

Year: 2000 Vol. 66 Ed. 6 - (12º)
Artigos Originais
Pages: 652 to 658
Misdiagnosis of Hearing Loss Due to Ear Canal Collapse.
Author(s):
Sofia Toniossso*,
Maria C. Redondo**,
Otacílio Lopes Filho***.
Keywords: audiologyc thresholds, external acustic meatus, mensuring
Abstract:
Introduction: Collapse of the external auditory meatus during audiometry can lead to spuriously increased hearing thresholds being obtained, particularly at high frequencies, by pressure exerted on the pinna during audiometryc testing. The pressure of the earphone against the pinna may result in the partial closure or complete collapse of the external auditory meatus during audiometry. To avoid such errors, na effective method has to be used to eliminate outer ear closure to allow sound to reach" the tympanic membrane during tonal audiometry. Material and methods: In a sample of 47 patients, we demonstraded best. results after using a small piece of polyethylene tubbing inserted in the canal to avoid the collapse of the ear canal.
![]()
INTRODUCTION
Throughout the previous 30 years, many researchers published studies showing that the reduction in sensitivity of air conduction may be caused in some subjects by the pressure exerted by the earphones on the pinna during audiological assessment. This pressure against the pinna may lead to total or partial closure of the external ear canal.
The identification of this condition, under the responsibility of the audiologist and otorhinolaryngologist, has been done owing to:
o Inconsistency in the collection of inter and intra-test hearing thresholds (similar to those found in patients who have suspicion of non-organic loss).
o Incompatibility between data found in pure tone audiometry and in immitanciometry (air-bone gap and presence of stapedial muscle reflex).
o Discrepancy among hearing thresholds and subjective impression that the examiner has during conversation.
According to some studies, the reduction of threshold resultant from this condition may vary from 5 to 50dbHL and the frequencies involved are equally variable, although it is more generally observed in high frequencies.
Previous studies do not suggest prevalence of sex, race or ear.
Many author's reported the most frequent occurrence of ear canal collapse in patients over 60 years of age. However; they pointed out that it may happen in any age range.
Misdiagnosis because of failure to identify the real nature and/or degree of hearing loss may result in adoption of incorrect management, such as exclusion of a worker from his workplace, fitting of hearing aids or even indication of an unnecessary surgery.
The purpose of the present study was to demonstrate the possible variations in hearing thresholds that may be produced by a collapsed ear canal and, consequently, raise awareness of professionals (audiologists and otorhinolaryngologists) to this phenomenon, preventing misdiagnosis and mistaken management approaches.
REVIEW OF LITERATURE
One of the first studies concerning this topic was made by Ventry et al., in 196120. These authors reported their findings in 2 male patients who showed functional hearing loss due to inconsistency of responses during pure tone audiometry. An inspection of the external ear canal showed that the pressure made by the earphones could have caused a collapse of the ear canal. In order to avoid collapse during the exam, small plastic tubes were inserted in the ears. Using this procedure, the authors had an improvement of hearing thresh olds of 15 to 30dBHL, both for pure tones and speech discrimination.
In a 13-year period, Hildyard and Valentine, in 19628, identified 48 cases in which they had observed ear canal collapse. The authors described an incidence of about 4%. These authors believed that the presence of collapse is not necessarily revealed by inter and intra-exam inconsistency and suggested that tests with tune fork, and inspection of auditory external canal were necessary to validate the audiological results.
Chandler, in 19643, investigated the effects of occlusion of external ear canal and concluded that high frequencies are the most affected, showing drop of thresholds of 40dBHL in the event of total occlusion.
Creston, in 19645, published the occurrence of external ear canal collapse in 2 children aged 6 and 9 years. The author observed in both of them an improvement in thresholds obtained for air conduction when a delicate plastic tube was placed in both ears, producing increases in thresholds of 15dbHL in one and 25 to 40dBHL in the other child.
In another study, Creston, in 19656, observed the incidence of collapsed external ear canal during audiological test of 282 children aged between 6 and 9 years. The author found an incidence of 3.5% worsening of auditory thresholds as a result of external ear canal collapse. Creston emphasized that this condition is more frequent than suspected by audiologists and otorhinolaryngologists.
Ross and Tucker, in 196515, published the audiological findings of a 57 year-old woman, showing incompatibility between pure tone air conduction audiometry and conversation performance. Otoscopy revealed a very narrow external ear canal. Audiometric tests conducted after the insertion of a plastic tube in the ear canals produced an improvement between 5 and 30dBHL in thresholds of air conduction, and the most significant improvement was felt at 4,000Hz.
Stark, in 196618, evaluated hearing of a 4 -year-old boy who failed in pure tone audiometry in the right ear. Conditioned audiometry showed a 10 to 25dbHL gap in all frequencies. Insertion of a rubber part in the ear canal produced an improvement of air conduction of 5 to 25 dBHL in many frequencies. According to the authors, a significant indication of the presence of collapse was not inconsistency of results, but rather the presence oistapedial reflex and air-bone gap. This author recommended a mandatory inspection of external ear canal before audiological assessment, regardless of patient's age.
Smith, in 196619, suggested that before the performance of the exam, all patients should be inspected as to the possibility of collapse of external ear canal by pressing the pinna against the head. If the external ear canal seemed to collapse, some kind of device would be inserted in the canal before the audiological assessment. The author observed that external ear canal collapse may also be associated with tympanic membrane perforation, in which results are substantially worse than expected. The author also cautioned to the fact that patients who have conductive hearing losses may also experience external ear canal collapse.
Chaiklin and McClellan, in 19712, used different methods to determine the best procedure to identify external ear canal collapse and their effects on auditory thresholds of different frequencies. The authors stated that visual inspection is not enough to identify collapse because it is difficult to visualize occlusion. In addition, they determined that the use of instruments (such as plastic tubes, rubber devices, gauze pads placed in the ear) or earphones slightly away from the pinna were poor methods to measure the decrease of thresholds caused by collapse. The authors concluded that free field audiometry or the use of circumaural (NAF) phones were the most acceptable methods in the case.
In 1975, Pearlman12 described in his study the use of small pieces of polyethylene tubes inserted in the entry of external ear canal, enabling sound to reach the tympanic membrane despite the pressure made by the phones on the pinna. The method was successfully used by patients of all ages. There were no auditory artifacts obtained with the use of the technique and the pseudo-conductive hearing losses that occurred without the use of these tubes were eliminated.
Reidner and Schimuzu, in 197614, explored the effects of collapse on the measures of acoustic reflex and they considered the use of circumaural phones an effective option. In the same study, in order to determine the influence of ear canal collapse on auditory thresholds, circumaural phones were used to activate a non-collapse state. The authors suggested the use of correction values for each frequency since there are acoustic modifications resultant from the increased volume of the ear when this kind of cushion is used if compared to the volume of the ear when regular supra-aural phones are used. The authors also suggested that not only hearing thresholds are subject to the effects of ear canal collapse, but also stapedial reflex results may be hindered by it.
Schow and Goldbaum, in 198016, also compared the use of supra-aural and circumaural phones and found the greatest differences between the two conditions in frequencies between 1,000 and 4,000Hz. The authors considered presence of collapse when there was a difference in auditory thresholds of 15dBHL or higher. In the same study, 41% of the subjects who had suggestive results of external ear canal collapse in one or both ears were people older than 80 years, a number much higher than the one obtained for younger subjects. The authors suggested the comparison of the gap between air and bone conduction and the presence of stapedial reflex as supplementary for the detection of collapse.
Schow and Nerbonne, also in 198017, studied the occurrence of collapse in elderly patients (between 60 and 90 years of age). The authors questioned if the increase in hearing loss in the population was due to aging or if it was a consequence of more cases of external ear canal collapse. The authors suggested that the use of circumaural phones, instead of supra-aural ones in this population would be indicated, since it may reduce the occurrence of collapse because it applies less pressure on the pinna.
Marshall and Grossman, in 198211, conducted a study aiming at finding strategies that would minimize the effects of collapse to a smaller degree of variation. They concluded that the use of circumaural phones was the best technique to attenuate the effects of ear canal collapse, because it resulted in lower thresholds for most of the frequencies. However, authors suggested some disadvantages, such as non-standardization for calibration of this type of phone and the fact that they do not produce such high levels of intensity as the supra-aural one, what makes measuring of more severe losses a difficult process. According to the authors, changes in threshold as a result of external ear canal collapse may reach 30dBHL and the use of circumaural phones, despite its limitations, may be the practical solution to solve these effects.
Randolph and Schow, in 198313, evaluated subjects aged between 20 and 79 years using circumaural and supra-aural phones. If the differences in thresholds for both conditions were 15dBHL or higher at any frequency, the presence of collapse was questioned. Out of the total number of studied subjects, 36% showed differences in thresholds of 15dBHL or higher in at least one ear (4 subjects had alterations in both ears). Collapse was observed in all frequencies; however, it was less common in the frequency of 2,000Hz. In most cases, only one frequency was involved and the elderly population was more affected.
Mahony and Luxon, in 199610, described 2 patients who had elevated auditory thresholds as a result of external ear canal collapse, and were then submitted to an examination with a speculum introduced in the external ear canal. Therefore, the air -bone gap noticed in the first assessment was eliminated. In the study, since there was the doubt whether thresholds could be worsened by the use of the speculum, this issue was carefully observed. As a result, the authors showed worsening of air conduction thresholds for frequencies 250 and 8,000Hz in 78% and 82%, respectively. In the other frequencies, auditory thresholds worsening was not noticed.
MATERIAL AND METHODS
This study was conducted in the Division of Clinical Audiology of the Department of Otorhinolaryngology at Santa Casa de Misericórdia de Sao Paulo, between July 1998 and December 1999.
Patients were initially submitted to a complete audiological exam (pure tone air and bone audiometry, speech audiometry and immitanciometry).
After the insertion of a small polyethylene tube in the external ear canal, we retested the patients who had:
o air-bone gap higher than 10dBHL and presence of stapedial reflex;
o sudden fall of air thresholds in frequencies 6,000 and/or 8,000Hz higher than 25dBHL compared to the previous frequency.
Ages ranged from 10 to 87 years.
During testing, we used supra-aural phones (MX41).
We considered improvement of auditory thresholds for air conduction and speech recognition when the difference obtained for the two conditions (with and without polyethylene tube inserted in the canal) was higher than 10dBHL.
This study describes the alterations of auditory thresholds of 47 subjects who had improvement of thresholds when retested with polyethylene tubes inserted in the external ear canal to avoid the effects of collapse.
RESULTS
Out of 47 studied subjects, 13 (27.5%) demonstrated a sudden drop of pure tone thresholds for 6.000 and/or 8.000 Hz which was higher than 25 dBHL, in one or both ears; for this reason, they were retested with a polyethylene tube inserted in the external ear canal. The improvement of auditory thresholds under these conditions amounted to 10 to 40 dBHL.
The remaining 34 subjects (72,5%) had air-bone gap in at least one ear and presence of stapedial reflex; for this reason, they were retested with a polyethylene tube inserted in the external ear canal. Under these conditions, auditory thresholds had an improvement of 10 to 50dBHL and speech recognition thresholds improved up to 30dBHL.
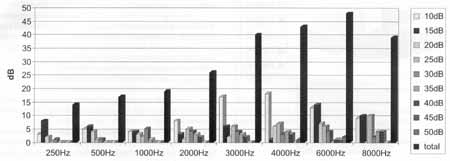
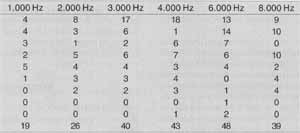
Analyzing the improvement of hearing thresholds per ear obtained with the polyethylene tube, we observed that the frequency with highest incidence of improvement of auditory thresholds was 6.000 Hz, with 48 ears showing improvement of threshold, and 13 ears had improvement of 10 dBHL, 14 of 15 dBHL, 7 of 26 dBHL, 6 of 25 dBHL, 4 of 30 dBHL, 1 of 40 dBHL, 1 of 45 dBHL, and one reached an improvement of 50 dBHL.
With an equally high incidence of improvement of auditory threshold after the insertion of polyethylene tube in the external ear canal, we found the frequency of 4.000Hz, with a total of 43 ears, divided into 18 ears with improvement of 10 dBHL,1 of 15 dBHL, 6 of 20 dBHL, 7 of 25 dBHL, 3 of 30 dBHL, 4 of 35 dBHL, 3 of 40 dBHL and one with improvement of 50 dBHL.
The frequency of 3,000 Hz also showed a large number of ears with improvement of thresholds in the retest, with a total of 40 ears, divided into 17 that presented improvement of 10dBHL, 6 of 15dBHL, 2 of 20 dBHL, 6 of 25 dBHL, 4 of 30 dBHL, 3 of 35 dBHL and 2 ears showed improvement of 40 dBHL.
In 8,000 Hz we observed 39 ears with improvement of auditory threshold: 9 ears presented improvement of 10 dBHL, 10 of 15 dBHL, 10 of 25 dBHL, 2 of 30 dBHL, 4 of 35 dBHL and 4 ears showed 40 dBHL hearing level improvement.
For 2,000 Hz, the number of ears that modified auditory thresholds after the retest was significantly high: 26 ears, divided into 8 that improved 10 dBHL, 3,15 dBHL,1, 20 dBHL, 5, 25 dBHL, 4, 30 dBHL, 3, 35 dBHL and 2 ears improved 40 dBHL.
Despite the fact that it is rarely described in the literature, we observed a significant number of ears that showed improvement of thresholds in 1.000 Hz (total of 19 ears), divided into 4 that presented improvement of 10 dBHL, 4 of 15 dBHL, 3 of 20 dBHL, 2 of 25 dBHL, 5 of 30 dBHL and 1 of 35 dBHL; in 506Hz totaling 17 ears: 5 had improvement of 10 dBHL, 6 of 15 dBHL, 4 of 20 dBHL, 1 of 25 dBHL and 1 of 30 dBHL; and finally, in the frequency of 250 Hz, out of a total of 14 ears, 3 had improvement of 10 dBHL, 8 ears of 15 dBHL, 2 ears of 20 dBHL and 1 ear of 30 dBHL.
Graph 1 shows the variations of auditory thresholds, according to frequency range, with insertion of polyethylene tube in external ear canal.
As observed, there was a considerable improvement in hearing thresholds when they were retested in a way that the effects of external ear canal collapse were minimized.
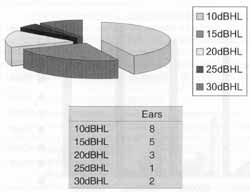
As to thresholds of speech recognition, we noticed that 8 ears had an improvement of 10 dBHL, 5 ears of 15 dBHL, 3 ears of 20 dBHL, 1 ear of 25 dBHL and 1 ear of 30 dBHL, when retested with polyethylene tube.
Graph 2 presents the variations of thresholds of speech recognition when retested with the polyethylene tube inserted in the external ear canal.
DISCUSSION
Incorrect positioning of phones during audiological assessment may lead to false auditory thresholds in all frequencies.
This mistake in determining hearing thresholds may result from both collapse of external ear canal or incorrect positioning of phones and consequent escape of sound pressure.
Factors such as the pressure made by the phones, size of head and configuration and size of external ear may account for these alterations (Zwislocki et al., in 198822; Burkhard and Corllis, in 19541; Erber, in 19687; Villchur, in 197021).
Graph 1. Variation of hearing thresholds in dBHL according to frequency range
Many researchers (Chandler, in 19643; Creston, in 19645; Hildyard and Valentine, in 19628; Ventry, Chaiklin and Boyle, in 196120) demonstrated that the pressure exerted by the phones on the pinna may cause a false air-bone gap. The occurrence of external ear canal collapse may be questioned when we come across:
o patients without hearing complaints;
o patients without history of inner ear affections or hearing loss;
o patients without evidence of middle ear affection or hearing loss;
o extremely protuberant pinna that could be easily pressed by the use of phones, resulting in closure of external ear canal, and
o extremely narrow external ear canal.
Many strategies have been suggested to solve the problem of external ear canal collapse, including the use of circumaural phones, which do not press the pinna, insertion of tubes, speculums, molds, etc. in the external ear canal to keep it free; as well as the use of gauze pads placed behind the pinna. These methods are fast and simple, however we sometimes observe narrow and tortuous canals, followed or not by extremely flaccid pinna, which do not respond well to these methods, maintaining the ear collapse during the assessment.
The introduction of a speculum in the external ear canal may interfere in its natural resonance, leading to reduction of hearing thresholds. Chaiklin and McClellan, em 19712, suggested that the use of this type of instrument could be effective for many subjects who have external ear canal collapse, however its insertion may also lead to reduction of auditory thresholds.
Graph 2. Variation of speech recognition thresholds in dBHL.
Another alternative is the use of circumaural phones that apply pressure on the head rather than on the pinna (Marshall and Grossman, in 198211) or of insertion phones that would also help minimize the effects of collapsed ear, despite the fact that this resource brings about other difficulties, such as calibration, limited testing of high frequency, and hygiene (Zwislocki et al., in 198822; Killion and Villchur, in 19899). Supra-aural phones (TDH-39 with MX-41) are the most widely used and they have the advantage of easy calibration; nevertheless, these phones press intensively the pinna, favoring the occurrence of collapsed ear in more susceptible patients.
A third strategy also used by various authors would be the insertion of different instruments in the external ear canal to maintain it free (Ventry et al., in 196120; Coles, in 19674; Marshall and Grossman, in 19821'; Mahoney and Luxon, in 199610). However, this kind of procedure may result in minor mistakes because of the modification of the natural resonance of external ear canal, despite the fact that the magnitude of these mistakes do not mask the benefits of this kind of procedure.
CONCLUSION
Collapse of external ear canal is much more frequent than we expect; that is why it should be taken into consideration during the audiological assessment.
Since there is the likelihood of producing a wrong diagnosis if the audiometric findings are incorrect, all patients should be checked, verifying the existence of collapsed external ear canal before the exam begins. It may be easily done by pressing the pinna against the head.
Although the collapse is easily observed in the presence of air-bone gap and positive stapedial reflex, we should not consider it as affecting only high frequencies.
As observed, the problem of external ear canal collapse is not limited to specific age ranges and it should be investigated in all cases presenting air-bone gap and presence of stapedial reflex and/or incompatibility between subjective impressions and the results of audiological assessment.
Another key issue is the fact that although collapse is frequently seen in high frequencies, it may be present in all frequency ranges.
It is important to highlight that the occurrence of external ear canal collapse is not restricted to sensorineural hearing losses - in fact, it may be present in subjects who have conductive hearing loss.
Many methods have been suggested, but the use of polyethylene tubes has advantages because it is easily introduced in the external ear canal, it does not require another examiner to help insertion and despite evidence suggesting that it modifies the natural resonance of the external ear canal, its benefits exceed the disadvantages (differences of hearing thresholds obtained with and without insertion of polyethylene tube reached 50dBHL).
REFERENCES
1. BURKHARD, M. D.; CORLLIS, E. L. R. - The response of ear phones in ears and couplers. J. Acoust. Soc. Am., 26 (5): 679685, 1954.
2. CHAIKLIN, J. B.; McCLELLAN, M. E. -Audiometry management of collapsible ear canals. Arch. Otolaryngol., 93:397-407, 1971.
3. CHANDLER, J. R. - Partial occlusion of the external auditory meatus; its effect upon air and bone conduction hearing acuity. Laryngoscope, 74: 22-54, 1964.
4. COLES, R. - External meatus closure by audiometer earphone. J. Speech Hear Disord, 32: 296-297, 1967.
5. CRESTON, J. E. - Collapse of the ear canal during audiometry. Arch. Otolaryngol., 79:389-392, 1964.
6. CRESTON, J. E. - Collapse of the ear canal during routine audiometry. J. Laryngol., 79: 893-901, 1965.
7. ERBER, N. P - Variables that influence sound pressures generated in the ear canal by audiometric earphone. J. Acoust. Soc. Am., 44 (2): 555-562, 1968.
8. HILDYARD, V.; VALENTINE, M. - Collapse of the ear canal during audiometry. Arch. Otolaryngol., 75: 422-423, 1962.
9. KILLION, M. C., VILLCHUR, E - Comments on earphones in audiometry. J. Acoust. Soc. Am., 85'(4): 1775-1779, 1989.
10. MAHONEY, C. F. O; LUXON, L. M. - Misdiagnosis of hearing loss due to ear canal collapse: a report of two cases. J. Laryngol. Otol., 110: 561-566, 1996.
11. MARSHALL, L.; GROSSMAN, M. A - Management of ear canal collapse. Arch. Otolaryngol., 108: 357-361, 1982.
12. PEARLMAN, R. C. - Preventing collapse of external auditory meatus during audiometry. Arch. Otolaryngol., 101: 686-688, 1975.
13. RANDOLPH, L. J.; SCHOW, R. L. -Threshold in accuracy in an elderly clinical population: ear canal collapse as a possible cause. J. Speech. Hear Res., 26. 54-58, 1983.
14. RIEDNER, E.; SHIMIZU, H. - Collapsing ears and acoustic reflex measurement with circumaural ear cushions. Arch. Otolaryngol., 102 358-362, 1976.
15. ROSS, M.; TUCKER, C. A. - A case study of collapse of the ear canal during audiometry. Laryngoscope, 75: 65-67, 1965.
16. SCHOW, R. L.; GOLDBAUM, D. E. -Collapsed ear canals in the elderly nursing home population. J. Speech Hear Disord, 45: 259-267, 1980.
17. SCHOW, R. L.; NERBONNE, M. A - Hearing levels among elderly nursing home residents. J. Speech Hear Disord, 45:124-132, 1980.
18. STARK, E. W. - Collapse of the ear canal during audiometry: a case report. J. Speech Hear Disord, 31: 374-376, 1996.
19. SMITH, C. - Collapsing ear canals. J. Speech Hear Res., 9: 317, 1966.
20. VENTRY, I. M.; CHAIKLIN, J. B.; BOYLE, W. F. - Collapse of the ear canal during audiometry. Arch. Otolaryngol., 73: 727-731, 1961.
21. VILLCHUR, E. - Audiometer earphone mounting to improve intersubject and cushion fit reliability. J. Acoust. Soc. Am., 48: 1387-1396, 1970.
22. ZWISLOCKI, et al. -J. Acoust. Soc. Am., 83:1688-1689, 1988.
* Speech and Hearing Pathologist, Specialization in Clinical Audiology under course at the Department of Otorhinolaryngologist, Irmandade da Santa Casa de Misericórdia de Sao Paulo.
** Head of the Division of Clinical Audiology at Irmandade da Santa Casa de Misericórdia de São Paulo.
*** Faculty Professor of Otorhinolaryngology at Faculdade de Ciências Medicas da Santa Casa de São Paulo.
Study conducted at the Department of Otorhinolaryngology, Faculdade de Ciências Medicas da Santa Casa de São Paulo and Irmandade da Santa Casa de Miseric6rdia de São Paulo.
Article submitted on September 28, 2000. Article accepted on October 6, 2000.
Print: ![]()