

Year: 2004 Vol. 70 Ed. 1 - (11º)
Artigo Original
Pages: 66 to 73
 PDF PT
PDF PT Computed tomography in the diagnosis of fenestral otosclerosis
Author(s):
Andy de Oliveira Vicente 1,
Norma de Oliveira Penido 2,
Hélio K. Yamashita 3,
Pedro Luiz Mangabeira Albernaz 4
Keywords: otosclerosis, tomography, x-ray computed, hearing loss
Abstract:
Aim: To identify the main tomographic findings of fenestral otosclerosis and to evaluate the utility of the high resolution computed tomography (HRCT) as a diagnostic method of this osteodystrophy. Study design: A prospective and multicentric study using computed tomography (CT) of the temporal bone. Material and Method: 54 patients with a clinical and surgical diagnosis of otosclerosis. A tomographic analysis has been performed to evaluate the sensitivity of CT scans in diagnosing fenestral otosclerosis, verifying the sites of predilection for otosclerotic lesions, the bilateralism and symmetry of the disease. In this study, 22 patients undergone CT scans of temporal bones have been included in order to investigate other otologic diseases and have constituted the control group. Results: The CT scan was positive in 87% of the patients (77% of the ears). The tomographic findings were mostly bilateral (78,7%) and the fenestral focus more prevalent was the anterior focus to the oval window. Conclusions: The CT scan has shown a high index of positivity and the anterior focus to the oval window has been the most prevalent in this population, and it could be considered the highly suggestive tomographic finding for otosclerosis.
![]()
Introduction
Otosclerosis is a primary focal otic capsule osteodystrophy of unknown etiology that affects genetically predisposed subjects. Most of the time, this condition affects isolated and/or small areas of the otic capsule without causing any symptom. However, in some occasions in which the otosclerotic focus affects the stapedial-vestibular joint and/or the sensorineural components of the inner ear, the disease leads to progressive hearing loss, which can be conductive, mixed or sensorineural 1.
Fenestral otosclerosis is characterized by presence of lesions located predominantly on the lateral wall of the otic capsule, that is, the region of the cochlear and vestibular windows, promontorium and tympanic segment of the Fallopian canal 2, 3, 4.
The introduction of high resolution computed tomography (HRCT) with specific windows for bones and extremely small sections in sophisticated devices, allowed more precise assessment of the temporal bone, enabling the detection of minimal structural abnormalities such as those present at fenestral otosclerosis.
The purpose of the present study was to identify the main tomographic findings of fenestral otosclerosis and to assess the use of HRCT as diagnostic method for this osteodystrophy.
Method
Multicenter prospective radiological study with 54 patients who had otosclerosis and were seen at the Ambulatory of Otorhinolaryngology, Federal University of Sao Paulo - Escola Paulista de Medicina, and Hospital Especializado CEMA. The diagnosis of otosclerosis was collected from clinical assessment (history, ENT examination, pure tone and vocal audiometry, immittanciometry) and surgical confirmation, that is, evidence of stapes fixation without any other evident cause. All patients were submitted to HRCT to study the temporal bones, totaling 108 analyzed ears. We included in the study 22 patients submitted to temporal bone CT scan for the investigation of other otological conditions (pulsatile tinnitus, chronic otitis media - COM, peripheral facial paralysis, petrous apex damage, vestibular Schwannoma, external acoustic canal (EAC) fracture, EAC osteoma, ossicle chain malformation), which comprised the control group.
CT scans were performed at axial and coronal sections of 1-2mm thickness and 1mm increment, with parameters of 1s, 90 to 200mA, 110 to 130kV, matrix 512 x 512 and bone window between 3,500 and 4,000 HU centered at 350 to 650 HU, without venous contrast.
Exams were analyzed and discussed with the radiologist. Otosclerotic lesions were characterized as hypodense areas of the lateral portion of the otic capsule or presence of thickness foci and/or obliteration of oval and round windows. Fenestral otosclerotic foci were identified according to their location in the otic capsule as follows:
1- focus anterior to oval window (FAJO)
1a - no involvement of cochlear endosteal layer (FAJO)
1b -involvement of cochlear endosteal layer (FAJOe)
2 - focus posterior to oval window (FPJO)
3 - focus on round window (FJR)
3a - partial involvement (p)
3b - obliteration (o)
4 - focus on stapes footplate (FPE)
4a - thickness of the whole footplate (e)
4b - anterior portion of the footplate (ant)
4c - posterior portion of the footplate (post)
4d - obliteration of the footplate (o)
5 - focus on facial nerve canal, tympanic segment (FCNFt)
6 - focus on promontorium (Fprom)
The sites of otosclerotic damage reported above were selected according to he histopathological and radiological evidence found in the literature.
During tomographic analyses, CT scan sensitivity for the diagnosis of fenestral otosclerosis and the most frequent locations of otosclerotic lesions were reported. We also assessed bilateral aspects and symmetry of CT findings and efficiency of the section (axial and coronal) to detect focus of fenestral otosclerosis.
To statistically analyze the data, we used marginal homogeneity tests.
Results
The studied population comprised 54 patients (108 ears) with clinical diagnosis of otosclerosis, being that 36 (66.7%) were female and 18 (33.3%) were male subjects. Ages ranged from 15 to 59 years, mean age of 40.8 years. The duration of the disease ranged from 5 months to 30 years, mean duration of 10.7 years. Family history of otosclerosis was negative in 33 patients (61%) and positive in 21 patients (39%).
Fenestral otosclerotic foci were evidenced and distributed based on the frequency of axial and coronal sections on the right (RE) and left ears (LE) (Table 1).
The main characteristics of otosclerotic foci found in this study are described in Tables 2 and 3.
Topography of otosclerotic foci evidenced in the CT scan is represented in Tables 4, 5, 6, 7, 8 and 9.
The test of marginal homogeneity was used to compare the distribution of CT scan findings on both ears and the comparison between distribution of CT scan findings obtained in two different CT scan sections (Tables 10 and 11).
Analysis of the control group
This group comprised 22 patients (31 ears), 12 men (54.5%) and 10 women (45.5%), ages ranging from 14 to 65 years (mean age of 34.7 years).
CT analysis of the control group
There was no CT scan finding suggestive of fenestral otosclerosis in this group of patients.
Discussion
Similarly to the epidemiological data reported in the literature 5-8, we evidenced predominance of female patients in our group with otosclerosis. In our study, the population comprised 36 women (66.7%) and 18 men (33.3%), with a female:male ratio of 2:1. The mean age of patients was 40.8 years and the average duration of the disease was 10.7 years. The control group comprised 12 men (54.5%) and 10 women (45.5%) with mean age of 34.7 years.
The incidence of otosclerosis patients with positive family history ranged from 49 to 58%, according to epidemiological clinical studies reported in the literature 7. In our study, the presence of positive family history for otosclerosis was detected in 39% of the cases. It is difficult to say what is the real incidence of positive family history in otosclerosis, especially because it has variable expression and penetration and it is asymptomatic in most cases 9.
We believe that in order to better understand CT scan findings of otosclerosis, in addition to anatomical knowledge of the temporal bone and training in interpretation of radiological images, it is necessary to have basic understanding of the histopathology of the disease. This is the reason why the otosclerosis topography referred in our study was based on the histopathology and radiology findings reported in the literature.
After the advent of high-resolution computed tomography, the radiological study of otosclerosis became more accurate, and we could detect abnormalities in the region of the oval window or close to it in 80 to 90% of the confirmed surgical cases 10. CT scan precisely shows active and spongiotic otosclerotic lesions, which can be single, multiple or confluent, caused by the process of bone demineralization inherit to this stage of the disease 2, 10, 11, 12, 13, 14.
The identification of inactive or sclerotic otosclerotic foci in the CT scan is more laborious owing to the similarity of density of the lesions and the normal otic capsule. These areas of sclerosis or radiopacity in the CT scan can only be visualized in cases in which the disease causes thickness of the stapes footplate, obliteration of the vestibular and cochlear windows, distortion of the labyrinthic contours and/or intralabyrinthic ossification 10, 15, 16.
In our study, the CT scan demonstrated fenestral otosclerotic foci in 47 patients (87%) or in 84 ears (77.7%) (Tables 1 and 2). In the literature, sensitivity of CT scan in the diagnosis of otosclerosis ranges from 34 to 90%, but in most recent studies, positivity of CT scan was demonstrated in about 90% of the fenestral cases 10, 17, 18. The presence of infra-millimeter lesions and/or inactive otosclerotic foci (sclerotic) in the otic capsule is the main cause of negative CT scan.
Swartz et al. tomographically assessed 35 patients with clinical diagnosis of fenestral otosclerosis and observed positive CT scan in 74.2%, being bilateral findings in 84.6% of these cases 4. In 61.5%, the foci were bilateral and symmetrical. Shin et al. observed that 84.7% of the cases with positive CT scan presented otosclerotic foci in both ears 17. In our sample, CT scan showed bilateral otosclerotic foci in 78.7% of the patients with positive CT scan, being bilateral and symmetrical findings in 38.3% of the cases (Table 3). Bilateral tomographic findings in our study were statistically significant (Table 11).
Shin et al. observed fenestral foci in 74.6% of the CT scan positive cases 17. Veillon et al evidenced foci in the CT scan in 80.9% of the analyzed ears 19. In our cases, 69% of the ears with positive CT scan had fenestral foci. CT scan findings were bilateral in 70.1% of the patients and they were bilateral and symmetrical in 48.38% (Table 4).
Among the fenestral foci, the one that deserves special attention is the focus located in the region anterior to the oval window. In 70 to 95% of the cases, dysplastic lesions (spongiotic, fibrotic and sclerotic) are located in the area next to the ante fenestral fistula, in the angle formed between the stapes footplate, the cochleaform process and the promontorium 1, 3, 5, 8, 9, 20, 21.
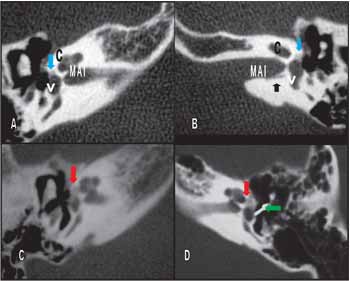
For this reason, we believe that CT scan should be considered the most important test for the radiological diagnosis of otosclerosis and, in our study, the foci in this region were named FAJO ( focus anterior to the oval window) (Figure 1).
Schuknecht and Barber, in a histology study of the temporal bone, observed affection of this region in 95.9% of the patients with clinical otosclerosis and in 51.2% of the cases, FAJO was the only site with otosclerotic lesion 22.
Shin et al 17 observed the presence of otosclerotic focus in this region in 69.8% of the cases and Veillon et al noted, in the CT scan, the presence of FAJO in 68.2% of the cases 19. In our study, we found FAJO in 83.3% of the patients (72.2% of the ears), being that in 33.3% of the patients it was the only tomographic finding (Tables 5 and 6). Such evidence provided support to the relevance of this radiological finding and allowed us to state that during the CT scan of a patient with suspicion of otosclerosis, this site should be investigated in depth.
The region of the round window can also be a target for otosclerotic lesions and according to histology findings described in the literature, this is the second most affected area, whose incidence ranges from 20 to 50% 5, 6, 9, 20, 23.
Swartz et al found non-occlusive otosclerotic foci in the round window of 7.26% of the patients with fenestral otosclerosis studied by CT scan 4. Schuknecht and Barber, by histology analysis of the otosclerotic temporal bones, classified the foci into marginal, bridge-like (lesion that covers the meatus of the round window niche) and obliterative 22. The authors observed the presence of focus in the round window in 26.8% of the cases, being that in 5.48% the foci were obliterative. They referred to the presence of fibrous thickness in the membrane and concluded that the obliterative focus in the round window represented a significant cause of failure in stapes surgeries. Shin et al found in their radiological study with CT scan a prevalence of obliterative foci of round window of 3.2% 17. Veillon et al noticed the presence of round window foci in 9.57% of the 2,215 ears analyzed with CT scan, being that in 0.85% of the cases, this focus occurred as the only labyrinthic capsule lesion 19. The authors also emphasized the importance of detecting round window otosclerotic foci in the CT scan, owing especially to the unsatisfactory surgical results that they can cause.
In our study, we divided the foci of the round window into partial (FJR(p)), with involvement of one segment of the round window niche, and obliterative (FJR(o)), with total involvement and lack of definition of round window niche. FJR was found in 10.2% of the ears, being that FJR(p) was observed in 4.7% and FJR(o) was observed in 5.5% of the ears (Figure 2 and Table 7). We believe it is worth mentioning that even though the evidence of FJR was not frequent in our patients, it should be addressed since it can produce disappointing surgical results, especially concerning evidence of FJR(o). Therefore, the CT scan findings of FJR(o) can contribute to the assessment of surgical feasibility.
The evidence of focus in the stapes footplate by the CT scan is undoubtedly a useful piece of information, especially in patients selected for stapedotomy and/or stapedectomy. The presence of footplate thickness and obliteration are inappropriate conditions and very challenging affections for the current otological surgeons, who normally conduct fewer surgeries like that. Garcia-Ibanez and Iurato, through the analysis of 78 footplates excised during stapedectomy, observed that the anterior region of the footplate was the most affected area (52.6%) by the otosclerotic lesions 24. The authors found thickness of the whole footplate, without obliteration, in 19.2% of the cases and in 5.12% of the cases it was in the posterior portion. Obliterative otosclerosis can be defined as thickness of the stapes footplate in which the oval window is filled with otosclerotic lesion of variable proportions and annular ligament is completely involved, preventing the delineation of the margins of the vestibular window. According to the literature, the incidence of obliterative otosclerosis ranges from 1 to 33% 25. Veillon et al. considered footplate thickness in cases in which thickness was higher than 0.6mm in the CT scan and they found in their sample 12.7% of this finding in the analyzed ears 19. Shin et al found an incidence of 4.8% of thick footplate in the CT scan analysis 17. By means of these concepts, we divided stapes footplate (FPE) into uniform thickness of the footplate (FPE(e)), anterior footplate thickness (FPE(ant)), posterior footplate thickness (FPE(p)) and footplate obliteration (FPE (o)). In 23% of the studied ears, we evidenced FPE; FPE (e) was observed in 13.8%, FPE (ant) in 4.6%, FPE (o) in 4.6% and FPE(p) in 0.92% of the ears (Figures 3 and 4) (Tables 8 and 9). Obliteration of one or both labyrinthic windows was found in 9.25% of our patients, being that FPE(o) was detected in 5.55 % of the cases, all of them with advanced disease. One patient (1.85%) in our sample presented contiguous obliterative foci in the oval and round windows in one ear (Figure 3F). In this case in special, the surgery was contraindicated owing to the severity of the disease demonstrated by CT scan. The contralateral ear had been submitted to previous stapedotomy. Some histopathology studies described this confluence between the oval and round windows foci, especially in more severe cases of the disease 5, 9, 22.
Another fenestral otosclerotic focus found in our sample was the focus on the cochlear promontorium (Fprom), in the region comprised between both labyrinthic windows (Figures 5a and b). Swartz et al. detected this CT scan finding in 40% of the patients with fenestral otosclerosis. In our study, we managed to evidence Fprom in 3.7% of the patients (Table 1). In such cases, there was concomitant presence of stapes footplate thickness.
The focus affecting facial nerve canal in the tympanic segment FCNFt was evidenced in 7.4% of the patients (6.5% of the ears) in our sample (Figure 5) (Table 1). We believe that this focus is resultant from the expansion of FAJO towards the auditory tube. Takasaki et al. found histopathology evidence of this type of lesion 21.
The focus of the posterior region to the oval window (FPJO) was not visualized in our study. In the radiology literature, such topography was not commented, despite the fact that histological evidence of this lesion had been described in up to 11% of the cases 7, 26.
As to efficacy of CT scan sections, axial sections proved to be more reliable to diagnose FAJO, presenting statistically significant results. In other topographies, there was no statistically significant difference between both incidences (Table 10). Therefore, we can infer that axial sections are essential in the radiological approach of patients with suspicion of fenestral otosclerosis. Coronal section seemed to be useful for the detection of thickness and obliterations of the oval and round windows, Fprom and FCNFt. In our opinion, another application of the test is the assessment of the dimensions of the oval window niche and its correlation with the facial nerve.
It is important to emphasize that despite the fact that CT scan provides valuable information, it does not replace histopathological evidences in otosclerosis, which makes histology the main exam for the definite diagnosis of this osteodystrophy. We expect that technological advances in imaging will provide greater diagnostic sensitivity in the future, especially concerning sclerotic lesions of this disease.
Conclusions
Computed tomography scan was effective in the diagnosis of fenestral otosclerotic foci, presenting high level of positive responses.
CT scan findings were bilateral in most patients and such evidence was statistically significant.
FAJO was the predominant focus in this population and it can be considered a highly suggestive CT scan finding of otosclerosis.
Computed tomography proved to be extremely useful in preoperative assessment of patients with otosclerosis.Table 1 - DISTRIBUTION OF OTOSCLEROTIC FOCI ON THE RE AND LE AT AXIAL AND CORONAL SECTIONS.
Ciscan in each ear
Table 2- ASSESSMENT OF POSITIVE AND BILATERAL PRESENCE OF OTOSCLEROTIC FOCI BY COMPUTER TOMOGRAPHY.
Table 3 - CHARACTERISTICS OF OTOSCLEROTIC FOCI FOUND BY COMPUTED TOMOGRAPHY.
Table 4 - CHARACTERISTICS OF FENESTRAL FOCI
Table 5 - FREQUENCY OF FAJO IN THE STUDIED POPULATION.
Table 6 - FAJO CHARACTERISTICS.
Table 7 - CHARACTERISTICS OF FOCUS ON THE ROUND WINDOW.
Table 8 - DISTRIBUTION OF FPE ON THE RIGHT EAR OF THE STUDIED POPULATION.
Table 9 - DISTRIBUTION OF FPE ON THE LEFT EAR OF THE STUDIED POPULATION.
Table 10 - DESCRIPTIVE LEVELS OF COMPARISON BETWEEN FINDINGS OF CT SCAN SECTIONS (A / C).
Legend: A=axial ; C=Coronal
*Marginal homogeneity test
Table 11 - ASSESSMENT OF BILATERAL CHARACTERISTIC OF TOMOGRAPHIC FINDINGS.
*Marginal homogeneity test
There was no statistically significant difference concerning positive response of CT scan between the ears, that is, findings were bilateral in most cases.
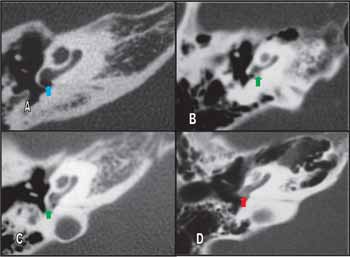
Figure 1(A-D): Temporal bone computed tomography in axial sections evidencing focus anterior to the oval window (FAJO). A and B: FAJO of small dimensions, without involving the endosteum of the cochlea (blue arrows). Black arrow in B: singular nerve canal;
C and D: FAJO involving the cochlea endosteum (red arrows). Note the presence of stapedotomy prosthesis (green arrow).
MAI = inner acoustic canal; C = cochlea.
Figure 2(A-D): Temporal bone computed tomography in axial sections at the level of the round window (JR). A: niche of normal JR (blue arrow); B and C: foci with partial involvement of round window (FJR(p)) (green arrows); D: obliteration focus on the round window (FJR(o)) (red arrow).
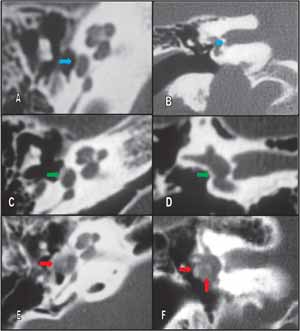
Figure 3(A-F): A: Temporal bone computed tomography in axial sections at the level of the oval window evidencing normal footplate (blue arrow); B: coronal section CT scan, demonstrating normal footplate (blue arrow); C: axial section CT scan evidencing thickness of the footplate (FPE(e)) (green arrow); D: Coronal section CT scan evidencing FPE(e) (green arrow); E: Axial section CT scan evidencing diffuse lesion causing obliteration and loss of oval window definition FPE(o) (red arrow) ; F: Coronal section CT scan demonstrating confluent obliterative foci in both labyrinthic windows (red arrows).
Figure 4 (A-B): A: Temporal bone computed tomography in coronal sections at the level of the oval window, evidencing FAJO and thickness of the anterior region of the footplate (blue arrow); B: axial section CT scan evidencing FAJO (green arrow) and thickness of the posterior portion of the footplate (red arrow).
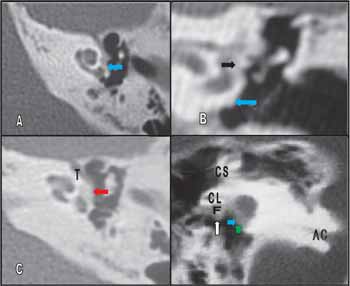
Figure 5(A-D) - Temporal bone computed tomography showing areas of hypotransparency in the promontorium and facial nerve canal; A: axial section CT scan demonstrating hypotransparency focus on the cochlear promontorium (blue arrow); B: Coronal section CT scan evidencing irregularity of the promontorium contour (blue arrow) and stapes footplate thickness (black arrow); C: Axial section CT scan demonstrating FAJO progressing towards the tympanic segment of the facial nerve (red arrow); D: Coronal section CT scan evidencing obliteration of the oval (blue arrow) and round (green arrow) windows and involvement of the facial nerve canal (tympanic portion) (white arrow). F: facial nerve; CL: lateral semicircular canal; CS: superior semicircular canal; AC: cochlear aqueduct; T: tympanic segment of the facial nerve (in B).
References
1- Glasscock ME, Shambaugh GE. Surgery of the Ear. 4th ed, Philadelphia: WB Saunders, p.371-387,1990.
2- Valvassori GE: Imaging of the Otosclerosis. Otolaryngol Clin North America 1993;26(3): 359-371.
3- Rovsing H. Otosclerosis fenestral and cochlear. Radiologic Clinics of North America 1974;12(3):505-515.
4- Swartz JD, Faerber EN, Wolfson RJ, Marlowe FI. Fenestral Otosclerosis: significance of preoperative CT evaluation. Radiology 1984;151(3):703-707.
5- Nager GT. Histopathology of otosclerosis. Arch Otolaryng 1969;89:157-179.
6- Lindsay JR. Histopathology of otosclerosis. Arch Otolaryngol 1973;97:24-29.
7- Schucknecht HF: Pathology of the ear. 2nd ed., Lea & Febiger, Philadelphia, 1993, p.365-379.
8- Niedermeyer HP, Arnold W. Etiopathogenesis of otosclerosis. ORL 2002;64:114-119.
9- Guild SR. Histologic otosclerosis. Ann Otol Rhinol Laryngol 1944; 53:246-66.
10- Berrettini S, Ravecca F, Volterrani D, Forli F, Boni G, Neri E, Francheschini SS. Single Photon Emission Computed Tomography in Otosclerosis: Diagnostic accuracy and correlation with age, sex, and sensorineural involvement. Otol Neurotol 2002;23:431-438.
11- Maffe MF, Henrikson GC, Deitch RL. Use of CT in stapedial otosclerosis. Radiology 1985;156:709-14.
12- Maffe MF, Valvassori GE, Deitch RL. Use of CT in cochlear otosclerosis. Radiology 1985a;156:703-8.
13- Shin YJ, Deguine O, Sevely A, Manelfe CL, Fraysse B. Pure Sensorineural hearing loss and otosclerosis. Rev Laryngol Otol Rhinol 2000;121(2):45-47.
14- Swartz JD, Mandell DW, Wolfson RJ, Marlowe FI, Popky GL, Silberman HD, Wilf H, Swartz NG, Berger AS. Fenestral and cochlear otosclerosis: Computed Tomographic evaluation. Am J Otol 1985b;6(6):476-481.
15- Phelps P. The basal turn of the cochlea. The British Journal of Radiology 1992;65:370-374.
16- Ruckenstein MJ, Rafter KO, Montes M, Bigelow DC. Management of far advanced otosclerosis in era of cochlear implantation. Otol Neurotol 2001;22:471-474.
17- Shin YJ, Fraysse B, Deguine O, Cognard C, Charlet JP, Sévely A. Sensorineural hearing loss and otosclerosis: a clinical and radiologic survey of 437 cases. Acta Otolaryngol 2001a;121:200-204.
18- Shin YJ,Calvas P,Deguine O,Charlet JP,Cognard C,Fraysse B. Correlations between computed tomography findings and family history in otosclerotic patients. Otol Neurotol 2001b;22:461-464.
19- Veillon F, Riehm S, Emachescu B, Haba D, Roedlich Marie-Noëlle, Greget M, Tongio J. Seminars in Ultrasound, CT, and MRI 2001;22(3) 271-280.
20- Nager GT. Sensorineural deafness and otosclerosis. Ann Otol Rhinol Laryngol 1966;75: 481-511.
21- Takasaki K, Sando Isamu, Hirsch BE. Loss of facial nerve fibers in a case o otosclerosis.
Am J Otol 2000;21:766-768.
22- Schuknecht HF, Barber W. Histologic variants in otosclerosis. Laryngoscope 1985;95:1307-1317.
23- Linthicum FH Jr. Histopathology of otosclerosis. Otolaryngologic Clinics of North America 1993;26(3):335-352.
24- Garcia-Ibañes JL, Iurato S. Anatomical study of the otosclerotic stapedial footplate. Arch Otolaryng 1969;90:410-417.
25- Ayache D, Sleiman J, Plouin-Gaudon I, Klap P, Elbaz P. Obliterative otosclerosis. Journal of Laryngology and Otology 1999;113:512-514.
26- Merchante SN, Incesulu A, Robert J.G, Nadol JB Jr. Histologic studies of the posterior stapediovestibular joint in otosclerosis. Otol Neurotol 2001;22:305-310.
1 Otorhinolaryngologist, Master studies under course, Discipline of Otorhinolaryngology, UNIFESP - EPM, Preceptor of the Residence in Otorhinolaryngology, Hospital Cema.
2 Affiliated Professor of Otorhinolaryngology, UNIFESP-EPM.
3 Joint Professor, Department of Imaging Diagnosis, UNIFESP-EPM.
4 Faculty Professor, Discipline of Otorhinolaryngology, UNIFESP-EPM.
Study conducted in the Ambulatory of Otorhinolaryngology, Federal University of Sao Paulo - Escola Paulista de Medicina, and Hospital Cema.
Address correspondence to: Andy de Oliveira Vicente - Rua Guaimbé 465, apt 10, CEP- 03118-030 - Sao Paulo SP.
Tel: (55 11) 6605-3929 - e-mail: andyvicente@uol.com.br
Article accepted for poster presentation at III Congresso Triológico de Otorrinolaringologia.

Print: ![]()