investigated by stapedial acoustic reflex (Metz recruitment). In patients with NIHL, the difference in minimal audibility thresh olds and stapedial reflexes reaches values below 60dB, characterizing it as a recruiting disease5.
Since it is a pathological entity that may result in lawsuits and claims for indemnification all over the world, including Brazil, objective tests are required to confirm the veracity of the disease, such as brainstem evoked potentials (BERA) and otoacoustic emissions.
When evaluating brainstem evoked potentials in subjects with NIHL, similarly to all patients who have cochlear pathology, we observed the presence of well defined wave: I, III and V at intensities close to the auditory threshold characterizing the occurrence of recruitment. In cases in which there is a significant fall in high frequencies, we may found absence of response or a pattern similar to that of a conductive hearing loss, with increased latency from wave I on, but with maintained values for interpeak intervals4.
Another objective test conducted to assess subjects with hypothesis of NIHL is the investigation of otoacoustic emissions. Transient evoked otoacoustic emissions are obtained by stimuli that have pure tones between 400 and 4,OOOHz, or 600 and 6,000Hz. It is a wide band sign that stimulates the cochlea as a whole and these emissions can be captured in patients who have hearing thresholds above 25 to 30dB. Another kind of emission that surges almost spontaneously in the presence of an acoustic stimulus is the distortion product, and it may be generated at any frequency using selected stimuli; the test is used to evaluate the cochlear activity in specific frequencies. Owing to its -similarity with the audiometric curve and the possibility of evaluating the ciliary cell functions at different points of the cochlea, distortion products have more clinical application than transient evoked potentials. DPOAE may be captured at the frequencies 0.5 to 8KHz in subjects who have thresholds up to 50dB¹.
In the present study, upon evaluating the isolated audiometry of each patient, we observed that the type of curve most commonly found was sharp fall in high frequencies in 41.25%. As to speech discrimination, the vast majority (77.5%) showed normal results and recruitment was present in 75% of the ears. Despite the fact that this audiometric profile is more commonly found in other pathologies, such as ototoxicity and presbyacusis, and that the notch curve is considered typical of NIHL, we should always consider the hypothesis of NIHL when presented with a curve that has a fall in highs, which was the predominant type in our study.
At BERA, we observed alterations of auditory thresholds, presence or absence of responses to waves I, III and V, interpeak I-V interval and morphology of wave. Morphology of curves and interpeak intervals did not provide significant data for diagnosis of NIHL, differently from what was observed by Noorhassin et al.4. On the other hand, BERA showed abnormal auditory thresholds in 33.3% of the subjects who had normal pure tone thresholds, agreeing with the findings by Jerger and Mauldin². For each ear, we calculated the average for pure tone thresholds in frequencies 2, 4 and 6KHz and compared to the thresholds of BERA. We did not consider sensorineural losses above 90dBHL (11/80 - 13.75%). We found differences in thresholds between the two exams that ranged from -26.6 to + 31.7dB, mean of 4.48dB and median of 5.0dB. These figures are in accordance with the study by Suzuki et al.8, who also found a close relation between thresholds of pure tone audiometry and BERA in patients exposed to noise. However, in the present study, the median of the difference was smaller than that found by Suzuki.
When we evaluated DPOAE comparing with severity of hearing loss in pure tone audiometry and the most affected frequencies, it was possible to observe that, regardless of the severity of hearing loss, all patients with abnormal thresholds had abnormal DPOAE in the affected frequencies (absence of distortion product). Taking into account that all patients with sensorineural hearing loss have a fall in 3, 4, 6 or 8KHz, and studying the otoacoustic emissions in the frequencies 3, 4 and 6KHz in these 73 ears, we observed alteration of distortion product in 61 ears (82.4%), from 3KHz on, in 69 ears (93.3%) from 4KHz on, and in 68 years (91.1%) from 6KHz on. These findings confirm the data from the audiometry and show the importance of investigating these frequencies in patients exposed to high intensity noise.
Among the ears that showed hearing thresholds within normal ranges, we observed 2 alterations of thresholds in BERA without alteration of otoacoustic emissions. In one normal ear, showing thresholds lower or equal to 20dBHL except for 4KHz, in which it was 25dBHL, we observed alteration of distortion product at the same frequency. There was a trend in our study showing that BERA and otoacoustic emissions may present alterations earlier than pure tone audiometry when it comes to noise exposure; however, follow-up of a larger number of patients without hearing loss employing the three exams would be required to compare the sensitivity of the procedures.
CONCLUSION
In the present study, pure tone audiometry alterations resulting from chronic exposure to high intensity noise were more frequently found in the frequencies above 3KHz, and fall in high frequencies was the most prevalent curve; therefore, otorhinolaryngologists should be careful upon the finding of this type of curve in the evaluation of noise exposed subjects. According to the results obtained, all patients with sensorineural hearing loss induced by noise had alterations of frequencies 3, 4, 6 and 8HKz, and alterations of distortion products were present in 82.4% of ears that had losses from 3KHz on, in 93.3°/0 of those with losses from 4KHz on and in 91.1% of those from 6KHz on. The authors pointed out the importance of studying these frequencies in patients exposed to noise.
Among those ears with thresholds within normal range, we detected alteration of distortion product in one case, and alteration of BERA threshold in two, suggesting higher sensitivity of otoacoustic emissions and BERA in cochlear damage caused by noise exposure when compared to pure tone audiometry. In order to confirm this hypothesis, we believe that more studies following up normal hearing individuals that are exposed to noise for prolonged periods of time should be conducted.
REFERENCES
1. HALL, A. J.; LUTMAN, M. E. - Methods for Early Identification of Noise Induced Hearing Loss. Audiology 38: 277-280, 1999.
2. JERGER, J.; MALDIN, L. - Prediction of Sensorineural Hearing Level from the Brainstem Evocated Response. Arch. Otolaryngol., 104: 456-461, 1978.
3. LASMAR, A..; NUELMANN, A.; COSTA, E.; SELIGMAN, J.; IBAÑEZ. R..- Perda Auditiva Induzida por Ruído. 1ª edição; Porto Alegre, Editora Bagaggem Comunicação Ltda.; 1997; p. 153-161.
4. NOORHASSIM, I.; KIMITAKA, K.; KOUSUKE, N. - Pure Tone Audiometry and Audiometry Brainstem Response in Noise Induced Deafness. Am. J. Otolaryngol 17.- 31-35, 1996.
5. NUELMANN, A.; COSTA, E.; SELIGMAN, J.; IBAÑEZ, R. Perda Auditiva Induzida por Ruído, 1ª edição; Porto Alegre, Editora Bagaggem Comunicação Ltda.; 1997; pg 15-291.
6. OLIVEIRA, J. A. A.; NUELMANN, A.; COSTA, E. , SELIGMAN, J.; IBAÑEZ, R. - Perda Auditiva Induzida por Ruído, 1ª edição; Porto Alegre, Editora Bagaggem Comunicação Ltda; 1997; p. 101-142.
7. SELIGMAN, J.; NUELMANN, A.; COSTA, E.; SELIGMAN, J.; IBAÑEZ, R. - Perda Auditiva Induzida por Ruído, 1ª edição; Porto Alegre, Editora Bagaggem Comunicação Ltda.; 1997; p. 144.
8. SUZUKI, T.; KODERA, K.; KAGA, K. - Auditor Evocated Brainstem Response Assessment in Otolaryngology. Ann NY Acad. Sci, 388: 480-500, 1982.
9. WERNER, A. F.; MENDEZ, A. M.; SALAZAR, E. B. - El Ruido y la Audición. Buenos Aires, Ad-Hoc SRL Ed,1990.p.85-99.
* Collaborating Physician of the Department of Otorhinolaryngology ar Hospital das Clínicas da Faculdade de Medicina de São Paulo (HCFMUSP).
** Director of Clínica Otorhinus, Ph.D. and Assistant of the Clinic of Otorhinolaryngology at HCFMUSP, Assistant of the Clinic of Otorhinolaryngology at Casa de Saúde Santa Marcelina.
*** Resident Physician of Clínica Otorhinus.
**** Physician, Preceptor of Residents at Clínica Otorhinus, responsible for seminars of the Service of Otorhinolaryngology at Clínica Otorhinus and Casa de Saúde Santa Marcelina.
Study presented at 35° Congresso Brasileiro de Otorrinolaringologia, which received a special citation. Study conducted at Clínica Otorhinus.
Address for correspondence: Centro de Estudos Alexandre Médicis da Silveira (CEAMS) - Rua Cubatão, 1140 - 04013-044 São Paulo /SP.
Tel: (55 11) 572-0025-Fax: (55 11) 572-7373.
Article submitted on August 15, 2000. Article accepted on October 20, 2000.


Print: ![]()