

Year: 2000 Vol. 66 Ed. 6 - (17º)
Relato de Casos
Pages: 687 to 690
Facial Pain by Ectopic Tooth.
Author(s):
Marconi T. Fonseca*,
Marcos A. C. de Lacerda**,
Sânzio T. Valle**,
Raquel T. Silva***.
Keywords: ectopic tooth, facial pain, maxillary sinus
Abstract:
Ectopic toot in paranasal sinus is a extremely rare event. We report the case of a female pacient with cronic facial pain of unknown cause, that was found the presence of an impacted tooth in maxillary sinus. Comments and review of literature also are in this paper.
![]()
INTRODUCTION
Members of more developed societies show disproportion between size of mandible and teeth. This imbalance generated by the incompatibility between the existing space and the size of teeth favors the inclusion or retention of the tooth inside the bone tissue (Howe, 1960).
The presence of tooth in the nasosinusal tract may be either an ectopic eruption or the result of mobilization due to dental extraction or trauma.
It may be present in various places, such as orbit, nasal cavity, maxillary sinus, palate, mandible condyle, coronoid process or through the skin9, 3, 6.
An ectopic tooth may be deciduous, permanent or supernumerary, which is the most common presentation6.
The incidence of supernumerary tooth ranges from 0.1% to 1% in the population, and out of these total, only a small percentage develop in the nasal-sinusal region3, 6, 11, 13.
Its embryogenesis is still not clear and some authors believe that there is possibly a family trend in its occurrence13.
Facial pain is a possible symptom caused by the presence of an ectopic tooth in the nasal-sinusal tract; whose mechanism we shall discuss next.
CASE REPORT
Patient M. L. P. A., female and aged 49 years, came to the Service of Otorhinolaryngology on 8/4/97 complaining of facial pain for approximately 1 year, on nasal-frontal area. The pain had moderate intensity and frequency, normally relieved by common analgesics. She reported worsening of pain in previous months, extending onto the maxillary region.
At oropharyngoscopy, we observed absence of all teeth, which had been previously extracted, but there was no history of dental dislocation. There were no further findings in the ENT exam.
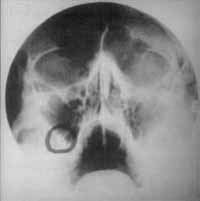
We ordered paranasal sinus x-ray and detected a small radiopaque image close to the lateral-inferior angle of right maxillary sinus. Next, we ordered CT Scan of paranasal sinuses at coronal and axial sections and it showed an oval image of bone density, measuring 15x 4mm, located on the posterior-inferior-lateral wall of right maxillary sinus, part projected into the sinus and part into the pterygoid-palatine fossa, suggestive of ectopic tooth.
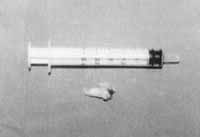
We indicated surgical removal of lesion and it was conducted on 3/19/98, with Caldwell-Luc surgery, under general anesthesia. The complete removal of the surgical piece was performed and we confirmed the diagnosis of ectopic premolar tooth, measuring 1.6cm. The surgery was uneventful and the patient was discharged one day after surgery.
In the first pre-op visits, the patient reported that she did not have facial pain anymore; the last visit was doneth moths after the surgery and since the patient was asymptomatic,she was finally discharged.
Photo 1.
Anatomical pathologic analysis of the surgical piece revealed characteristics of regular teeth.
DISCUSSION
Since it is a rare event, the literature does not have many studies on the topic, but the most complete one was conducted by Smith et al. (1979) who presented 27 well documented cases. This lack of evidence contributes to the existence of doubts concerning the topic, especially about the origin. Some theories have been described: tooth dislocation by trauma of the oral cavity or cyst; developmental disorder or incomplete fusion, such as in cleft palate; maxillary infection, both odontogenic and rhinogenic; genetic factors; space restrictions due to excessive dentition, persistent deciduous teeth or exceptionally dense bone9, 3.
The hypothesis of space restriction would be the most suitable to explain this case.
Clinical history and physical exam exclude the other hypotheses, including the one of dislocation by trauma, despite the fact that the patient had all teeth extracted. She did not report any events or complications during extractions; moreover, in the case of dislocation by trauma the most commonly affected teeth, because of anatomical position, are the 1st molar and the 2nd molar4, 8, 12, 7.
The ectopic tooth removed in this case was a pre-molar located in an area innervated by the maxillary branch of the trigeminal nerve (V pair)5. We believe that the pain was due mostly to irritation or distention of the periosteum of the maxillary sinus, rather than irritation of sinusal mucosa, wich is little sensitive to pain stimuli2.
Photo 2.
Other symptoms, such as nasal obstruction, epistaxis, rhinorrhea and cascomia, are more common when the ectopic tooth has intranasal location. Intranasal or intrasinusal ectopic teeth may be totally asymptomatic and they may be casually identified during a clinical or radiological exam9, 3.
The diagnosis should be confirmed by radiological exam and paranasal sinus CT scan is the most suitable exam, not only for diagnostic purpose, but also for surgical management of the case.
Differential diagnosis should be made with exostosis, foreign body, tumors and bone sequestrum9, 3, 10. The presence of nasal-sinusal tooth may lead to complications, such as chronic sinusitis, aspergillosis and oroantral fistula3.
In all studies reviewed by us, there was agreement as to surgical treatment approach and Caldwell-Luc surgery is the best approach to remove an ectopic tooth.
FINAL COMMENTS
Facial pain and headaches are very common complaints in the ENT practice, and maybe that is why the risk of a oversimplification of causal diagnosis is higher, associating these symptoms to more frequent pathologies, such as sinusitis or migraine.
Careful anamnesis and complete ENT exam are important to help avoiding these misdiagnoses. By doing so, we will diagnose and treat other less frequent causes, such as septal impactation, occlusive or TMJ disorders, exostosis and ectopic tooth.
Photo 3.
Photo 4.
REFERENCES
1. BODNER L., TOVI F., BAR. ZIU J. - Teeth in the maxillary Sinus-imaging and management J. Laryngol. Otol., 111: 820-824.
2. CERVILLA F. F., JUAN M. C. - in Barcells Riba M. - Cefaleas y Algias Craneofaciales en Oto Neuro Oftalmologia. Ponencia do VI Cong. Nac. Soc. Espanola Oto Neuro Oftal. 1994. Ed. Mayo - Barcelona: 145-158.
3. EL-SAYED, Y. - Sinonasal Teeth. J. Otolaryngol., 24 (3):180-183, 1995.
4. JONES, E. H.; STEEL, J. S. -Roots in Maxillary Sinus. Australian Dental L. 14: 08-11. 1969.
5. LEVINE, H. L. - Otorhinolaryngologic Causes of Headache. Med. Clin. North Am., 75 (3): 677-692, 1991.
6. NASTRI, A. L.; SMITH, A. C.- The Nasal Tooth. Case Report. Australian Dental J., 41(3): 176-177, 1996.
7. OBERMAN, M.; HOROWITZ, I.; RAMON, Y. - Accidental Displacement of impacted maxillary third molars. Int. J. Oral Maxillofac. Surg., 15: 756-758, 1986.
8. SIMS. M. A. P. T. -A Dental Root in the Ostium of The Maxillary Antrum. Brit. Assoc. Oral Maxillo fac. Surg., 23: 67-73, 1985.
9. SMITH, R. A, GORDON, N. C, DELUCHI, S. F. - Intranasal Teeth. Oral Surg. Oral Med. Oral Pathol., 47(2):120-122,1979.
10. SPENCER, M. G., COULDERY, A. D.-Nasal Tooth. J. Laryngol. Otol., 99.1147-1150, 1985.
11. THAWLEY, S. E.; LAFERRIERE, K. A-Supernumerary Nasal Tooth. Laryngoscope, 87: 1770-1773, 1977.
12. VOW WOWERN, N. - Oroantral Communications and displacements of roots into the maxillary sinus: a Follow-up of 231 cases. J. Oral. Surgery, 29 (17): 622-627, 1971.
13. WINTER, G. B. - Hereditary and Idiopathic Anomalies of Tooth Number, Structure and Form. Dental. Clin. North Am., 13 (2): 355-373, 1969.
* Coordinator of the Service of Otorhinolaryngology at Hospital Socor.
** Assistant Physician of the Service of Otorhinolaryngology at Hospital Socor.
*** Intern Physician of the Service of Otorhinolaryngology at Hospital Socor.
Study conducted at Hospital Socor - Belo Horizonte/ MG.
Address for correspondence: Dr. Marconi Teixeira Fonseca - Rua juiz de Fora, 115/1301 - 30180-060 Belo Horizonte/ MG
Tel: (55 31) 295-5556 - Fax (55 31) 295-1941 - E-mail: otologic@joinnet.com.br
Article submitted on December 1, 1999. Article accepted on January 19. 2001.


Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial