

Year: 1992 Vol. 58 Ed. 2 - (14º)
Relato de Casos
Pages: 144 to 146
Metastatic small cell carcinoma presenting as a polyp ias the external auditory canal.
Author(s):
Ivanir Spezio Melo*,
Carlos Renato Melo*,
Evandro Sobroza de Mello*,
Carlos Thadeu Cerski**
Keywords: carcinoma, neoplasm metastasis, ear canal
Abstract:
Metastatic carcinoma presenting as an aural polyp is a rare tumor. A review of the literature revealed less than 140 reported cases. The common primary sites are the breast, the lung, and the kidney. A case of small-cell carcinoma of the cervix that metastasized to the external auditory canal, producing facial paralisy in a 74-years-old woman is described.
![]()
INTRODUCTION
Malignances affecting the temporal bone are uncommon conditions and metastatic tumors of this region are less frequent. To date less than 140 cases were reported 1. However, this number will be probably overpassed dite to the agressive therapy used on many primary tumors which permits longer survival times thus allowing more opportunity for unusual metastatic manifestation2. A case of small cell carcinoma (SCC) of the cervix with metastases to the external auditory canal (EAC) with a brief review of the literature are presented here. To our knowledge, only five cases originating from the cervix and uterus have been reported and this is the first of SCC of the cervix metastatic to the EAC.
CASE REPORT
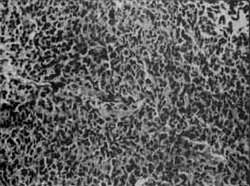
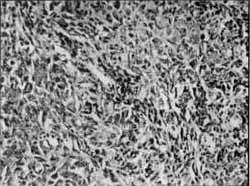
A 74-years-old white woman had the diagnosis of stage III B cervical poorly differentiated squamous cell carcinoma in January 1988 at another institution. On gynecological examination, the uterine cervix had a destructive vegetating tumor reaching the middle third of the from wall of the vagina. Rectal examination revealed extension of the mass to the pelvic wall. She was submitted to radiotherapy from February to April of the same year, and an apparently total regression of the tumor was obtained. In January 1989, when she returned to control, she presented with right-sided facial paralysis. An audiogram was not performed. Otological examination revealed a hemorrhagic tumoral mass protruding in the right auditory canal, without aural discharge. A biopsy of this mass disposed a neoplasm consisting of small cells with round to oval and spindle-shaped nuclei with scant cytoplasm disposed in a trabecular pattern, with high mitotic activity, and extensive necrotic areas (Fig. 1). Tissue for electron microscopic examination was fixed in 2.5% glutaraldehyde, postfixed in 1% cacodylate-buffered osmiun tetroxide, and embedded in Epon 812. Thin sections were examined with an electron microscope Zeiss Emm-9. Imunohistochemical investigation was performed in both cervical and ear biopsies and primary antibodies were localized using the avidin-biotin-complex method. Microscopic examination of the slides from the cervical biopsy revealed groups of malignant small cells, clustered around small vessels, and embedded in a necrotic background (Fig. 2). Grimelius stain was negative. Neoplastic cells were positive for keratin (AE1/AE3) and for epithelial membrane antigen (EMA), with many of them weakly positive for neuron-specific enolase (NSE), and negative for myoglobin, for carcinoembrionic antigen (CEA), and for protein S 100. Eleronic microscopy revealed cells closely apposed and occasionaly attached by small cell junctions with nuclei entoured by very irregular membranes (Fig. 3). Their cytoplasm contained few organelles and scattered membrane-bound neurosecretory granules (Fig. 3, inset). Chest roentgenograms showed no evidence of primary or secondary lung tumor. No further treatment was performed and the patient died at home within some weeks. Postmortein examination was not performed.
FIGURE 1
FIGURE 2
FIGURE 3
DISCUSSION
Metastatic tumors of the external auditory canal (EAC) are very rare. One of such unusual cases was found shortly before a sigmoidoscopy revealed a carcinoma of the rectum3. Almost all other cases were associated with signs of facial palsy and probably represent an extensive from the temporal bone metastasis. Acoordingly to JAHN et a14. metastatic tumor in the mastoid air cells reaches the tubotympanic cavity and external canal through vascular subepithelial vessels. FRIEDMAN et a15 reported four cases of metastases in the temporal bone, one of them presented as a bleeding mass protruding from the EAC and originating from a primary lung carcinoma. MADOX6 reported four additional cases, one of them also presenting as an aural polyp secondary to another lung carcinoma to which he added fine other cases from his review of the literature. Other such case was reported by SCHUKNECHT et al 7 from a total of ten cases secondarily involving the temporal bone. Amongst 35 malignant tumors of the EAC, CRABTREE et al8 described a case of metastatic tumor originating from the kidney. An interesting case appearing as a polyp in the EAC eight years after a neplhrectomy by renal carcinoma was reported by FERRON et al9 and considered as metastatic from the kidney tumor.
The cases described by HILL et al 10 and by MERRICK11 had their origin in an adenocarcinoma of the large bowel. More recently SALDANHA et al12 and MORTON et all added two new cases of metastases to the temporal bone secondary respectively to carcinomas of the bladder and breast, both presenting as a mass in the EAC. Of the nearly 140 published cases, the most common primary tumors are carcinomas of the breast, lung, and kidney1.
Cranial nerve palsies in patients with metastatic disease may result from entrapment of the nerve by leptomeningeal carcinomatosis, as it emanates from the cranium, or from incresead intracranial presure. Secondary tumors of facial nerve are not uncommon and facial nerve paralysis may also result from extensive intratemporal tumor involvementl3. In the latter case, facial nerve may be reached by an expanding tumor which have extend to the middle ear cleft and eroded the facial canal 2. Tumoral involvement of the facial nerve is estimate to cause about 5 per cent of all cases of peripheral facial paralysisl4. Isolated facial nerve paralysis was the presenting symptom in one of 27 patients with metastatic temporal bone tumors reviewed by MADDOX6. Actually, facial nerve paralysis has a higher incidesce in cases of metastatic disease and as many as 34 percent of patients developed it in the course of the disease.
Our patient presented initially with facial paralysis and an aural polyp and these were file only symptons she mentioned until-she was seen for the last time. However, a variety of otologic symptoms can be present in these patients. Aside the symptom triad of otalgia, preauricular swelling, and facial nerve paresis, reported by MADDOX6, patients with metastatic disease of the temporal bone can present hearing loss, aural discharge, vertigo, aural mass, or tinnitus. These symptoms are not pathognomonic and are more related to mastoid infection. All polypoid and granulation tissue in the EAC should then be biopsied and submitted to histological examination since differential diagnoses between metastatic disease and a benign destructive lesion or even a second primary malignancy should be established before planning a therapeutical approach.
In the present case neuroendocrine differentiation was manifested by the histological pattern, the ultrastructural finding of neurosecretory granules, and the expression of neuro-specific enolase. As a clinical and patllological entity SCC still constitute a matter of controversy. Some of them arise from the epithelial basal cells or the subcolumnar reserve cell and are of epithelial origin; others contain argyrophil or argentafin cells and are of neuroendocrine origin or may arise from a stem cell capable of neuroendocrine, epidermoid, and glandular differentiation. Accordingly the widely used old classification scheme of REAGAN et al16 size of the cell is the most important consideration to name a case as small-cell type. Because ó7 considerable overlap in histologic features other authors do not consider small-cell morphology as the most important criterium. Some cases lack demonstrable neurosecretory granules at electron microscopy bus has other features considered as diagnostic, like argyrophilial7.
We have used a very limited panel of primary antibodies in our immunohistochemical study. As in case others 17 have found coexpression of neuroendocrine makers and epithelial cytoskeletal proteins in their cases of SCC of the cervix. The distinction between SCC with neuroendocrine differentiation and SCC of epithelial origin is an important problem from a clinicopathological viewpoint since fomer have a recognized responsiveness to cliemotherapy and radiotherapy. The most valuable finding in recognizing SCC with neuroendocrine differentiation is the ultrastructural demonstration of neurosecretory granulses, since NSE can be found in some cases of nos-SCC18.
ACKNOWLEDGMENTS
Mrs. Iara Flores provided assitance from the Electron Microscopy Unit of the Departament of Pathology.
REFERENCES
1. MORTON, A.L.; BUTLER, S.A.; KIIAN, A.; JOI-INSON, A.; MIDDLETON, P.: Temporal Bone metastases: patliophysiology and imaging. Otolaryngol Head Neck Surg 97: 583-587, 1987.
2. BERLINGER, N.T.; KOUTROUPAS, S.; ADAMS, G.; MAISEL, R.: Patterns of involvement of the temporal bone in metastatic and systemic tnalignaney.l.aryrtgoscope90:619-627, 1980.
3. SADEK, S.A.A.; DIXON, N.W.; HARDCASTLE, P.F.: Metastatic carcinoma of the external auditory meatus secondary to carcinoma of the rectum. A case report. J Laryngol O1ol 97: 459-464, 1983.
4. JAHN, A.F.; FARKASHIDY, J.; BERMAM, J.M.: Metastatic tumors in the temporal bone: a pathophiysiologic study. J Otolaryngol 8: 85-95,1979.
5. FRIEDMAN, L; OSBORN, D.A.: Metastatic tumors in the ear, rose and throat region. J Laringol Otol 79: 576-591, 1965.
6. MADDOX, ILE.: Metastatic tumors of the temporal bane: Ann Otol Rhinol Laringol 76: 149-165,1967.
7. SCHUKNECHT, H.F.; ALLAM, A.F.; MURAKAMI, Y.: Pathology of secondary malignant tumors of /lie temporal bone. Ann Otol Rhinol Laryngol 77:5-22, /968.
8. CRABTREE, J.A.; BRITTON, BA L; PIERCE, M.K.: Carcinoma of the external auditory canal. Laryngoscope 86: 405-415, 1976.
9. FERRON, P.; LeCLERC, J.: Métastase á l'oreille d'un liypenéplr rosne. J Otolaryngol 11: 235-238, 1982.
10. HILL, B.A.; KOHOUT, R.I.: Metastatic adenocarcinoma of the temporal bone. Arch Otolaryngol 102: 568-571, 1976.
11. MERRICK, Y.: Metastatic color adenocarcinoma of the middle ear. Arch Otorhinolaryngol 238: 103-105, 1983.
12. SALDANHA, C.B.R.; BENNETT, J.D.C; EVANS, J.N.G.; PAMBAKIAN, H.: Metastasis to the temporal bone, secondary to carcinoma of the bladder. J Laringol Otol 103: 599-601, 1989.
13. JUNG, T.T.K.; JUN, B.H.; SI IEA, D. et M.: Primary and secondary tumors of the facial nerve. Arch Otolaryngol 112: 1269-1274, 1986.
14. MAFEE, M.F.; VALVASSORI, G.E.; KUMAR, A. et al.: Tumors and tumor-like conditions of the middle ear and mastoid: role of CT and MRI. An analysis of 100 cases. Otolaryngol Clin North Am 21: 349-375, 1988.
15. FUJII, S.; KONISHI, I.; FERENCZY, A. et al.: Small cell undifferentiated carcinoma of the cervix: histology, ultrastructure, and iuununohitochemistry of two cases. Ultrastruct Pathol 10: 337-346,1986.
16. REAGAN, J.W.; MAMONIC, M.S.; WENTZ, W.B.: Analytical study of the cells in cervical squamous cell cancer. Lab Invest 6:241-250, 1957.
17. GERSELL, D.J.; MAZOURAN, G.; MUTCH, D.G.; RUDLOFF, M.A.: Small-cell undifferentiated carcinoma of the cervix. A clinicopathologic, ultrastructural, and immunocytochemical study of is cases. Am J Surg Pathol 12: 684-698,1988.
18. LINNOILA, R.L.: Neuroendocrine differentiation in endocrine and nonendrocrine lung carcinomas. Am J Clin Pathol 90: 641-652,1988.
* Departamento de Patologia da Universidade Federal de Santa Maria, RS.
** Serviço de Patologia do Hospital de Clinicas de Porto Alegre, RS.
Trabalho apresentado do XVIII Congresso Brasileiro de Patologia, Rio de Janeiro, julho de 1990.

Print: ![]()