

Year: 2000 Vol. 66 Ed. 6 - (16º)
Relato de Casos
Pages: 680 to 685
Auditory Neuropaty: Case Report.
Author(s):
Cristiana R. B. Abe*,
Luciana P. Garolla*,
Sanyelle S. Pinheiro**,
Marisa F. Azevedo***,
Clara R. B. De Ávila****.
Keywords: neuropathy, hearing
Abstract:
This article relates a case of auditory neuropathy in a young patient, who have received early intervention.
![]()
INTRODUCTION
In recent years, thanks to the introduction of evoked otoacoustic emissions (EOAE) in the battery of audiological exams, a new clinical group of patients started to be identified with the diagnosis of auditory neuropathy 6, 1 0.
Auditory neuropathy is identified by the presence of EOAE and/or cochlear feedback and absence of ABR (auditory brainstem responses) potentials, showing, respectively, normal functioning of external ciliary cells and abnormal neural synchrony 6. 10.
Subjects who have auditory neuropathy may experience difficulties to understand speech, especially in the presence of background noise. They have difficulties to follow a normal conversation, requiring the support of orofacial reading 6. 10.
The purpose of the present article was to report the case of a child with auditory neuropathy diagnosed in the first months of life at the Follow-up multidisciplinary program of high risk neonates at Hospital São Paulo, Universidade Federal de São Paulo (UNIFESP), and submitted to speech and hearing therapy.
REVIEW OF LITERATURE
Auditory neuropathy is characterized by the following findings6, 10:
o It may manifest alone or as part of a generalized neuropathological process.
o Hearing levels may be either normal or altered, in different degrees and configurations of hearing losses.
o Speech recognition is impaired, especially in the presence of noise.
o Normal functioning of external ciliary cells, that is to say, EOAE and cochlear feedback are normal.
o Absence of efferent suppression of EOAE in the presence of ipsi or contralateral acoustic stimulation.
o Ipsi and contralateral stapedial reflexes are absent.
o Abnormal neural function, that is to say, ABR is absent or severely impaired.
o Incompatibility between pure tone thresholds and EOAE, revealing the need for further investigation.
o Imagining techniques (magnetic resonance and computed tomography) are normal.
o Diverse etiology, such as peri-natal events and genetic factor (for example, types I and II Charcot-Marie-Tooth syndrome or Guillain-Barré syndrome).
Subjects with auditory neuropathy initially present history and performance in exams similar to those of subjects with central auditory processing disorder. However, the results of electrophysiological measures reveal more peripheral alter ations in auditory neuropathy, which may be located in the internal ciliary cells, tectorial membrane, synapse between internal ciliary cells and auditory nerve, neurons of spiral ganglion, fibers of the acoustic nerve and/or related to a biochemical abnormality of neurotransmitters6, 10.
Auditory rehabilitation of such patients requires a different approach from the one adopted for regular peripheral hearing loss6.
Normally, patients benefit very little from the use of hearing aids. Some patients believe that FM systems (system to aid interpersonal communication and media3) are useful because they improve signal/noise ratios. If amplification will be provided, it is recommended the use of a small gain hearing aid with WDRC compression (dynamic compression) in order to minimize harmful events on the otoacoustic emissions6.
Patients diagnosed as having a severe/profound loss, who show little or no benefit from the use of hearing aids, may have auditory neuropathy and deserve to go through further diagnostic investigation, including EOAE and ABR exams, which are sensitive tests to cochlear and neural functions.
Events during the neonatal period, such as hyperbilirrubinemia, are among the etiological factors of auditory neuropathy6. Therefore, it is suggested that we conduct as early as possible an investigation with EOAE, ABR and behavioral observation to sound stimuli in neonates who have these risk indicators for hearing disorders, in order to enable fast intervention and better prognosis.
CASE REPORT
E. C. G., female 2-years and 11-month old Caucasian patient, born in Sao Paulo/ SP. She was the 6th baby of an issue of four. The mother had had two stillborn babies because of dehydration.
The patient was born in term (gestational age of 37 1/ 7 weeks - Capurro), normal delivery, weighting 3,185 grams. She had hemolytic anemia because of RH incompatibility. She was submitted to phototherapy and to two exsanguination transfusions. She took ototoxic drugs for 14 days (Amicacyn and Vancomycin). She remained for 18 days in the incubator.
At 1month of age, the patient was submitted to behavioral screening conducted by the Discipline of Hearing Disorders, together with the Discipline of Pediatrics at UNIFESP. In this screening, the child showed absence of cochlear-palpebral reflex at 100dBSPL; she was then referred to a complete set of audiological exams in the Service of Child Audiology.
In the audiological assessment, the patient showed the presence of transient EOAE and absence of ABR bilaterally at 130 dBSPL, maintaining absence of reflex for more intense sounds, compatible with the diagnosis of auditory neuropathy.
Since then, the patient has been followed by a multidisciplinary team of speech and hearing pathologists, otorhinolaryngologist, pediatrician and neurologist. In the Out-Patient Service of Human Communication Disorders and Audiology Disorders we conducted periodical hearing assessments and family counseling about hearing, speech and language aspects.
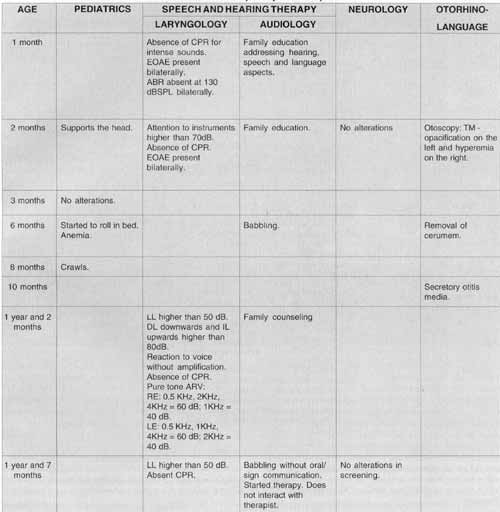
Chart 1 describes the multidisciplinary follow-up of the patient.
CHART 1 - ECG Multidisciplinary Follow-up
CHART 2 - Risk indicators associated with hearing disorder7.
DISCUSSION
The prevalence of hearing disorders in the, cases of uneventful newborns (1:1,000) increases to 10:1,000 if there are risk factors for hearing loss7.
The data registered in the hospital file of the patient enabled her to be classified as high risk for hearing disorder, according to the joint Committee on Infant Hearing 1994 (Chart 2).
Since 1987, we have developed a program of hearing screening at UNIFESP aiming at early identification of peripheral and central hearing losses, in order to enable immediate management. The protocol of hearing screening includes cochlear-palpebral reflex higher than 100dBSPL, and transient otoacoustic emissions2. This protocol was recommended by the Brazilian Committee on Hearing Losses in Children5.
The studied child was submitted to complete audiological assessment because she showed absence of cochlear-palpebral reflex during the hearing screening. Since cochlear-palpebral reflex is present in more than 90% of hearing newborns1, its absence suggested the presence of hearing disorder.
In recent years, due to technological advancement, measures of transient EOAE were included in the batteries of children hearing tests9, as an objective method to assess the presence of external ciliary cells in the cochlea. Transient EOAE present in our patient suggested preserved cochlear function.
ABR is especially useful to identify abnormalities of neural synchrony, from the distal portion of the auditory nerve to the brainstem4, 8. The studied child had absence of responses at 130dBSPL in the test.
The case presented all characteristics described in the literature and considered essential for the diagnosis of auditory neuropathy - present EOAE and absent ABR6, 10. The diagnosis confirmed in the first 2 months of life enabled early intervention, family counseling and follow-up of speech and language development.
Recent studies11 have shown the relevance of speech and hearing intervention before 6 months of age because of plasticity and maturation of central nervous system for the prognosis of language development. Children who were diagnosed as having a hearing disorder in the first semester of life had language, hearing and speech developments much better than those diagnosed after this period. In addition, owing to intervention before 6 months of life, family dynamics is preserved, reducing maternal stress and the guilty parents normally feel if diagnosis is too much delayed11.
In fact, speech and hearing therapy started in the first year of life has enabled progression of linguistic and hearing skills of the child, as we may observe in Chart 1.
FINAL COMMENTS
It is paramount to conduct the complete battery of audiological tests in high risk newborns, including EOAE, ABR and behavioral assessment.
This case reinforced the importance of multidisciplinary assessment performed in the nursery, because we identified earlier a case of auditory neuropathy, allowing multidisciplinary intervention in the first year of life, a critical period for maturation and plasticity of central nervous system.
REFERENCES
1. AZEVEDO, M. F.; VIFIRA R. M. & VILYEARVA T. C. P. - Desenvolvimento auditivo de crianças normais a de alto risco. Sao Paulo, Plexus, 1995.
2. AZEVEDO, M. F. - Avaliação audiológica no primeiro ano de vida. In: LOPES F°, O. - Tratado de fonoaudiologia. São Paulo, Roca, 1997, p.239 - 264.
3. BONALDI, L. V. & ALMEIDA, K. - Equipamentos a sistemas auxiliares para o deficiente auditivo. In: ALMEIDA, K. & IORIO, M. C. M. - Prótese auditivas: considerações teóricas a aplicações clínicas. São Paulo, Lovise, 1996, p. 106 - 217.
4. CASTRO Jr, N. P. & FIGUEIREDO, M. S. - Audiometria eletrofisiológica. In: BASSETTO, M. C. A.; BROCK, R. & WAJNSZTEJN, R. - Neonatologia: um convite a atual do fonoaudiologica. Sao Paulo, Lovise, 1998, p. 201 - 220.
5. COMITE BRASILEIRO SOBRE PERDAS AUDITIVAS NA INFANCIA - Recomendação 01/99. Jornal do CFFA, 5: 3 - 7, 2000.
6. HOOD, L. J. - Auditory neuropathy: what is it and what can we do about it? Hear J., 51 (8): 11 - 18, 1998.
7. JOINT COMMITTEE ON INFANT HEARING - Position Statement 1994. Pediatrics, 95(1): 152 - 156, 1995.
8. MATAS, C. G.; FRAZZA, M. M. & MUNHOZ, M. S. L. -Aplicação do potencial auditivo de tronco encefálico em audiologia pediátrica. In: BASSETTO, M. C. A.; BROCK, R. & WAJNSZTEJN, R. - Neonatologia: um convite a atuação fonoaudiológica. São Paulo, Lovise, 1998, p. 301 - 310.
9. PARRADO, M. E. S. - Emissões otoacusticas em recém-nascidos. In: BASSETTO, M. C. A.; BROCK. R. & WAJNSZTEJN, R. - Neonatologia: um convite a atua(7ao fonoaudiologica. Sao Paulo, Lovise, 1998, p. 295 - 300.
10. STARR, A.; PICTON, T. W.; SININGER, Y.; HOOD, L. J.; BERLIN, C. I. - Auditory neuropathy. Brain, 119: 741 - 753, 1996.
11. YOSHINAGA - ITYEAR, C.; SEDEY, A. L.; COULTER, D. K. & MEHL, A. L. - Language of early and later identified children with hearing loss. Pediatrics, 102: 1161 - 1171, 1998.
* Speech and Hearing Pathologist, Specialist in Human Communication Disorders - Speech Disorders and Audiology, with Universidade Federal de São Paulo.
** Speech and Hearing Pathologist, Specialist in Human Communication Disorders - Speech Disorders, with Universidade Federal de São Paulo.
*** Speech and Hearing, Pathologist. Joint Professor of the Discipline of Hearing Disorders of the Department of Otorhinolaryngology and Human Communication Disorders at Universidade Federal de São Paulo.
**** Speech Pathologist. Joint Professor of the Discipline of Human Communication Disorders of the Department of Otorhinolaryngology and Human Communication Disorders at Universidade Federal de São Paulo.
Affiliation: Hospital São Paulo, Universidade Federal de Sao Paulo.
Address for correspondence: Cristiana Rodrigues Belo Abe - Rua Amadeu Gamberim, 208 - 08010-110 São Paulo/ SP - Tel: (55 11) 6137-7225
Article submitted on September 16, 1999. Article accepted on September 28, 2000.
Print: ![]()
All rights reserved - 1933 /
2026
© - Associação Brasileira de Otorrinolaringologia e Cirurgia Cérvico Facial