

Year: 2000 Vol. 66 Ed. 6 - (11º)
Artigos Originais
Pages: 644 to 648
Does Pure Tone Threshold Audiometry and/or Behavorial Auditory Assessment Confirm Subsequent Response Obtained Precociously in Children with Auditive Deficiency?
Author(s):
Raquel G. Lemos*,
Pedro L. Cóser**,
Claudio Cechella***.
Keywords: audiology, hearing tests, deafness in child, audiometry, auditory brainstem responses
Abstract:
Aim: This research was made after survey of the audiologics diagnostics obtained through of the auditory brainstem response (ABR), pure tone threshold audiometry (PTA) and/or behavioral auditory assessment (BAA) made in 30 children with auditive deficiency with the purpose of to compare and Check the agreement between them. Results: In the comparison of the diagnostics of the grades of hearing loss obtained watched a agreement of 97,30% of the diagnostics in the hearing losses of profound grade, 77,78% in the severe grade, 57,15% in the moderate grade and 33,33% in the moderately-severe; in general, of the clinical point of view, watched diagnostic agreement in 57 (95,00%) of the 60 ears researched.
![]()
INTRODUCTION
Early detection of hearing loss is essential for diagnosis and management of human communication disorders in children and it has been emphasized by different authors for years (Katz, 1989; Santos and Russo, 1989; Northen and Downs, 1991; Oliveira, 1994; Oliveira, Azevedo, Vieira andAvila, 1995; Azevedo, Vieira and Vilanova, 1995).
Hearing impairment detected at the first years of life enables early auditory habilitation, and probably, better quality of life to the child.
To perform audiological assessment, there are objective procedures, such as brainstem audiometry, evoked otoacoustic emissions, and immitanciometry, in addition to subjective methods, such as behavioral audiometry with instruments and pure tone audiometry.
The use of more than one diagnostic technique combining objective and subjective procedures guarantees more consistent results.
Brackmann and Froquer (1983) presented a strategy to evaluate young children or those who do not cooperate in regular behavioral methods, and considered evoked brainstem response combined with immitanciometry and behavioral tests as the preferred choice for this kind of situation.
Based on that, this study aimed at comparing the results obtained with evoked brainstem response (ABR) conducted early in life to the results obtained with pure tone audiometry or behavioral audiometry performed years later in 30 hearing impaired children treated at the Service of Educational Audiology at Universidade Federal de Santa Maria, to check if the estimates of hearing loss level determined by ABR were confirmed by conventional audiological tests conducted some time later.
MATERIAL AND METHOD
This study was conducted based on the audiological diagnoses concluded by ABR, pure tone audiometry (PTA) and behavioral audiometry (BA) in 30 children with hearing impairment treated at the Service of Educational Audiology at Universidade Federal de Santa Maria.
Out of 30 studied children, 14 were male and 16 were female patients, ages ranging from 1 month to 9 years and 11 months.
All children had been submitted to ABR, 17 had undergone PTA and 13 were submitted only to BA, because they were not able to respond to pure tone audiometry. At the time of the study, most of the children were aged between 7 and 9 years; at the time of ABR, they were between 1 and 3 years; at the time of PTA, between 5 and 7 years, and at the time of BA they were between 3 and 5 years.
ABR had been conducted in an ENT clinic, according the criteria proposed by Jewett (1970); pure tone audiometry had been performed in the Service of Audiology at Universidade Federal de Santa Maria, according to the psychometric method of limits of Katz (1989 and 1994), and behavioral audiometry, as suggested by Eisenberg (1965), Downs (1971), Taylor an Mencher (1972), Northen and Downs (1991), Russo and Santos (1989 and 1991) and Oliveira (1994).
Both for ABR and PTA, levels of hearing loss wee classified according to Davis and Silvermann (1970) criteria:
1) mild loss: minimum response level between 26 and 4 dB;
2) moderate loss: minimum response level between 41 and 5 dB;
3) moderately severe loss: minimum response level betwee 56 and 70 dB;
4) severe loss: minimum response level between 71 and 9 dB;
5) profound loss: minimum response levels exceeding 90 dl In order to compare diagnosis of hearing loss obtained b ABA and PTA and BA, we used the arithmetic average of the minimal level of response to a click and tone pip of 1,000H at ABR and the mean thresholds of frequencies 1,000, 2,000 an 4,000Hz at PTA. In 3 ears, we did not obtain responses to on stimulus of ABR, so we added 10 dB to the maximum of the equipment (85dB) and calculated the average, amounting to 90dB.
To check diagnostic agreement of the exams we used the statistical method of Student t test, at the level of 1%, for independent sample differences.
RESULT AND DISCUSSION
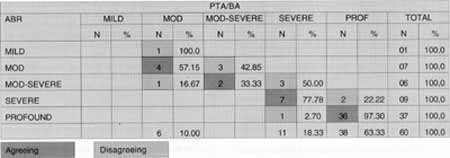
For the comparative study between the diagnoses c level of hearing loss obtained with ABR and those of PTA any BA we crossed and compiled data, according to level of loss (Chart 1).
The results of distribution of agreeing and disagreeing audiological diagnoses, according to side of ear, are shown in Table 1, and its distribution, according to side o ear and level of hearing loss in shown in Table 2. The result of Student t test, applied to the values of Table 2, are show in Table 3. .
Based on the analysis of results of Chart 1, we may stag that out of 60 studied ears, 49 had agreeing diagnosis as to level of hearing loss and 11 had a disagreeing diagnosis.
Out of 11 ears with disagreeing diagnosis, 10 had level of hearing loss determined by ABR at the immediately adjacent level determined by PTA, and in 9 cases the estimate of hearing loss determined by ABR was less intense than the estimates by PTA. In only one ear, the level of hearing loss was immediately adjacent, but ABR had established a more severe level than PTA. In this case, ABR is being confronted with PTA (subject 8) and maybe we should give more credit to this test because it covers a larger number of frequencies than ABR. In the only disagreeing case, in which ABR was compared to BA (subject 18), we observed more severe hearing loss in A,BR than BA, probably because the patient had a better hearing reserve in low frequencies.CHART 1 - Distribution of occurrence of agreeing and disagreeing diagnoses of hearing loss with ABR and PTA or BA.
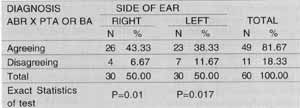
TABLE 1 - Distribution of agreeing and disagreeing diagnoses according to side of ear.
The differences in decibels (dB) between the mean of click and tone pip of 1,000 Hz at ABR and the mean frequencies of 1,000, 2,000 and 4,000 Hz of PTA varied from 5 to 30 dB.
In the case of subjects 2, 3, 8, 13 and 14, differences in decibels were, respectively, 6 dB, 5 dB, 11 dB, 6 dB and 13,3 dB in the disagreeing ear; in subject 30, differences were 16.6 dB and 13.3 dB in the right ear and left ear, respectively. These differences were considered small from a clinical and therapeutic point of view, however, they were enough according to the criteria adopted to change the classification of level of hearing loss, resulting in disagreeing diagnoses of these ears. Taking into account the small difference in decibels; we considered this disagreement irrelevant from the clinical point of view.
In subject 10, there was a difference of 20B between ABR, which classified the hearing loss as mild, and the PTA, which classified it as moderate. This patient has the diagnosis of Usher syndrome and clinically she experienced worsening of loss at the time of ABR and PTA; therefore, there was no disagreement in the results but rather a characteristic evolution of the syndrome, with worsening of hearing.
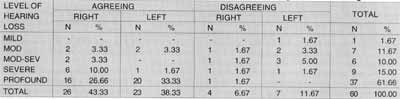
In case 9, we observed a difference of 30 dB between ABR and PTA in-the right ear, and 35dB in the left ear, and the result of ABR was again better than that of PTA. The patient was 5y6m when he was submitted to the last PTA; therefore, we may conclude that either the patient was not conditioned to respond to PTA or there was, in fact, a diagnostic, mistake in ABR.TABLE 2 - Distribution of agreeing and disagreeing diagnoses per ear, according to level of hearing loss.
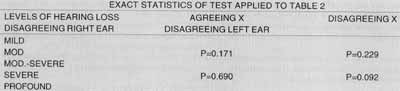
TABLE 3 - Exact statistics of Student's t test applied to values of Table 2.
In subject 18, in the right ear, we observed profound loss at ABR and severe at BA. This subject was 3 years and 11 months and was not able to respond to PTA and at BA he responded as having a profound loss in the left and a severe one in the right side. This disagreement may be due to a better hearing reserve in low frequencies, since this region is not assessed by ABR.
Out of 11 ears with disagreeing diagnoses, 7 had clinical disagreements (differences of mean of 1,000, 2,000 and 4,000 Hz at PTA and means of click and tone pip of 1.000 Hz at ABR between 5 and 16.6 dB), one ear had disagreeing diagnosis because of actual worsening of hearing and only 3 ears showed real disagreement between diagnoses obtained from the tests.
These results are in accordance with the literature that suggested a standard deviation of 15dB for responses to click when compared to the mean of 1,000, 2,000 and 4,000 Hz of PTA (Jerger and Mauldin, 1978) or thresholds varying from -10 and +20 dB, as found by Stapells, Picton, Durieux-Smith, Edwards and Moran (1990). Brackmann a Froquer (1983), suggested the use of click combined with a tone pip of 1,000Hz in order to learn more about low frequencies.
The results of the comparison of agreeing and disagreeing diagnoses obtained with ABR and PTA and BA, according to side, are shown in Table 1, in which we may observe that most of the ears (81.67%) diagnoses agreed and in 18.33% they disagreed.
In order to check the existence or not of statistically significant difference among disagreeing and agreeing diagnoses, considering the side, we used Student t test at the level of significance of 1% and we found that the value of p among agreeing and disagreeing diagnoses in the right ear was 0.01 (1%), and in the left ear it was 0.017 (1.7%), accepting the hypothesis H, that is, although there was a great difference in the number of agreeing and disagreeing exams, the statistical test did not produce statistically significant difference, a fact that might be explained by the small sample.
The results of the comparison of diagnoses obtained with ABR and PTA, or BA, according to different levels of hearing loss and side, are exposed in Table 2 and the results of Student t test are shown in Table 3.
The results of Table 2 show that in 59.99% of all examined ears the diagnosis of profound hearing loss made by ABR agreed with the diagnosis made by PTA and BA, and in only 1.67% of them there was diagnostic disagreement. In 11.67% of all examined ears, the diagnosis of severe hearing loss defined by ABR agreed with the diagnosis made by PTA and BA, and in only 3.33% of the cases there was diagnostic disagreement. In 3.33% of all examined ears, the diagnosis of moderately severe hearing loss defined by ABR agreed with the diagnosis made by PTA and BA, and in only 6.67% of the cases there was diagnostic disagreement. In 6.66% of all examined ears, the diagnosis of moderate hearing loss defined by ABR agreed with the diagnosis made by PTA and BA, and in only 5.00% of the cases there was diagnostic disagreement. In 1.67% of all examined ears, the diagnosis of mild hearing loss defined by ABR disagreed with the diagnosis made by PTA and BA.
In order to check whether there was statistically significant difference among agreeing and disagreeing diagnoses, considering the level of hearing loss, we used Student t test for a level of significance of 1% and we confirmed that the value of p for agreeing and disagreeing diagnoses in the right side, moderate level, was p = 0.171 (17.1%); for severe level it was p=0.690 (69.0%); in the left ear, p=0.229 (22.9%) for moderate level; and in severe level, p= 0.092 (9.2%). All these p values confirm the hypothesis Ho, that is to say, the results of the statistical analysis were not statistically significant regardless of the level of hearing loss. This fact might be explained by the small sample.
Generally speaking, both from a clinical and a statistical perspective, diagnoses of level of hearing loss determined by ABR agreed with those defined by PTA or BA.
A CONCLUSION
At the end of this study that aimed at checking the reliability of evoked brainstem response using clicks and tone pips of 1,000Hz, conducted early and confronted with pure tone audiometry (PTA) or behavioral audiometry (BA) performed years later, in a sample of 30 hearing impaired children, we concluded that:
o Evoked Brainstem Response conducted at an age in which pure tone audiometry is impossible to be performed, or when behavioral audiometry is not perfectly clear, is highly reliable because diagnoses were confirmed in 57 (95%) out of the 60 tested ears.
REFERENCES
AZEVEDO, M. F.; VILANOVA, L. C. P.; CARVALHO, R. M. M.; GARCIA, V. L. & FUJINAMI, A. A. - Rubéola congenita: caracterização dos aspectos clínicos a audiológicos. Acta AWHO, 8 (3): 97-104, 1989.
AZEVEDO, M. F.; VIEIRA, R. M. & VILANOVA, L. C. P.- Desenvolvimento auditivo de crianças normais a de alto risco. Sao Paulo, PLEXUS, 1995.
BRACKMANN, D. E. & FROQUER, D. B. - Evaluation of the auditory system: an Update. Ann. Otol. Rhinol. Laryngol. (92): 651-6, 1983.
DAVIS, H. & SILVERMAN, S. R. - Hearing and deafness, 3ª ed., New York, HOLT, RINENHART & WINSTON, 1970.
DOWNS, M. P. - Audiological evaluation of the congenitally deaf infant. Otolaryngol. Clin. North. Am., 4(2): 347-58, 1971.
EISENBERG, R. B. - Auditory behavior in the human neonate: I. methodological problems and the logical design of research procedures. J. Audiol. Res., 5(2): 159-77, 1965.
JERGER, J. & MAULDIN, L. - Prediction sensorineural hearing level from the brain stem evoked response. Arch. Otolaryng., (204): 456-61, 1978.
JEWETT, D. L. - Volume conducted potentials in response to auditory stimuli as detected by averaging in the cat. EEG and Clinical Neurophysiology, (28): 609-18, 1970.
KATZ, J. -Tratado de Audiologia Clinica., 3ª ed., MANOLE, 1989_____, Handbook of Clinical Audiology., 4ª ed. , BALTIMORE, 1994.
NORTHEN. J. L. & DOWNS, M. P. - Hearing in children, 4ª ed., BALTIMORE, 1991. 417 p.
OLIVEIRA, T. T. - Triagem auditiva com sons não calibrados: detecção precoce da deficiência auditiva infantil. Santa Maria, 1994. [TESE DE MESTRADO].
RUSSO, I. C. & SANTOS, T. M., - Audiologia infantil: princípios e métodos de avaliação na criança. 3ª ed., São Paulo, CORTEZ; 1989.
______ -A prática da audiologia clínica. 3ª ed., São Paulo, CORTEZ, 1991.
STAPELLS, D. R.; PICTON, T.W.; DURIEX-SMITH, A.; EDWARDS, C. G. & MORAN, L. M. - Thresholds for short-latency auditory-evoked potentials to tones in notched noise in normal hearing and hearing-impaired subjects. Audiology, 29(5): 262-74, 1990.
TAYLOR, D. J. & MENCHER, G. T. - Neonate response - The effect on infant state and auditory stimuli. Arch. Otolaryngol., (95):120-4, 1972.
* Speech and Hearing Pathologist, Specialized in Speech and Language Therapy at Universidade Federal de Santa Maria.
** Otorhinolaryngologist, Ph.D. in Human Communication Disorders, Universidade Federal de Sao Paulo - Escola Paulista de Medicina, Joint Professor of the Department of
Otorhinolaryngology and Speech and Hearing Pathology at Universidade Federal de Santa Maria.
*** Neurologist, Master and Assistant Professor of the Department of Otorhinolaryngology and Speech and Hearing Pathology at Universidade Federal de Santa Maria.
Address for correspondence: Raquel Guidotti Lemos - Rua Tamandare, 1029 - Apt°. 146 - Aclimação - 01525-001 São Paulo/ SP - Tel: (55 11) 3272-3854.
Article submitted on August 30, 2000. Article accepted on September 28, 2000.
Print: ![]()