

Year: 2000 Vol. 66 Ed. 6 - (3º)
Artigos Originais
Pages: 592 to 596
Lateral Teleradiograph of Cranium and Lateral Radiograph of the Nasopharynx: Comparative Study in Children with Nasal Obstruction.
Author(s):
Cláudio M. Y. Ikino*,
Walmir E. P. A. D'Antonio*,
Rodrigo A. C. de la Cortina*,
Marcus Lessa**,
Arthur M. Castilho**,
Elder Y. Goto**,
Ossamu Butugan***,
Terezinha S. Amaral ****.
Keywords: adenoid, nasopharyngeal airway, nasal obstruction, radiology
Abstract:
Introduction: Nasal obstruction is a common complaint in daily practice and adenoidal obstruction is one of the main causes of that in childhood. Radiological assessment constitutes a noninvasive, generally available and objective means of estimating the nasopharynx airway. Some authors describe correlations among radiographic evaluation, clinical and intraoperative findings. Purpose: This study intends to compare lateral teleradiograph of cranium (LTC) and lateral radiograph of the nasopharynx (LRN) in the evaluation of nasal obstruction children. Material e methods: We studied 26 patients between 3 to 11 years old with nasal obstruction and/or mouth breathing for more than 3 months. Both radiographs were taken in the same day and they were evaluated by Cohen and Konak approach. Results: The mean age was 6.4 years and 16 patients were female and 10 male. We found the some interpretation in both radiographs in 73.1% of children. 61.5% of the LRN presented head rotation in the sagital plane. Conclusion: Authors conclude LTC is the radiograph of choice in the nasal obstruction children approach because it evaluates the nasopharynx airway as the LRN but it minimizes changes in head positioning.
![]()
INTRODUCTION
Nasal obstruction is a frequent complaint in our daily ENT practice. In children, especially those aged 4 to 15 years9, the main cause is hypertrophy of pharyngeal tonsil (adenoids)8. The diagnosis of this affection requires anamnesis and physical exam, and sometimes it is necessary to complement the investigation with subsidiary exams, such as radiological1, 2, 7, 12 and endoscopic12 exams.
One important aspect to be mentioned is that the symptoms of patients with adenoid hypertrophy and the indication of adenoidectomy because of obstructive condition are based on impairment of permeability of the nasal part of pharynx (rhinopharynx) and not on the absolute size of adenoid1, 3, 6, 9.
Nasal endoscopy, both flexible and rigid, enables direct visualization of the nasal part of the pharynx, allowing the evaluation of the size of adenoids and the compromise of the airways by the adenoid. However, this exam is not completely accessible, especially if we consider the status of public health in our country, and, in addition, it is an invasive exam, which may be traumatic and difficult to perform in a patient that does not collaborate2, 12. Radiological assessment is a noninvasive exam, more accessible and it allows objective evaluation of dimensions of adenoid and compromise of airways1-12.
Among all types of radiological exams, we point out the importance of nasopharynx radiograph and lateral teleradiograph of the head. Nasopharynx radiograph is the most widely used exam to evaluate patients with nasal obstruction, aiming at checking the nasal portion of the pharynx. Lateral teleradiograph of the head is a radiological technique that has been used for many years in odontology to evaluate dental occlusion and upper airways and it has now been used by otorhinolaryngologists to evaluate patients with sleep obstructive apnea. In addition, various authors have shown that the technique allows investigation of adenoid and nasopharynx; however, it requires the use of cephalometric tracings, which have increased the cost of the exam and generated the surge of other evaluation methods3-10.
The objective of this study was to compare lateral teleradiograph of the head without cephalometric tracing and nasopharynx radiograph in children with nasal obstruction, using the method described by Cohen and Konak (1985) 1.
MATERIAL AND METHOD
We conducted a prospective study of 26 children treated at the Division of Clinical Otorhinolaryngology at Hospital das Clinicas, Faculdade de Medicina da Universidade de São Paulo (HCFMUSP), submitted to anamnesis and complete physical otorhinolaryngologic exam, whose main com plaint was nasal obstruction and/or mouth breathing for 3 months. They ranged in age from 3 to 11 years, and they seen in the period between January and August 1999. We ordered nasopharynx radiograph and lateral teleradiograph of the head to all patients, performed in the same day. Nasopharynx radiograph was conducted with the patient standing up, in profile, and the rays were directed to the level of the hard palate. Lateral teleradiograph of the head was conducted similarly but the head was fixed by the cephalostat at the level of the external acoustic canal.
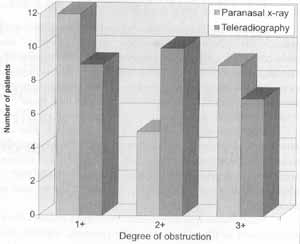
The analysis of exams was conducted by two of the authors (CMYI and WEPAD) at the same time, concluding a single analysis. Exams did not contain the identification of patients and lateral teleradiograph of the head and nasopharynx radiograph of the same patients were seen independently. Both exams were evaluated based on permeability of airways of the nasal portion of pharynx, based on Cohen and Konak1 method: 1+ - thickness of airway larger than of soft palate (1 cm below the upper portion); 2+ - thickness of airway smaller than that of soft palate, but larger than half of its diameter; 3+ thickness of airway smaller than half of the thickness of soft palate. Another fact observed was rotation of the head at the sagittal plan and to be considered "rotated" the exams had to show mandible separation bigger than 3mm.
Statistical analysis used was Qui-square test, with level of significance of 5% (p<0.05).
RESULTS
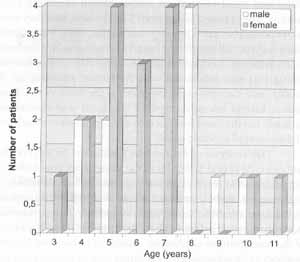
We evaluated 26 children with mean age of 6.4 years, ranging from 3 to 11 years, divided into 16 female and 10 male subjects. Distribution of patients according to age and sex is shown in Figure 1.
Evaluation of the airways according to degree of obstruction in the nasopharynx radiograph and lateral teleradiograph of the head is presented in Figure 2.
There was agreement as to permeability of airways in the nasal portion of pharynx between the two techniques used in 19 (73.1%) patients, and it was statistically significant (x2= 5.538; p<0.02) in the 7 (26.9%) exams in which there was no agreement.
In 16 (61.5%) nasopharynx radiographs there was alteration in the position of patients, that is, they were considered "rotated" exams, but there was no statistically significant difference (x2 = 1.385; 0.1<p<0.2); in 10 (38.5%) nasopharynx radiographs the position was correct. In lateral teleradiograph of the head there was no case of altered position.
In Figures 3 and 4 we show an example of nasopharynx radiograph and lateral teleradiograph of the head, respectively, in which there was coincidence in the evaluation of the airways of the nasal portion of the pharynx. In Figures 5 and 6 we show an example of nasopharynx radiograph and lateral teleradiograph of the head, respectively, in which there is no coincidence in the evaluation of the airway of the nasopharynx.
Figure 1. Distribution of patients according to sex and age.
Figure 2. Assessment of permeability of nasal portion of pharynx.
Figure 3. Radiography of nasopharynx - reduction of airway in the nasal portion of pharynx 1+.
Figure 4. Lateral teleradiograph of the head - reduction of airway in the nasal portion of pharynx 1+.
DISCUSSION
Radiological study of nasopharynx is important as an objective assessment of size of adenoid and permeability of airways9, 10. Paradise et al. (1998) considered the audiological evaluation as golden standard because of generalized access to it, objectivity, noninvasive approach and correlation with the volume of adenoid removed in surgery8. Jeans et al. (1981) compared cephalometric findings with the volume of adenoid removed in surgery and found a correlation between them. Elwany (1987)3 and Kemaloglu et al: (1999)7 compared the clinical findings with cephalometric findings and detected correlation between them. In this study, the authors excluded patients who had other causes of nasal obstruction, such as rhinitis, septum deviation and general unsatisfactory conditions1. Cohen et al. (1992) found correlation between nasopharynx radiograph and intraoperative findings in 85% of the patients2.
Figure 5. Radiography of nasopharynx reduction of airway in the nasal portion of pharynx 3+.
Figure 6. Lateral teleradiograph of the head - reduction of airway in the nasal portion of pharynx 2+.
There are some parameters described for the evaluation of airways and adenoid in radiological exams, most of them cephalometric tracings. However, such methods are not used in daily clinical practice, because they have high cost, are not easily accessible and authors still debate about the different methods described3.
Holmberg and Linder-Aronson (1979) found correlation between size of adenoids, clinical assessment of otorhinolaryngologists and semi-quantitative assessment of lateral teleradiograph of the head5. Cohen and Konak (1985) evaluated the methods of analysis of lateral teleradiograph of the head described by 6 authors (Johannesson, Marau, Fujioka, Hilbert, Sorensen and Crepeau) and concluded that such methods are neither easy nor fast enough to be used routinely, since they involve different tracings and measures that are not always possible to be made, depending on the quality of the x-ray1. Thus, Cohen and Konak (1985) proposed a simpler method of evaluation, based on the analysis of airway in the nasopharynx1. Wornald and Prescott (1992) showed that the radiological evaluation that best correlated with endoscopic findings was the one by Cohen and Konak11.
In our study, we evaluated nasopharynx radiograph and lateral teleradiograph of the head based on Cohen and Konak's method. We found that the evaluation of the airway in the nasal portion of the pharynx coincided in both radiological techniques in 72.1% of the cases. We noticed 61.5% of nasopharynx radiographs that had positioning problems of patients, and although there was no statistically significant difference, it is a marked factor if compared to teleradiograph in which there was no mispositioning. It happened because in lateral teleradiograph of the head the patient stands during the exam, maintains the teeth occluded, lips at rest and the head is fixed by the cephalostat at the level of external ear canal. This fixation maintains the head fixed in a reproducible position and prevents cephalic rotation on the sagittal plan4, 6, 7. Another interesting piece of information is that the cost of the lateral teleradiograph of the head without cephalometric tracings is lower or similar to those of nasopharynx radiograph.
CONCLUSIONS
1. Lateral teleradiograph of the head is as good an exam as nasopharynx radiograph to evaluate the airway of the nasal portion of the pharynx in children.
2. The technique of lateral teleradiograph of the head is better than the one of nasopharynx radiograph, since the head position of the patient is fixed, avoiding variations on the sagittal and transversal plans and enabling a more reliable analysis of the airways, without artifacts produced by rotation of the head. This information is important especially in children that not always maintain the desired positioning.
3. Finally, based on these conclusions, we proposed the use of lateral teleradiograph of the head instead of nasopharynx radiograph in children with nasal obstruction.
REFERENCES
1. COHEN, D.; KONAK, S. - The Evaluation of Radiographs of the Nasopharynx, Clin. Otolaryngol., 10 (2): 73-8, 1985.
2. COHEN, L. M.; KOLTAI, P. J.; SCOTT, J. R. - Lateral Cervical Radiographs and Adenoid Size: Do They Correlate? ENT Journal, 71 (12):638-42, 1992.
3. ELWANY, S. -The Adenoidal-Nasopharyngeal Ratio (NA Ratio), J. Laryngol. Otol., 101: 569-73, 1987.
4. GIOVANETTI, R. A. - Mensuração da Parte Nasal da Faringe em Pacientes com Hipertrofia da Tonsila Faringea. Estudo Cefalometrico em Criança. São Paulo, 1998, 24-77 (Tese de Doutorado - Faculdade de Medicina da Universidade de São Paulo).
5. HOLMBERG, H.; LINDER-ARONSON, S. - Cephalometric Radiographs as a Means of Evaluating the Capacity of the Nasal and Nasopharyngeal Airway, Am. J. Orthod., 76 (S): 479-90, 1979.
6. JEANS, W. D.; FERNANDO, D. C. J.; MAW, A. R. - How Should Adenoidal Enlargement be Measured? A Radiological Study Based on Interobserver Agreement, Clin. Radiol., 32:337-40, 1981.
7. KEMALOGLU, Y. K.; GOKSU, N.; INAL, E.; AKYILDIZ, N. Radiographic Evaluation of Children with Nasopharyngeal Obstruction due to the Adenoid, Ann. Otol. Rhinol. Laryngol., 108:67-72, 1999.
8. PARADISE, J. L.; BERNARD, B. S.; COLBORN, K.; JANOSKY, J. E. -Assessment of Adenoidal Obstruction in Children: Clinical Signs Versus Roentgenographic Findings, Pediatrics, 101(6): 979-86, 1998.
9. POOLE, M. N.; ENGEL, G. A.; CHACONAS, S. J. Nasopharyngeal cephalometrics, Oral. Surg. Oral. Med. Oral. Pathol., 49 (3): 266-71, 1980.
10. WEIMERT, T. A. - Evaluation of the Upper Airway in Children, ENT Journal, 6G 196-200, 1987.
11. WORMALD, P. J.; PRESCOTT, C. A. J. -Adenoids: Comparison of Radiological Assessment Methods with Clinical and Endoscopic Findings, J. Laryngol. Otol., 106: 342-4, 1992.
12. YANAGISAWA, E.; YANAGISAWA, K. - Endoscopic View of Adenoids, ENT Journal, 73 (2): 74-5, 1994.
* Intern Physician of the Division of Clinical Otorhinolaryngology at Hospital das Clinicas, Faculdade de Medicina da Universidade de São Paulo.
** Resident Physician of the Division of Clinical Otorhinolaryngology at Hospital das Clinicas, Faculdade de Medicina da Universidade de São Paulo.
*** Associate Professor of the Discipline of Otorhinolaryngology at Faculdade de Medicina da Universidade de São Paulo.
**** Assistant Dentist of the Division of Odontology at Hospital das Clinicas, Faculdade de Medicina da Universidade de São Paulo.
Study conducted at the Division of Clinical Otorhinolaryngology and Institute of Radiology, at Hospital das Clinicas, Faculdade de Medicina da Universidade de São Paulo.
Address for correspondence: Claudio Marcio Yudi Ikino - Rua Las Palmas, 201 - Americanópolis 04339-000 São Paulo/ SP - Tel: (55 11) 5588-0714 - E-mail: claudioikino@hotmail.com
Article submitted on November 9, 1999. Article accepted on January 19, 2000.




Print: ![]()